Comparison of Real-Time Ultrasonography Guided Versus Conventional Anatomical Landmark Guided Central Venous Cannulation
Background: Ultrasonography provides ‘real-time’ imaging thus reducing chance of complications while placing a central venous catheter. Placement of catheter becomes faster than conventional method. We performed a study in adults to compare USG guided central venous cannulation with conventional anatomical landmark technique in terms of ease of cannulation, number of attempts, success or failure rate, time consumed for successful cannulation and associated complications. Methods: Patients were randomized into two groups. In Group A, central venous cannulation was done by conventional anatomical landmark guided technique. In Group B, USG guided central venous cannulation was done. Data regarding patient demography, number of attempts, site and side of cannulation, time taken for each successful cannulation and any complication in terms of arterial puncture, hematoma, hemothorax, pneumothorax and misplacement were recorded. Thereafter intergroup comparison was done. Results: Both groups were comparable in terms of number of attempts, success or failure rate and complications of the procedure. Mean time taken for successful cannulation in Group A was 438 seconds and in Group B it was 224 seconds (p 0.004) which is statistically significant. Conclusion: We conclude that USG guided central venous cannulation is faster than conventional anatomical landmark guided technique.
Introduction
Placement of central venous catheter is very important in many surgeries like in cases of cardiac surgeries where measuring central venous pressure is very much important. It is used for hemodynamic monitoring, administration of inotropes and vasodilators. It is an integral part of critical care management. Central venous line is used for administration of parenteral nutrition, cytotoxic drugs, continuous or intermittent monitoring of biochemical or physiological parameters. When peripheral venous access is not possible CVC is done.
Traditionally cannulation has been done blindly using anatomical landmark guided technique which is associated with many well-known complications such as arterial puncture, hematoma formation, pneumothorax, hemothorax, air embolism, nerve injury and misplacement. Even with experienced operators conventional method of placing central venous cannula may have complication rate as high as 12.3%. The internal jugular vein, subclavian vein and femoral veins are commonly used sites for central venous cannulation [1].
Placing central venous catheter in paediatric patients is very difficult where the vessels are much smaller in size and easily compressible.
Ultrasonography provides ‘real-time’ imaging, i.e. the needle can be visualised entering the vein. Role of USG while doing central venous line is well established very long ago. The agency for healthcare research and quality in USA and the National Institute for Clinical Excellence (NICE) in UK recommends CVC placement under USG guidance to improve patient care. USG guidance also decreases number of attempts per cannulation increasing success rate makes the procedure faster and lessens complications as USG provides ‘real-time’ imaging. Success rate with USG guidance can be as high as 100% with less complication. Availability of USG guidance make many procedures as bedside procedures. But its acceptance and popularity is hampered due to its unavailability and lack of trained personnel [2, 3, 4, 5, 6, 7].
This prospective randomized controlled study was performed to compare USG guided central venous cannulation with conventional anatomical landmark guided technique in terms of number of attempts, success or failure rate, complication rate and time taken for successful cannulation.
Material and Methods
Approval from Institutional ethics committee and informed consent from each patient were obtained. It was a prospective, single blinded, randomised controlled study. Adult patients, aged between 20 to 60 years of both sexes scheduled for elective cardiac surgery in cardiovascular and thoracic surgery OT were included as they need central venous access for measurement of central venous pressure and administration of inotropes and vasodilators.
Exclusion criteria were patient refusal, patients aged below 20 years, and above 60 years, patients with neck abnormality like anatomical, congenital, post-burn contracture etc. local site infection, coagulopathy, known vascular abnormality and diminished pulmonary function assumed to be unable to tolerate potential complication of pneumothorax were excluded from study.
Sample size
Sample size for the study was calculated on the basis of success rate of cannulation at first attempt as a primary outcome measure. It was estimated that 38 subjects would be required for each group in order to detect 20% improvement in successful cannulation when done under USG guidance compared to conventional anatomical landmark technique alone with 80% power and 5% probability of type-I error. This calculation assumes that success rate in the control group would be 75% on the basis of earlier studies and the calculation is one sided. nMaster 2.0 software (Department of biostatistics, Christian medical college, Vellore, 2012) was used for calculating sample size for this study. Assuming equal distribution of patients in both groups a total number of 76 patients was taken for the study (N=76) with 38 patients in each group (n=38). Patients were randomized into two groups using computer generated randomization chart.
Materials and Methods
Seventy six patients posted for elective cardiac surgery in CTVS OT were enrolled in this study and randomized on chart into two groups, group A and group B. Group A had 38 cases of conventional anatomical landmark guided central venous cannulation and Group B had 38 cases of USG guided central venous cannulation . The group were allocated by computer generated randomization chart.
