Fatal Evolution of an Aortic Ring Abscess in a Multiple Valve Heart Diseases Patient
The aortic ring abscess is a rare and serious complication of infectious endocarditis. Echocardiography remains the diagnostic key, the treatment is expensive and the prognosis is generally dark .we report the case of a 29 years old patient with multiple value diseases who presented an aortic ring abscess.</p> <p>Observation: This is Miss M. D, 29, known with a rheumatic multiple valve disease: a combined mitral and tricuspid disease and an aortic regurgitation for over 15 years, with a history of multiple hospitalizations.</p> <p>At admission, she was in bad condition, suffered significant weight loss, was pale, a congestive heart failure, mitral regurgitation and stenosis signs, aortic regurgitation and pulmonary hypertension on a background of fever in the long course. The biology test noted anon specific inflammatory syndrome and negative blood cultures. Echocardiography showed, in addition to the multiple valve disease, a fluid collection at the valsalva sinus, suspicious of an abscess and multiple vegetation at the aortic valves.</p> <p>The patient received probabilistic anti biotherapy and congestive heart failure treatment. Surgery was indicated.</p> <p>Under probabilistic anti biotherapy, evolution was favorable at first then the clinical condition has deteriorated resulting in the death of the patient. The check up echo cardiographic noted a significant increase in the volume of the abscess.</p> <p>Conclusion: The aortic ring abscess is a serious complication of infectious endocarditis on native and prosthetic valve. Diagnosis is based mainly on Transthoracic and transosoephagial echocardiography. Surgery is indicated.
Introduction
The aortic ring abscess is a rare and serious complication of infective endocarditis, usually occurring on previously damaged valves. Rheumatic fever is the most common cause of valvular lesions and is a public health problem in developing countries and is more common in women. Echocardiography remains the key examination for diagnosis, management is expensive and the prognosis is generally poor, especially in developing countries. We report the case of a 29-year-old multiple valves disease patient with fatal aortic ring abscess.
Observation
Patient MD, 29 years old woman, nulliparous, with a history of recurrent tonsillitis and polyarthralgia in childhood, known to have a multiple valves disease type of mitral, aortic and tricuspid regurgitations and stenosis. Since 1998 patient was hospitalized several times in the department for suspicion of infectious endocarditis. The first hospitalization was in 1999 for rheumatic evolution, the second in 2007 for fever and negative blood culture on valvular heart disease. On admission, she had a poor condition, an important weight loss, a clinical anemia. There was also eodema of the lower limbs going back to the soft knees, painless and taking the scoop. Blood pressure was 100/50 mmHg, temperature was 36.2°C, heart rate was 88 bpm, respiratory rate was 24 cycles / min, diuresis was 1200 cc, weight was 49 Kg for 1.68 m and a BMI at 17.37 Kg/m².
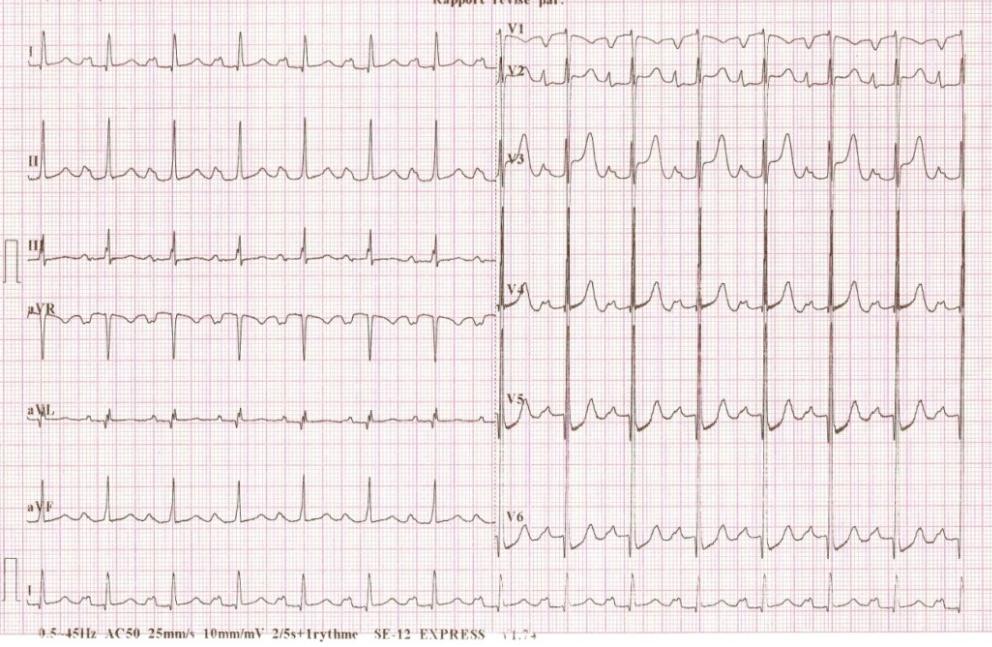
