Iatrogenic Injuries during Retrograde Delivery of Cardioplegia- Prevention, Diagnosis and Management: A Collective Review
The causative factors and morphologic spectrum of iatrogenic coronary sinus injuries during retrograde delivery of cardioplegia through the coronary sinus are many and varied. In this review, we give an account of all cases previously described as iatrogenic injuries of the coronary sinus, analyzing in detail those cases where an accurate anatomical description of the injuries was provided. We identified 27 investigations and reviewed the anatomic variations of the coronary sinus, causative mechanisms of injury to the coronary sinus, diagnostic features, intraoperative findings and management of the patients described. Transesophageal echocardiography, contrast injection into the coronary sinus and intraoperative identification of the catheter tip perforation of the inner wall of the coronary sinus, transmural migration and eventual perforation or laceration of the right ventricle and hemodynamic or pressure tracing of the coronary sinus identified these injuries involving the coronary sinus and its tributaries. We have grouped the injuries into categories that have a bearing on the appropriate surgical approach, discussing the appropriate repair for each group. We submit that an increased appreciation of various types of iatrogenic coronary sinus injuries may well contribute to its prevention and improved future surgical management.
Introduction
The goal of cardiac surgeons must be an unhurried correction of cardiac abnormalities under direct vision. “…The heart suffering no damage during periods of arrest.” So wrote Melrose and colleagues in The Lancet in 1955 in a classic treatise that initiated the concept of cardioplegia [1]. Although there have been major advances in the methods of myocardial protection since then, cardiac operations have nevertheless remained far from unhurried because of the anaerobic damage that can occur with all current methods of myocardial protection [2, 3, 4, 5, 6, 7].
The objective of myocardial protection is to prolong the safe operating time, prevent operative death, perioperative infarction and functional impairment. This objective ultimately translates into optimizing the ratio of myocardial energy supply to energy demand, while the aorta is cross-clamped [2, 3, 4, 5]. Despite numerous advances in methods of myocardial protection time remains a major adversary of the cardiac surgeon. Aortic occlusion renders the myocardium ischemic and dependent solely on the anaerobic metabolism. Hence, prolonged procedures are associated with higher morbidity and mortality [5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17]. Methods of myocardial protection in general use today provide excellent preservation for elective procedures in low-risk patients. They are associated with minimal attendant morbidity and mortality. The outcomes, however, are less optimal for urgent operations in high-risk subgroups with poor ventricular function and provide the impetus for investigating alternative methods of myocardial protection [12, 13, 14, 15, 16, 17, 18, 19, 20].
Regardless of its potential and proven advantages over the antegrade method, retrograde myocardial protection regime failed to gain wider acceptance for more than 20 years until the pioneering work of Menasche and colleagues in 1982 and Gundry and colleagues in 1990 [21, 22]. Their work and the introduction of efficient closed delivery systems, incorporating DLP INC and Research Medical INC designed perfusion catheters have resulted in the resurgence of retrograde cardioplegia in high-risk and re-operative patients [23, 24, 25, 26, 27]. However, there is a sharp contrast between the number of experimental and clinical data available [23, 28, 29, 30, 31, 32, 33, 34]. In the current practice, coronary sinus has been used as a route of delivery in several myocardial protection technique strategies including intermittent cold crystalloid cardioplegia, intermittent cold blood cardioplegia, continuous normothermic blood cardioplegia and continuous cold blood cardioplegia [24, 25, 35, 36, 37, 38, 39, 40, 41].
Despite widespread use of retrograde coronary sinus cardioplegia in recent years, little has been reported regarding the etiological mechanisms of coronary sinus injuries, their prevention, diagnosis and management [24, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60]. With these deficiencies in mind, we have analyzed the published literature, using a MEDLINE search to identify the described instances of coronary sinus injury, the variations in the coronary venous anatomy, the methodology of diagnosis and the treatment modalities utilized for a successful outcome. We have synthesized all of these features with regard to their bearing on the strategies for surgical management of coronary sinus injuries. As far as we could establish, there have been 27 publications addressing specifically the etiological mechanisms and management of various types of coronary sinus injuries. For the purposes of this review we have selected these 27 publications which have an accurate description of the management strategy and perioperative mortality [24, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60].
Advantages of Retrograde Cardioplegia
Retrograde coronary sinus cardioplegic perfusion offers several advantages.