Before the surgery, laboratory investigations were checked (Hb%, TLC, DLC, platelet count, ESR, FBS, PPBS, serum urea, creatinine, LFT, BT, CT, PT, APTT, INR, Echocardiography, CXR, ECG-12 lead, cath. Study and any other relevant investigations according to the patient). Proper anaesthetic check-up and optimisation was done before the day of operation.
On the morning of surgery, patient were wheeled inside the operating theatre and standard monitors were attached (ECG, pulse oximetry, NIBP). Peripheral intravenous line was established, arterial line (radial or femoral) was done under local analgesia. Thereafter induction was done with inj. midazolam, inj. fentanyl and inj. thiopentone sodium and patient was intubated after giving inj. rocuronium. After intubation central venous cannulation was done. Maintenance of anesthesia was done with oxygen, nitous oxide, isoflurane and inj. vecuronium.
Patient was positioned in Trendelenburg position, a wedge was placed below the shoulder. Head was turned to contra-lateral side. The right sided internal jugular vein was the first preferred site for central venous cannulation. Right subclavian vein, left subclavian vein, left internal jugular vein and femoral vein were tried only when we failed to place central venous cannula in right IJV successfully. Group A: After taking all sterile precautions the right sided carotid artery pulsation was felt at the apex area in the neck formed by two heads of sternocleidomastoid muscle.
Artery was pressed medially and by the lateral side of this arterial pulsation a 22G seeker needle was introduced directing towards ipsilateral nipple at an angle of 20-30 degree with the skin to locate the right internal jugular vein. Thereafter the 18G introducer needle was inserted lateral to pulsation point by the side of the seeker needle in the same direction. After successful aspiration of blood guide-wire was inserted and the introducer needle was withdrawn. Dilator was passed through the guide-wire to dilate the tract and withdrawn. Central venous catheter was inserted and guide-wire was withdrawn. Free flow of blood through CVC was checked. CVC was sutured with the skin and dressing was done.
Group B: In this group a portable ultrasound machine with 10 M Hz linear array vascular probe was used to detect the vein. Lead and probe was cleaned with antiseptic solutions, sterile jelly was applied over the probe and covered with a sterile sheath. Sterile jelly was also applied over the area to be scanned. The probe was placed perpendicular to the skin over the apex of the triangle. Each probe has orientation marker over it which correlates to a mark over the screen. In longitudinal plane, the probe is oriented with the marker towards patients head and visualise the IJV along its long axis. In transverse plane, probe is oriented with the marker towards the patients’ right so providing image similar to CT scan. Vessels were visualised in transverse section with 2D USG. IJV was visualised as non-pulsatile compressible oval structure while the internal carotid artery as a pulsatile oval structure. If pressure was applied IJV got compressed whereas artery remained as such. Every time patency of the vessel was checked with compressibility tests. Once vein was identified probe was positioned to keep the vein at the centre of the screen. Whenever the introducer needle was pushed the veins got compressed. As the needle was inserted through the anterior wall, it slowly pushed inside the vein puncturing the wall without opposing the posterior wall to avoid double puncture. After successful aspiration of blood the rest of the procedure was same as before.
To assess complication chest x-ray was obtained after the procedure. Complications like arterial puncture, hematoma, and pneumothorax were recorded. The procedure was considered to be failure if there was more than one attempt, site change after failure to pass catheter in right IJV or handover to more experienced operator after failure of two attempts at right IJV. An attempt was defined as introducer needle insertion through the skin and removal from the skin. At the end of the procedure data was collected regarding patient demographics, method of insertion, site and side of CVC, number of attempts. Any operator change and time for introducer needle from insertion to successful blood aspiration and total time for successful cannulation were recorded.
Statistical Analysis of Data
Data was summarised by descriptive statistics namely mean and standard deviation (SD) for numerical variables and counts and percentages (%) for categorical variables. Chi-sqare test, Fisher’s exact test was employed for intergroup comparison of the categorical variables. All statistical analyses were two tailed and p<0.05 was considered as statistically significant.
Results
No statistical significant difference was seen between both groups in distribution of age (years) and sex (male/female) (Table 1).
| Group A | Group B | p value | ||
| Age | 44.9±14.4 | 42.2±13.01 | 0.38 | |
| (mean±SD) | 44.9±14.4 | 42.2±13.01 | 0.38 | |
| Sex | Male | 23 | 30 | 0.08 |
| Sex | Female | 15 | 8 | 0.08 |
Table 1: Distribution of age and sex.
In respect to number of attempts, success and failure rate, and complication rate both groups are found to be comparable. Only the total time taken for successful cannulation found to be significantly lesser in USG guided technique than the conventional anatomical landmark guided technique.
