Coronary Traffic Jam Caused by a Trifurcating Left Main in a Cardiac Arrest STEMI Patient
Case Report: A 64 year old male presented to the emergency room as a case of cardiogenic shock. He had history of previous percutaneous coronary intervention (PCI) to left anterior descending artery (LAD) two years ago.ECG taken at emergency room (ER) showed acute inferolateral ST elevation myocardial infarction (STEMI). Coronary angiogram (CAG) revealed trifurcating left main with ramus as the culprit lesion. PCI of trifurcating left main (LM) is a complex procedure. But the challenge was overlapping previous LAD stent in the setting of trifurcating left main with acute angles between LAD, Ramus and LCx with medina classification (1 1 0 1)
El Gizy S, Al Jarallah M, Rajan R* and Dashti R
Cardiac Center, Amiri Hospital, Kuwait, E-mail: cardiology08@gmail.com LAD, Ramus and LCx with medina classification (1 1 0 1) Abbrevations: PCI: Percutaneous Coronary Intervention; STEMI: ST Elevation Myocardial Infarction; ER: Emergency Room; CAG: Coronary Angiogram; LM: Left Main; CABG: Coronary Artery Bypass Grafting; DAPT: Dual Antiplatelet Therapy; LCX: Left Circumflex Coronary Artery; TIMI: Thrombolysis in Myocardial Infarction; RI: Ramus Intermedius.
Introduction
First ever LM angioplasty was performed by Dr Gruntzig in 1979 [1]. Trifurcation stenting of left main (LM) coronary artery is considered to be a very high risk procedure [2]. Treatment of complex trifurcation lesions has always been a challenge to the interventional cardiologists despite the evolution of technology in the field of PCI. Treating such lesions with DES along with kissing and simultaneous use of multiple balloon technique appears promising. Lesions of LM trifurcation is usually managed by Coronary artery bypass grafting (CABG) but patient who is having high risk for surgery may be taken for LM trifurcation stenting [3]. Syntax Score must be considered while managing such complex coronary lesions. LE MANS is the first trial which showed LM stenting has similar outcomes as in CABG [4].
A 64 years old male patient known diabetic, hypertensive and smoker presented to the emergency room as a case of cardiogenic shock. He had history of coronary artery disease with previous PCI and stenting to LAD.ECG taken at ER showed sinus rhythm with ST elevation in II III AvF. Patient was loaded with dual antiplatelet therapy (DAPT) and low molecular weight heparin and an urgent coronary angiography via right radial artery approach was planned. Coronary angiogram showed (Medina 1101) trifurcation of LM with totally occluded ramus branch, LAD showed patent previous stent which was encroaching to the ostium of the ramus branch which causes the total occlusion of the ramus artery and left circumflex coronary artery (LCX). Ramus was found to have thrombus (Figure 1).
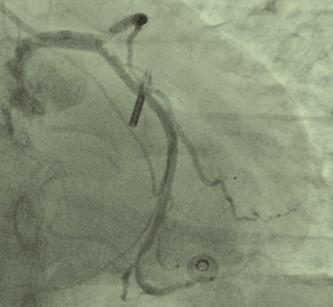
Figure 1: Trifurcation of LM with totally occluded ramus branch. We decided to do PCI to the culprit lesion which was the ramus branch. A 6 Fr EBU guiding catheter was engaged into the left main via the right radial artery and 0.014-inch coronary wire was placed into the ramus artery. Aspiration catheter was used but it didn’t cross the ostium of the ramus branch because of the encroachment of the stent of the LAD. The ostium of ramus showed severe ostial stenosis. As a results of trials of aspiration, the ramus branch appeared as a big and sizable artery. Predilatation was done with balloons 1.5x15 and 2.5x15 the LAD and LCX was compromised, so we inserted 2 wires into the LAD and LCX through femoral artery with another guiding catheter into the left main (Figure 2). We did inflation of LAD, LCX and ramus branch at the same time (Figure 3).