- It avoids the risk of injury to the coronary ostium associated with ostial cannulation [26, 27].
- In the presence of critically obstructive coronary artery disease, retrograde coronary sinus perfusion provides homogenous cooling [26, 27, 61, 62].
- It is a useful procedure in the presence of calcified aorta [45].
- The surgery remains uninterrupted particularly during combined mitral and aortic valve replacement, Bentalls procedure, distal graft- aortic anastomosis and while closing the aortotomy [43, 44, 45].
- It reduces the occurrence of supraventricular arrhythmias by retarding atrial rewarming during aortic cross-clamp [21]. Possibly, the egress of cold cardioplegic solution causes topical endocardial cooling of the right atrium [24, 25, 26, 27].
- Retrograde cardioplegia can provide uniform myocardial protection in the grossly hypertrophied myocardium due to the presence of numerous venous channels in the human heart which act as effective conduits for delivery of cardioplegic ingredients in a uniform manner [24, 25, 26, 27, 42, 43, 44, 61, 62, 63, 64, 65].
- Adequate, immediate delivery of the cardioplegic solution is achieved, especially in the setting of type-A aortic dissection, thus minimising the ischemic time [66].
- Coronary sinus cardioplegia is able to retrogradely flush air and atheromatous debris from the coronary arteries [43, 44, 45].
It is the author’s routine practice to restart myocardial perfusion with warm blood via the pump after disconnecting the cardioplegia solution to decrease the myocardial ischemia in procedures requiring long aortic cross-clamp time, e.g., Bentalls procedure, concomitant valve replacement, coronary artery bypass grafting, and redo coronary artery bypass grafting [66, 67].
Limitations of Retrograde Coronary Sinus Cardioplegia
As outlined by Menasche in his report on 500 patients and other investigators including us, retrograde coronary sinus cardioplegia does have some limitations [45]. These include:
- Inadequate preservation of the right ventricle; this concern has been raised on the basis of canine studies [68]. However radionuclide angiocardiography studies, have demonstrated that the venous drainage patterns of the human right ventricle are more suitable for retrograde coronary perfusion, provided the balloon catheter does not impede cardioplegia flow into the distal branches of coronary sinus [26, 27, 69, 70, 71].
- The cardioplegia distribution is non-homogenous since the venous system is located predominantly subepicardially [72].
- Need for bicaval cannulation for proper positioning of the coronary sinus catheter.
- Injury to the coronary sinus which may vary from atrioventricular hematoma to coronary sinus rupture.
- It takes a longer time to arrest the heart with retrograde cardioplegia compared to the antegrade route.
However, this delay can be circumvented by the first induction dose of cardioplegia through antegrade route [73, 74, 75].
Incidence of Iatrogenic Coronary Sinus Injury
Due to the rarity of coronary sinus rupture, distinct repair techniques are infrequently reported, and its actual incidence is unknown. The main risk factor indeed remains, i.e., the retrograde cardioplegia. However, a misplaced venous cannula causing coronary sinus rupture has been reported in case of an unfavorable anatomic configuration and during minimally invasive cardiac surgical procedures. Left ventricular and septal hypertrophy represent other risk factors for coronary sinus injuries [46, 47, 48, 55, 58]. In the present day clinical practice, coronary sinus catheter misplacement or displacement has been reported in 2 to 2.6 percentages of patients and iatrogenic injuries in 0.06 to 0.6 percentages of patients. This is similar to the 1 to 5 percent incidence rate of coronary complications reported after the use of direct ostial cannulation [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60].
Coronary sinus injuries also have been reported during retrograde pacemaker lead implantation for biventricular simulation. Injuries in about 10 percentage of the cases are clinically silent and do not require surgical treatment. It is essential to establish a clinically feasible routine to correct these injuries [73, 74, 75, 76, 77, 78, 79, 80, 81, 82].
Retrograde Coronary Sinus Catheter: Techniques of Insertion, Determination of the Correct Placement
The retrograde cardioplegia catheter is inserted into the coronary sinus either by opening the right atrium or by puncturing the right atrial wall and blindly advancing the catheter. In the former, a successful insertion can be visually confirmed, but it requires isolation of superior and inferior caval veins. Meanwhile using the blind technique, it is difficult to insert and confirm successful placement by manual palpation especially in re- operations, smaller sized coronary sinus and in those with anomalies of the coronary venous drainage system. There is no way to recognize intracardiac events such as penetration of the coronary vein or coronary sinus perforation during cardiac manipulation.