The physical examination noted a parasternal right ventricular impulse and a hyperdynamic left ventricular impulse. Heart sounds were regular with apexic diastolic rolling, 3/4 systolic murmur at apex site, 4/6 rough left lateral systolic murmur, loud pulmonary B2. Peripheral pulses were present and symmetrical; the lungs were normal; painfullhepatomegalia(13 cm); the ENT and stomatological examination were normal. The biology found a nonspecific inflammatory syndrome with neutrophil leukocytosis at 10,080 elements / mm3 (88%) and a positive CRP at 48mg / l; sedimentation rate and fibrinemia were normal at 03 mm in the first hour and 0.60 g/l, respectively. In addition, thrombocytopenia was noted at 28,000 elements / mm3, normochromic normocytic anemia with a hemoglobin level of 11 g/dl, antistreptolysin O (ASLO) at 400 IU/l. blood sugar and renal function were normal. Blood cultures, HIV serology, Hbs antigen, Emmel test, AFB search were negative. Hepatic assessment was disrupted with slightly elevated transaminases (ASAT at 90.1 IU/I, ALAT at 49.3 IU/I); the prothrombin rate at 34% for a spontaneous INR at 2.34. The blood ionogram showed hyponatremia at 118 mEq/l, serum potassium at 5.1 mEq/l and chlorine at 91 mEq/l. according to modified Duke criteria, AE was possible in our patient. The electrocardiogram (Figure 1) recorded a regular sinus rhythm with a heart rate of 85 cycles per minute (cpm), a QRS axis at + 50°, atrial hypertrophy and left ventricular hypertrophy.
The chest X-ray showed cardiomegaly with a diaphragmatic upper extremity, a cardio-thoracic ratio of 0.58, rectitude of the left middle arch, and a double contoured aspect of the right lower arch. Transthoracic Doppler echocardiography showed rheumatic multiple valves disease with tight mitral stenosis, moderate tricuspid regurgitation, and mild aortic regurgitation. In addition, the echocardiography noted a dilation of the Valsalva sinus at 47 mm with a fluid collection towards the posterior valsalva sinus, very suspicious of an abscess (Figure 2), but also the presence of multiple attached vegetations to the aortic sigmoid. Transoesophageal echocardiography confirms this suspicious image of abscess of the posterior aortic ring.
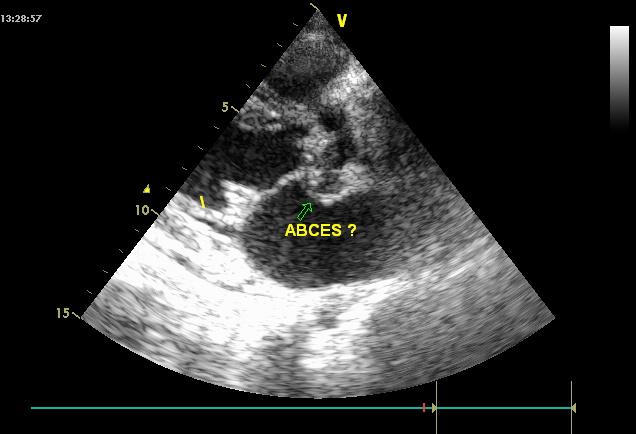
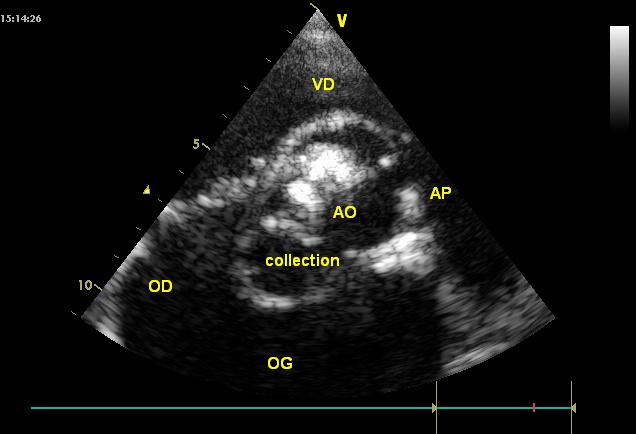
Figure 2: Transthoracic echocardiography image showing post-admission aortic abscess. The patient was put on probabilistic bi-antibiotic therapy (Gentamicin and Ceftriaxone) and under symptomatic treatment of heart failure (diuretics and ACE). Surgery indication was discussed The evolution under treatment was favorable with stable apyrexia, a regression of heart failure symptoms. However, systematic echocardiography and biology screening systematic before discharge, showed persistence of anemia, biological inflammatory syndrome, thrombocytopenia and image of abscess. Patient was discharged after 45 days of hospitalization and she was oriented in surgery. Four weeks later, the patient who did not receive surgical treatment was readmitted to the department for serious worsening of her condition. It is a state of septic shock associated with signs of global heart failure. The echocardiographic control noted a worsening of the abscess which doubled or tripled its volume (Figure 3).