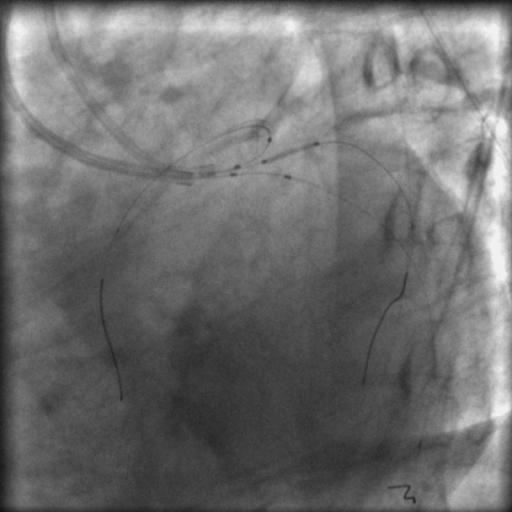
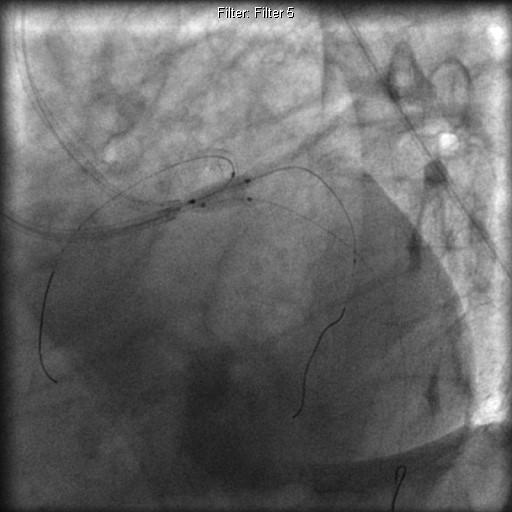
Figure 3: Simultaneous inflation of 3 kissing balloons. As a result of PCI to ramus branch, the ostium of LAD and LCX were comprised, so we did kissing balloons for both LAD and Ramus. The result was good but the ostium of LCX was affected. Then we did kissing balloons between ramus and LCX. The result was good for LCX and ramus but the LAD was compromised again, so we did the kissing balloons at the same time for LAD, ramus and LCx. The final angiographic picture showed a successful revascularization with (TIMI) flow (Figure 4). The patient was asymptomatic and discharged the next day and was advised to continue DAPT with statin.

Discussion
Trifurcation lesions are less frequent and are challenging than bifurcation lesions [5]. Incidence of ramus intermedius ranges from 15 to 30% [6, 7]. Most of the LM trifurcation arises in the presence of ramus intermedius (RI) coronary artery [8]. In our case RI was present and been one of the contributor to the trifurcation. LM trifurcation can be treated either by CABG or high risk PCI. While treating LM trifurcation lesions with PCI, there are many major limitations one may encounter. Mainly the difficulty in passing multiple guide wires and balloons. It may increase the time consumed for the total procedure and thereby the use of more contrast along with longer exposure to fluoroscopy. Also it is associated with high probability of having adverse events like stent thrombosis [2]. In our case, the lesions were close to each other’s with acute angles in between LAD, ramus and LCX. We stented ramus artery after predilatation, then used kissing balloons between LAD and ramus but LCX was affected so we did kissing balloons between ramus and LCX. As a result of this LAD was affected so the decision for 2nd guiding and triple balloons inflation at the same time was taken.
Conclusion
In the setting of complex trifurcation lesions, bifurcation and trifurcation maneuver with kissing and simultaneous inflation of balloons appears to be a better option for successful revascularisation. Multiple guiding catheters are recommended for getting free mobility of the wires, balloons and stents.
References
-
Gruntzig AR, Senning A, Siegenthaler WE (1979) Nonoperative dilatation of coronary-artery stenosis: percutaneous transluminal coronary angioplasty, N Engl J Med 301(2): 61-68.
-
Shammas NW, Dippel EJ, Avila A, Gehbauer L, Farland L, et al. (2007) Long-term outcomes in treating left main trifurcation coronary artery disease with the Paclitaxel-eluting stent. J Invasive Cardiol 19(2): 77- 82.
-
Shammas NW, Shammas GA, Jerin M, Parikh A, Coin K, et al. (2009) Treatment of Left Main Coronary Trifurcation Lesions with the Paclitaxel Drug-Eluting Stent: Mid-Term Outcomes from a Tertiary Medical Center,J Invasive Cardiol 21(7): 321-325.
-
Tsai TH, Cheng CI (2016) Stenting or bypass surgery for unprotected left main coronary artery disease-still a long rally to go. Journal of Thoracic Disease 8(9): 2292-2295.
-
Shao C, Stella PR, Agostoni P (2012) Complex Made Easy: Left Anterior Descending Artery Trifurcation Lesion Completely Treated With a Single Device. J Invasive Cardiol 24(8): 164-166.
-
Koşar P, Ergun E, Oztürk C, Koşar U (2009) Anatomic variations and anomalies of the coronary arteries: 64- slice CT angiographic appearance. Diagn Interv Radiol 15(4): 275-283.
-
O'Brien JP, Srichai MB, Hecht EM, Kim DC, Jacobs JE et al. (2007) Anatomy of the heart at multidetector CT: what the radiologist needs to know. Radiographics 27(6): 1569-1582.
-
Kini S, Bis KG, Weaver L (2007) Normal and variant coronary arterial and venous anatomy on high- resolution CT angiography. AJR Am J Roentgenol 188(6): 1665-1674.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study