The correct positioning of the catheter into the coronary sinus is vital to provide adequate administration of cardioplegia [81, 83, 84, 85, 86]. Methods to determine correct placement of the catheter are:
- Blind insertion into the right atrium close to inferior caval vein - right atrial junction. This technique risks injury to the atrium, inferior caval vein or coronary sinus and/or its tributaries.
- Palpate the right atrial-inferior caval vein junction on partial bypass to confirm the position of the catheter at the atrioventricular groove and the base of the left atrial appendage. This technique may be difficult in hemodynamically unstable patients [83, 84, 85, 86].
- Manasse has described an ingenious technique using a Y catheter inserted into the ascending aorta and another coronary sinus catheter inserted into the coronary sinus via right atrium and interconnecting the two. Thus, the arterial blood runs from the ascending aorta into the coronary sinus. If the retrograde sinus catheter is inserted correctly, the coronary sinus pressure increases immediately to 20-30 millimetre of mercury and does not change at all unless malpositioned [78, 86].
- Aldea and colleagues reported on the usefulness of transesophageal echocardiography for directing the coronary sinus catheter in the blind technique.79 The coronary sinus is imaged in long axis by slightly advancing or retroflexing the probe from the mid- esophageal four-chamber view. It is seen in the short axis in the mid-esophageal two-chamber view just superior to the atrioventricular groove. The modified bicaval view with the probe in the mid esophagus at 110-120 degrees shows the orifice of the coronary sinus and is useful in placing percutaneous coronary sinus catheters during minimally invasive procedures [55, 79, 80].
- Fluoroscopy and contrast injection: coronary sinus catheter placement via the right internal jugular vein is performed for retrograde cardioplegia administration in patients undergoing minimally invasive procedures.
Fluoroscopy allows visual confirmation of coronary sinus cannulation and detects extravasation [87, 88].
Causes for Unsuccessful Cannulation and Cardioplegia Delivery Failure
- Smaller sized coronary sinus opening. The diameter of the coronary sinus orifice ranges from 4.7 mm to 10.7 mm (average 7.9 mm) [72, 76].
- As the catheter is inserted into the right atrium and advanced along the posterolateral right atrial wall towards the coronary sinus orifice, it may push the right atrium wall adjacent to coronary sinus orifice and gets misdirected towards the inferior caval vein or right ventricle. As described by Orihasi K and colleagues, anterior traction of the lateral right atrial wall helps in straightening the course of the catheter along the posterior right atrial wall towards the coronary sinus orifice [76]. This maneuver may not be possible in re-operative cases due to adhesions [79]. Transesophageal echocardiography is advantageous in guiding the catheter into the coronary sinus in such cases [76].
- Another reason for unsuccessful cannulation was the common orifice of the coronary sinus and middle cardiac vein.
If the operator forcefully advances the catheter in the branch vein against the resistance, the cardiac vein can be lacerated or penetrated. Higami and colleagues monitored the pressure at the catheter tip during retrograde infusion and obtained an unusually high pressure in 7.5 percentages of cases [86]. When transesophageal echocardiography facility is not available, this anomaly of coronary sinus orifice can be identified by direct inspection or by preoperative coronary angiography [76].
The common reasons for retrograde cardioplegic delivery failure are smaller size coronary sinus opening, catheter displacement/misplacement, the direction of the catheter tip into one of the venous tributaries and extreme advancement of the catheter tip beyond the base of the left atrial appendage.
Diagnosis of Coronary Sinus Injuries
Diagnosis is difficult in most patients as can be seen in different publications. The diagnosis of coronary sinus injury is based on appropriate clinical context and echocardiography. The echocardiography will show an anechoic area with absence of flow suggestive of hematoma between the pulmonary veins and the inferior caval vein (the oblique sinus region) [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 87, 88, 89]. Catheter misplacement in the tributaries of the coronary sinus or the right ventricle is best identified by their radiologic appearance [56, 57]. Intraoperatively misplacement of a catheter in the posterior cardiac vein is diagnosed by manual palpation, damp pressure tracings, and transesophageal echocardiography [80, 87, 88, 89]. Catheter tip causing perforation of the inner wall of the coronary sinus is invariably associated with a transmural migration and eventual perforation or laceration of the right ventricle. This type of injury is usually extensive, but accessible and more easier to control than the posterior wall injuries [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60].