The death occurred after 72 hours in a state of multi- organ failure.
Discussion
Aortic ring abscesses are found in 13-30% of infectious endocarditis and remain associated with heavy mortality [1, 2, 3]. These abscesses testify to an infectious process that most often reaches the aortic sleeve and can reach several parts of the heart. Extension to the aortic ring may result in abscess of the interventricular or interauricular septum, right ventricle or membranous septum, root of the large mitral valve or pulmonary artery, depending on the aortic sigmoid initially involved. The spread of suppuration to the central fibrous nucleus and the upper part of the interventricular septum exposes the lesions to Hissian tissue with the risk of severe conduction disturbances [4]. The diagnosis of IE remains based on the Duke criteria, developed in 1994 and adapted in 2002. It is therefore based on clinical examination, echocardiography and microbiological results [5, 6]. In 3 to 30% of cases of IE, blood cultures are negative. In our patient the blood cultures were negative. Transthoracic and especially transesophageal echocardiography is the main tool for the detection of abscesses of the aortic annulus. Ring abscess is common in infective endocarditis. A 1985 study published in the Archives of Heart and Vascular Diseases found 25 cardiac abscesses in 125 autopsies of fatal infective endocarditis (16 aortic, 5 mitral and 4 associated) [6]. Another study in the United States found 59 cases of aortic abscess in a sample of 95 necropsies performed in 128 infective endocarditis [1]. The abscesses are also common around 50% during prosthetic endocarditis as described in the literature [7].
In the case of our patient reported in this study, the abscess occurred on remodeled native valves of rheumatic origin. Treatment uses antibiotics but remains surgical [4, 5, 8]. The main bacteria found in blood culture in our cardiology unit are Gram positive [9]. We used mostly gram negative antibiotics. Two reasons to explain that choice, the efficiency in the IE we manage in our unit and the low cost making it more affordable to our patients. Our patient did not benefit from surgical management. The evolution was towards the enlargement of the abscess despite antibiotic therapy before ending in a septic shock table with multiple organ failure.
Conclusion
The aortic ring abscess is a major complication of infectious endocarditis whether native valve or on prosthesis. The diagnosis is mainly based on transthoracic and especially transesophageal echocardiography. Medical treatments based on antibiotic therapy are ineffective hence the collaboration with surgeons for better care.
References
-
Arnett EN, Roberts WC (1976) Valve Ring Abscess in Active Endocarditic Infection: Frequency, Location, Chest Clinical Diagnosis of the Study of 95 Necropsy Patients. Circulation 54(1): 140-145.
-
Benzarouel D, Ouanan F, Boumzebra D, El Hattaoui M (2012) Peraortal abscess and infectious endocarditis: beware of this dangerous duo. Ann Cardiold'Angeiol 61(4): 274-280
-
Shafran SD (2002) Infective endocarditis and perivalvular abscess: a dangerous duo. CMAJ 167(1): 38-39.
-
Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, et al. (2015) ESC Guidelines for the management of infective endocarditis. Eur Heart J 36(44): 3075-3128.
-
Rossel A, Carballo D, Carballo S (2012) Diagnosis and early management of infectious endocarditis. Rev Med Switzerland 8: 1966-1971.
-
Loire R, Madonna O, Tabib A (1985) Cardiac abscess in infectious endocarditis. About 25 anatomo-clinical cases. Arch Mal Coeur 78: 821-827.
-
Coignard E, Makri R, Isnard R (1999) Abscess of the aortic ring in an aortic mechanical valve carrier. The Letter of the Cardiologist 316: 23-24.
-
Choussat R, Thomas D, Isnard R, Michel PL, Iung B, et al. (1999) Perivalvular abscesses associated with endocarditis. Eur Heart J 20(3): 232-241.
-
Ndiaye MB, Diao M, Kane Ad, Bodian M, Mbaye A, et al. (2010) Endocardite infectieuse en milieu cardiologique Dakarois: étude descriptive à propos de 39 cas. The Pan AfricanMedical Journal 7: 12-22.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study