Average number of attempts with 18G introducer needle is 1.3 in both the groups (p 0.88) (Figure 1).
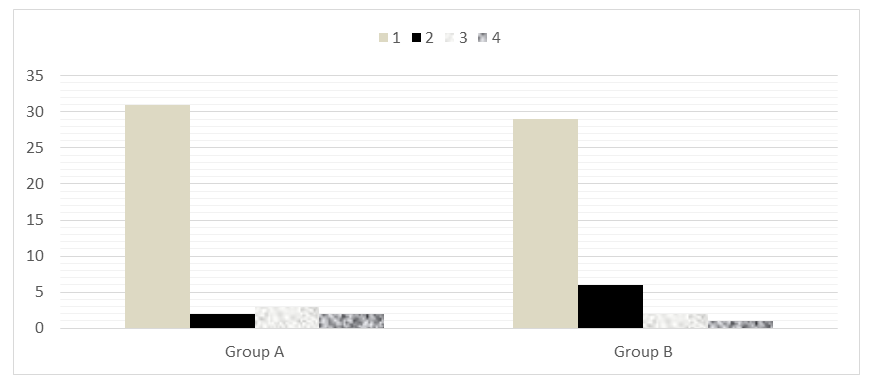
Figure1: Number of attempts by 18G introducer needle.
we had to change the site due to failure to pass the catheter in right IJV (Table 2).
| Right internal jugular vein | Right subclavian vein | Left subclavian vein | p value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group A | 35 | 2 | 1 | 0.2 | ||||||||
| Group B | 38 | 0 | 0 |
Table2: Number of cannulation at different sites.
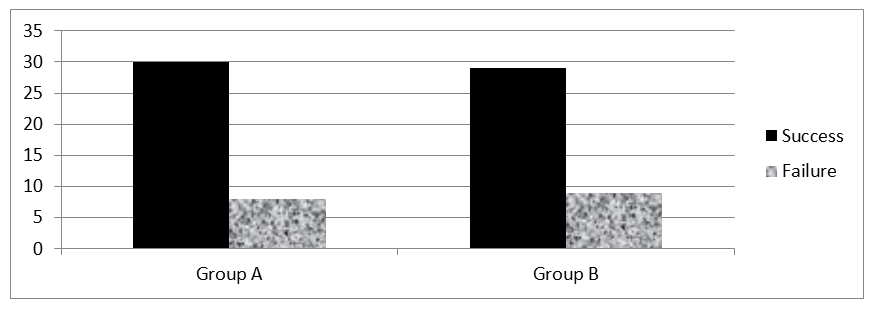
30 cannulations were successful out of 38 cases and in group B 29 cannulations were successful (Figure 2).
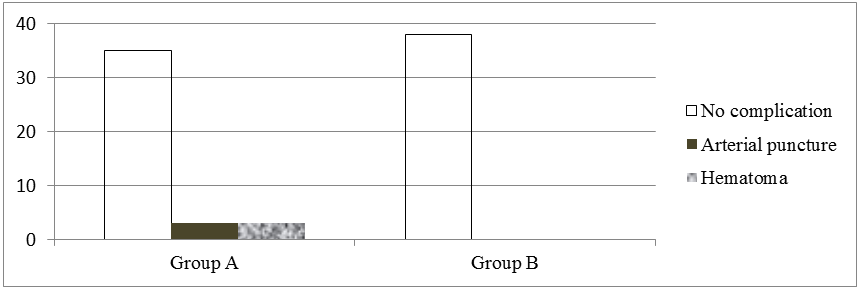
Regarding complications no case of hemothorax, pneumothorax or misplacement were noted in patients of either group. Only 3 cases of artery puncture and hematoma formation were noted in Group A patients but when intergroup comparison was done it was also found to have no statistical significance (p 0.07) (Figure 3).
Mean time taken for locating the IJV by 18G introducer needle is 118 seconds by conventional method and it is 39 seconds in USG guided technique which has no statistical significance (p 0.06). The mean time taken for successful placement of cannula is 438 seconds in Group A and in Group B it is 224 seconds which is significantly (p 0.004) lesser than the other group.