Pitfalls in the use of Transesophageal Echocardiography
Transesophageal echocardiography is undoubtedly an essential tool for determination of correct placement of coronary sinus catheter to avoid coronary sinus injury. However, there are several pitfalls in the use of transesophageal echocardiography.
- The images are tomographic, and the object out of the scanning plane is not visualized. With single plane transesophageal echocardiography, constant manipulation of the echocardiography probe is needed [76, 87, 88, 89].
- The catheter cannot be visualized when directed obliquely to the ultrasonic beam because the ultrasound beam is reflected elsewhere [76, 87, 88, 89].
- The right atrium and coronary sinus are not visualized distinctly when the blood is exsanguinated.
Pooling a certain amount of blood in the right atrium makes it easier to monitor the insertion procedures [76, 87, 88, 89].
Pattern of Coronary Sinus Injuries And Surgical Procedures for Injured Coronary Sinus and its Tributaries
Published literature document retrograde catheter displacement, misplacement, smaller size coronary sinus opening, common opening of the coronary sinus and middle cardiac vein, direction of the catheter tip in to one of the venous tributaries, extreme advancement of the catheter tip beyond the base of the left atrial appendage are the main causative factors of the failures to deliver retrograde cardioplegia. Malpositioning of the designed perfusion catheters often predisposes to a subsequent dislodgement or iatrogenic injuries [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60]. We used the descriptions of echocardiographic and surgical findings of the published cases with coronary sinus injury to stratify the various cases. We categorized the patients into several groups that have a bearing on the surgical mortality, morbidity, techniques and the outcome of surgical treatment (Figure 1). The patterns of iatrogenic injury during retrograde delivery of cardioplegia and their specific management as published in the literature are:
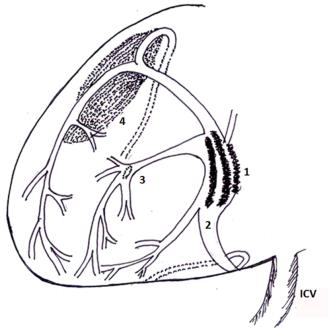
Figure 1: Diagrammatic representation demonstrating various types of iatrogenic injuries to the coronary sinus and its tributaries- (1) high pressure blow out rupture of the coronary sinus, (2) proximal injuries secondary to various causes, (3) distal rupture (perforation of the coronary sinus, and/or its radicals of the right ventricle), (4) hematoma without perforations in the atrioventricular groove. (ICV- Inferior caval vein) Proximal injuries: Proximal injuries are mainly due to direct perforation of the coronary sinus catheter tip with stylet in situ, catheter misplacement or displacement, electrodes used during biventricular facing and misdirected venous cannula while performing minimally invasive procedures. Malpositioning of the specially designed catheters, often predisposes to a subsequent dislodgement or iatrogenic injuries (Figure 1).
Various repair techniques described in the literature for proximal injuries of the coronary sinus are direct suture repair, single onlay pericardial patch repair by Aharinejad and associates, and double pericardial patch technique by Aignor and associates [46, 48, 50, 58]. The technique to treat coronary sinus ruptures are technically demanding to allow sufficient drainage through the coronary veins together with a complete hemostasis [83, 84, 85]. Direct suture repair frequently leads to stricture and distortion of the coronary sinus with increased risk for coronary sinus thrombosis [90, 91, 92].
The coronary sinus is repaired with an autologous pericardial patch that is secured with a continuous 5-0 polypropylene suture in the surrounding epicardium. A second patch is subsequently placed over the first one with an additional layer of fibrin glue in between the pericardial patches to achieve complete hemostasis. This technique avoids distortion and potential narrowing of the coronary sinus while providing adequate bleeding control [48]. Mid-portion injuries (Blow out rupture): A blowout rupture occurs in the middle portion of the coronary sinus due to balloon over-inflation or high infusion pressure [46, 47, 48, 49, 50, 51, 52, 53, 58, 59, 60]. In the case of blowout rupture, it is essential to stop the retrograde cardioplegia immediately, carry out the repair, and alter the strategy of myocardial protection [52].
When using a pericardial patch for repair, it is recommended to leave the catheter in situ to present the edges of the rupture. Weiss and associates have suggested placing a Gore-Tex conduit (WL Gore and Associates, Flag- staff, AZ), to create an alternative route between the patch and the right atrium [49]. A pericardial patch sutured directly to the edges of the rupture in most cases is technically not possible. Thus a patch anchored to the surrounding epicardium is an excellent solution to avoid this problem. A second patch may be placed over the first one to provide additional coverage with fibrin glue in between the patches for perfect hemostasis.48 Distal rupture (perforations of the coronary sinus, its radicals of the right ventricle): Rupture at the distal end of the coronary sinus, posterior cardiac vein or marginal cardiac veins are due to incorrect catheter placement, and/or hyperinflation of a catheter balloon which is advanced to the extreme end of the coronary sinus (Figure 1).
These injuries can occur during catheter manipulation with the stylet in situ. A clean and apparent injury is best repaired with 6-0 or 7-0 prolene. A small perforation of the veins may remain concealed underneath the sub- epicardial contusion [51, 54, 56, 57]. These injuries have been treated conservatively, but a delayed rupture of cardiac contusion has been reported [40, 54]. Therefore, a double layered on-lay pericardial patch is recommended to deal with this type of injury. To prevent delayed hemorrhage from a repair done on a decompressed right ventricle additional reinforcement is recommended on beating heart, before coming off cardiopulmonary bypass [84]. If overt bleeding is not present, treat conservatively [45, 46, 47]. Transesophageal echocardiography helps to detect the exact location of the injury [80]. Hematoma over the Atrio-ventricular groove: High infusion pressure can cause an atrioventricular groove hematoma and result in delayed coronary sinus rupture due to a retrocardiac chest tube. Non-expanding hematomas without hemodynamic compromise may be treated conservatively. Lacerations with expanding hematomas or hemodynamic alterations (e.g., pulmonary vein obstruction) necessitate repair with direct suture or pericardial patch [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60]. Laceration of the coronary sinus (High pressure ruptures of the coronary sinus and its tributaries): An extensive laceration of the coronary sinus is usually secondary to balloon over-inflation or over- pressurization during retrograde cardioplegia infusion (Figure 1) [24, 25]. This type of injury has been reported as a result of manual hyperinflation of a DLP Inc. catheter balloon, high flow rate through a research medical Inc. catheter with a self-inflatable balloon and due to high resistance encountered during delivery of cardioplegia through a malpositioned catheter [45, 46, 47, 48, 49, 50].
Generally, rupture of a coronary sinus through its radicals is extensive; hemorrhage extends in the sub- epicardial plane and eventually ruptures at a remote point [52]. This type of injury is difficult to control, because of the difficult access, and ill-defined edges, which are unsuitable for primary repair. It is best to repair this type of injury on a fully decompressed heart, with double layered only pericardial patch sandwiched with fibrin glue, and suture to the epicardium beyond the perimeters of the cardiac contusion, avoiding the branches of the coronary arteries [52]. Similar method may be used for the high-pressure ruptures of the coronary venous tributaries.
Prevention and Recommendations Of Management of Iatrogenic Coronary Sinus Injuries
From our experience and published literature, we recommend the following:
- Insert the coronary sinus catheter on partial bypass while the right atrium is distended.
- Check the position of the catheter at the atrioventricular groove and the base of the left atrial appendage using surgeon’s middle finger.
- If available, confirm the position by transesophageal echocardiography.
- Use the cardioplegia pump and pressure transducer to confirm the position of the catheter.
- In difficult cases, snug the superior and inferior caval veins, make a small atriotomy over the medial side of inferior caval vein - right atrial junction, 1 cm away from the atrioventricular groove. Then the catheter is placed within the coronary sinus under direct vision and secured with the atrial wall using a polypropylene suture.
- Avoid over-distension of the balloon (saline should be used instead of air because it decompresses the balloon effectively between infusions) [58].
- During balloon inflation, the delivery pressure needs to be monitored all the time, keeping it below 40 millimetre of mercury, rather than inflating the balloon to the manufacturer’s labelled volume.
- Avoid excessive retraction of the heart with the coronary sinus catheter in situ especially in the hypertrophied heart and during distal anastomoses of coronary artery bypass grafting.
- The pressure transducer for measuring coronary sinus pressures should be zeroed and set on 0- to - 40 millimetre of mercury scale.
- On instruction from the surgeon, activate the cardioplegia pump to the desired flow (125 millilitres per minute per metre square or approximately 200- 250 millilitres per minute flow).