Discussion
In this study average attempt by 18G introducer needle was 1.3 in both the groups (p 0.88). Cannulation was successful in 78.9% by conventional method whereas it was 76.3% by USG guidance (p 0.08). 81.5% cannulation was successful by conventional anatomical landmark guided technique in first attempt while it was 76.3% in USG guided technique. 13.1% successful cannulation needed more than two attempts in conventional method whereas it is 7.89% when USG guided. In 7.8% of patients we had to change the site due to failure to pass the cannula in right IJV in conventional method but none in USG guided technique (p 0.2). 7.89% of patients in conventional method had complication. In 3 patients arterial puncture and hematoma were noted. In USG guided technique no complication were reported. But complication rate is also comparable in both the groups with no statistical significance (P 0.07). Mean time taken for insertion into the vein and successful aspiration of blood by 18G introducer needle was 118 seconds in conventional method and it is 39 seconds in USG guidance (p 0.06). USG guided cannulation was found to be much faster (average time 224 seconds) than conventionally done cannulation (average time 438 seconds) with statistical significance (p 0.004). Our limitations of the study were less number of study population and less operator experience with the ultrasonographic method.
GB Palepu et al performed a study in 2009 and they found IJV cannulation was successful in 91.2% by landmark method and in 97.6% when it was USG guided (p 0.006) [8]. Cannulation was successful on first attempt in 72.7% by landmark technique, while it was 84.4% with USG guidance (p 0.004). Overall complication rate was 9.8% by landmark technique and 4.4% when USG guided (p 0.03). For subclavian vein, the success rate was 100% when USG guided while it was 92.9% for the other (p 0.52). Cannulation on first attempt was successful in 82.4% patients when USG guided while it was 71.4% for the other technique (p 0.49). Complication rate was 14.3% by landmark technique and 11.8% when USG guided (p 0.99).
Agarwal A et al had done a study where they found the mean time for successful insertion was 145 sec. when guided by USG and 176.5 sec. in landmark technique (p=0.00) [9]. An average of 1.2 attempts per cannulation was required when USG guided while 1.53 for the other group (p=0.03). 10% had arterial puncture and 2.5% pneumothorax in landmark technique and none when USG guided.
Grebenik CR, et al. found in 2004 that success rates were significantly greater in landmark group compared to ultrasound group (89.3% vs. 78%, p<0.002), and arterial puncture rates were significantly lower in landmark group (6.2% vs. 11.9%, p<0.03) [10]. There was no significant difference between the two groups in the time taken to perform the cannulation.
Breschan C, et al. found central venous cannulation was successful in all cases [11]. In 73.8% cases cannulation was successful in first attempt, in 14.2% cases after second attempt, and in 11.9% after three attempts. Significantly more puncture attempts were needed in smaller weight and younger children, whereas the time course of the study had no significant impact on the success rate.
Conclusion
Ultrasonography guided central venous cannulation is faster than conventional anatomical landmark guided central venous cannulation.
References
-
Schummer W, Schummer C, Rose N, Niesen WD, Sakka SG (2007) Mechanical complications and malpositions of central venous cannulations by experienced operators. A prospective study of 1794 catheterisations in critically ill patients. Intensive Care Med 33(6): 1055-1059.
-
Rothschild JM (2001) Ultrasound guidance of central vein catheterisation. Making health care safer: A critical analysis of patient safety practices. AHRQ publication no. 01-EO58: 245-253.
-
Guidance on the use of ultrasound locating devices for placing central venous catheters (2002) NICE technology appraisal no. 49.
-
Karakitos D, Labropoulos N, De Groot E, Patrianakos AP, Kouraklis G, et al. (2006) Real-time ultrasound guided catheterisation of the internal jugular vein: A prospective comparison with the landmark technique in critical care patients. Critical care 10(6): R162.
-
Denys BG, Uretsky BF, Reddy S (1993) Ultrasound assisted cannulation of the internal jugular vein: A prospective comparison to the external landmark guided technique. Circulation 87(5): 1557-1567.
-
Randolph AG, Cook DJ, Gonzales CA, Pribble CG (1996) Ultrasound guidance for placement of central venous catheters: A meta-analysis of the literature. Crit Care Med 24(12): 2053-2058.
-
Fry WR, Clargett GC, O’Rourke PT (1999) Ultrasound guided central venous access. Arch Surg 134(7): 738- 741.
-
Palepu GB, Deven J, Subrahmanyam M, Mohan S (2009) Impact of ultrasonography on central venous catheter insertion in intensive care. Indian J Radiol Imaging 19(3): 191-198.
-
Agrawal A, Singh DK, Singh AP (2009) Ultrasonography: A novel approach to central venous cannulation. Indian J Crit Care Med 13(4): 213-216.
-
CR Grebenik, A Boyce, ME Sinclair, RD Evans, DG Mason, et al. (2004) NICE guidelines for central venous catheterization in children. Is the evidence base sufficient? Br J Anaesth 92(6): 827-830.
-
Breschan C, Platzer M, Jost R, Stettner H, Beyer AS, at al. (2011) Consecutive, prospective case series of a new method for ultrasound-guided supraclavicular approach to the brachiocephalic vein in children. British Journal of Anaesthesia 106(5): 732-737.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study