- Monitor the coronary sinus waveform during the delivery of cardioplegia.
- During delivery of the cardioplegia, the surgical team including the anesthesiologist, the perfusionist need to ensure that the coronary sinus pressure is below 40 millimetre of mercury at all times. Conclusion Iatrogenic injuries of the coronary sinus and/or its tributaries are rarely reported, thus may be underestimated.
Unfavourable anatomic configuration, faulty catheter/electrode placement of the coronary sinus, left ventricular and septal hypertrophy and placement of electrodes for biventricular pacing remain the dominant causative factors for injury of the coronary sinus. The diagnostic accuracy is improving with the use of echocardiography and careful intraoperative examination. We have reviewed the various injury patterns, stratifying them into several categories. Management, however requires an individualized approach. Characterization of various injury patterns and their causative mechanisms will hopefully increase awareness of the existence and its management.
Financial Support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of Interest
None
References
-
Melrose DG, Dreyer B, Bentall HH, Baker JB (1955) Elective cardiac arrest. Lancet 269(6879): 21-22.
-
Buckberg GD, Brazier JR, Nelson RL, Goldstein SM, McConnell DH, et al. (1977) Studies of the effects of hypothermia on regional myocardial blood flow and metabolism during cardiopulmonary bypass. I. The adequately perfused beating, fibrillating, and arrested heart. J Thorac Cardiovasc Surg 73(1): 87-94.
-
Buckberg GD (1979) A proposed "solution" to the cardioplegic controversy. J Thorac Cardiovasc Surg 77(6): 803-815.
-
Buckberg GD (1989) Antegrade/retrograde blood cardioplegia to ensure cardioplegic distribution: operative techniques and objectives. J Cardiac Surg 4(3): 216-238.
-
Buckberg GD (1989) Recent advances in myocardial protection using antegrade/retrograde blood cardioplegia. Eur Heart J 10 Suppl H: 43-48.
-
Roe BB, Hutchinson NH, Ullyot DJ, Smith DL (1977) Myocardial protection with cold, ischemic, potassium- induced cardioplegia. J Thorac Cardiovasc Surg 73(3): 366-374.
-
Roe BB (1982) A history of clinical cardioplegia. In: Engelman RM, et al. (Eds.), A textbook of clinical cardioplegia. Mt. Kisco, NY: Futura, pp: 1-7.
-
Buckberg GD (1991) Myocardial protection during adult cardiac operations. In: AE Baue (Eds.), Glenn's Thoracic and Cardiovascular Surgery, Vol 2. East Norwalk, CT, Appleton & Lange, pp: 1417-1442.
-
Weisel RD, Goldman BS, Lipton IH, Teasdale S, Mickle D, et al. (1978) Optimal myocardial protection. Surgery 84(6): 812-821.
-
Weisel RD, Lipton IH, Lyall RN, Baird RJ (1978) Cardiac metabolism and performance following cold potassium cardioplegia. Circulation 58(3): I217-I226.
-
Bonfim V, Kaijser L, Bendz R, Sylvén C, Morillo F, et al. (1981) Myocardial protection during aortic valve replacement. Cardiac metabolism and enzyme release following continuous blood cardioplegia. Scand J Thorac Cardiovasc Surg 15(2): 141-147.
-
Lichtenstein SV, Abel JG, Panos A, Slutsky AS, Salerno TA (1991) Warm heart surgery: Experience with long cross-clamp times. Ann Thorac Surg 52(4): 1009- 1013.
-
Lichtenstein SV, Ashe KA, el Dalati H, Cusimano RJ, Panos A, et al. (1991) Warm heart surgery. J Thorac Cardiovasc Surg 101(2): 269-274.
-
Lichtenstein SV, el-Dalati H, Panos A, Slutsky AS (1989) Long cross-clamp time with warm heart surgery. Lancet 1(8652): 1443.
-
Lichtenstein SV, Salerno TA, Slutsky AS (1990) Pro: Warm continuous cardioplegia is preferable to intermittent hypothermic cardioplegia for myocardial protection during cardiopulmonary bypass. J Cardiothorac Anesth 4(2): 279-281.
-
Conti VR, Bertranou EG, Blackstone EH, Kirklin JW, Digerness SB (1978) Cold cardioplegia versus hypothermia for myocardial protection. J Thorac Cardiovasc Surg 76(5): 577-589.
-
Griepp RB, Stinson EB, Shumway NE (1973) Profound local hypothermia for myocardial protection during open-heart surgery. J Thorac Cardiovasc Surg 66(5): 731-741.
-
Cooley DA, Reul GJ, Wukasch DC (1972) Ischemic contracture of the heart: ”stone heart.” Am J Cardiol 29(4): 575-577.
-
Cunningham JN, Catinella FP, Spencer FC (1982) Blood cardioplegia- experience with prolonged cross- clamping. In: Engelman RM, et al. (Eds.), A textbook of clinical cardioplegia. Mt. Kisco, NY: Futura, pp: 241- 264.
-
Engelman RM, Rousou JH, Vertrees RA, Rohrer C, Auvil J (1980) Safety of prolonged ischemic arrest using hypothermic cardioplegia. J Thorac Cardiovasc Surg 79(5): 705-712.
-
Menasche P, Kural S, Fauchet M, Lavergne A, Commin P, et al. (1982) Retrograde coronary sinus perfusion: a safe alternative for ensuring cardioplegic delivery in aortic valve surgery. Ann Thorac Surg 34(6): 647- 658.
-
Gundry SR, Sequiera A, Razzouk AM, McLaughlin JS, Bailey LL (1990) Facile retrograde cardioplegia: transatrial cannulation of the coronary sinus. Ann Thorac Surg 50(6): 882-887.
-
Drinkwater DC, Laks H, Buckberg GD (1990) A new simplified method of optimizing cardioplegic delivery without right heart isolation. J Thorac Cardiovasc Surg 100(1): 56-63.
-
Menasche P, Subayi JB, Piwnica A (1990) Retrograde coronary sinus cardioplegia for aortic valve operations: a clinical report on 500 patients. Ann Thorac Surg 49(4): 556-564.
-
Menasche P, Subayi JB, Veyssie L, Le Dref O, Chevret S, et al. (1991) Efficacy of coronary sinus cardioplegia in patients with complete coronary artery occlusions. Ann Thorac Surg 51(3): 418-423.
-
Partington MT, Acar C, Buckberg GD, et al. (1989) Studies of retrograde cardioplegia. I. Capillary blood flow distribution to myocardium supplied by open and occluded arteries. J Thorac Cardiovasc Surg 97(4): 605-612.
-
Partington MT, Acar C, Buckberg GD, Julia PL (1989) Studies of retrograde cardioplegia. II. Advantages of antegrade/retrograde cardioplegia to optimize distribution in jeopardized myocardium. J Thorac Cardiovasc Surg 97(4): 613-622.
-
Pratt FH (1898) The nutrition of the heart through the vessels of Thebesius and the coronary veins. Am J Physiol 1(1): 86-103.
-
Blanco G, Adam A, Fernandez A (1956) A direct experimental approach to the aortic valve; II. Acute retroperfusion of the coronary sinus. J Thorac Surg 32(2): 171-177.
-
Lillehei CW, DeWall RA, Gott VL, Varco RL (1956) The direct vision correction of calcific aortic stenosis by means of a pump-oxygenator and retrograde coronary sinus perfusion. Dis Chest 30(2): 123-132.
-
Solorzano J, Taitelbaum G, Chiu RCJ (1978) Retrograde coronary sinus perfusion for myocardial protection during cardiopulmonary bypass. Ann Thorac Surg 25(3): 201-208.
-
Poirier RA, Guyton RA, McIntosh CL (1975) Drip retrograde coronary sinus perfusion for myocardial protection during aortic cross-clamping. J Thorac Cardiovasc Surg 70(6): 966-973.
-
Bhayana JN, Kalmbach T, Booth FV, Mentzer RM, Shimert G (1989) Combined anterograde retrograde cardioplegia for myocardial protection. A clinical trial. J Thorac Cardiovasc Surg 98(5 Pt 2): 956-960.
-
Salerno TA, Charrette EJP, Chiong MA (1981) Is cardioplegic re-arrest safe? Can J Surg 24(5): 483- 484.
-
Bernhard WF, Schwarz HF, Malick NP (1960) Intermittent cold coronary perfusion as an adjunct to open heart surgery. Surg Gynecol Obstet 111: 744-50.
-
Salerno TA, Christakis GT, Abel J, Houck J, Barrozo CA, et al. (1991) Technique and pitfalls of retrograde continuous warm blood cardioplegia. Ann Thorac Surg 51(6): 1023-1025.
-
Arom KV, Emery RW (1992) Coronary sinus cardioplegia: clinical trial with only retrograde approach. Ann Thorac Surg 53(6): 965-970.
-
Salerno TA, Houck JP, Barrozo CA, Panos A, Christakis GT, et al. (1991) Retrograde continuous warm blood cardioplegia: a new concept in myocardial protection. Ann Thorac Surg 51(2): 245-247.
-
Davies AL, Hammond GL, Austen WG (1967) Direct left coronary artery surgery employing retrograde perfusion of the coronary sinus. J Thorac Cardiovasc Surg 54(6): 848-855.
-
Guiraudon GM, Campbell CS, McLellan DG, Kostuk WJ, Purves PD, et al. (1986) Retrograde coronary sinus versus aortic root perfusion with cold cardioplegia: randomized study of levels of cardiac enzymes in 40 patients. Circulation 74(5): 105-115.
-
Rosenkranz ER, Vinten-Johansen J, Buckberg GD, et al. (1982) Benefits of normothermic induction of blood cardioplegia in energy-depleted hearts, with maintenance of arrest by multidose cold blood cardioplegic infusions. J Thorac Cardiovasc Surg 84(5): 667-677.
-
Chitwood WR, Sink JD, Hill RC, et al. (1979) The effects of hypothermia on myocardial oxygen consumption and transmural coronary blood flow in the potassium-arrested heart. Ann Surg 190(1): 106- 116.
-
Chitwood WR (1988) Myocardial protection by retrograde cardioplegia: coronary sinus and right atrial methods. In: Cardiac surgery: state of the art reviews; vol 2. Philadelphia: Hanley and Belfus, pp: 197-218.
-
Chitwood WR (1992) Retrograde cardioplegia: Current methods. Ann Thorac Surg 53(2): 352-355.
-
Menasche P, Piwnica A (1991) Cardioplegia by way of the coronary sinus for valvular and coronary surgery. J Am Coll Cardiol 18(2): 628-636.
-
Panos A, Salerno TA, Lichtenstein SV (1990) Continuous warm blood cardioplegia in surgery for acute post-infarction mitral insufficiency [Abstract]. J Mol Cell Cardiol 22(5): 31.
-
Panos AL, Ali IS, Birnbaum PL, Barrazo CA, al- Nowaiser O, et al. (1992) Coronary sinus injuries during retrograde continuous normothermic blood cardioplegia. Ann Thorac Surg 54(6): 1137-1138.
-
Aigner C, Wolner E, Mohl W (2006) Management of central coronary sinus ruptures using the pericardial patch repair technique. Ann Thorac Surg 81(4): 1275- 1278.
-
Weiss SJ (1994) Management of a difficult coronary sinus rupture. Ann Thorac Surg 58(2): 548-550.
-
Aharinejad S, Baumgartner H, Miksovsky A, Mohl W (1996) Closure of ruptured coronary sinus by a pericardial patch. Ann Thorac Surg 62(3): 889-891.
-
Economopoulos GC, Michalis A, Palatianos GM, Sarris GE (2003) Management of catheter-related injuries to the coronary sinus. Ann Thorac Surg 76(1): 112-116.
-
Fleisher AG, Mohan R, Sarabu MR, Reed GE (1994) Repair of coronary sinus rupture secondary to retrograde cardioplegia. Ann Thorac Surg 57(2): 476- 478.
-
Garibaldi AA (1994) Coronary sinus rupture (letter). Ann Thorac Surg 58(4): 1215-1216.
-
Guarracino F, Benussi S, Triggiani M, Oppizzi M, Donatelli F, et al. (1997) Delayed presentation of coronary sinus rupture after retrograde cardioplegia. J Cardiothorac and Vasc Anaesth 11(1): 89-90.
-
Krishnan S, Papworth DP, Farivar RS, Ueda K (2013) Identification of coronary sinus injury by transesophageal echocardiography during placement of a retrograde cardioplegia catheter for minimally invasive cardiac surgery. Anesth Analg 116(3): 560- 562.
-
Kaul TK, Fields BL, Jones CR (2000) Iatrogenic injuries during retrograde delivery of cardioplegia. Cardiovasc Surg 8(5): 400-403.
-
Kaul TK, Bain WH (1977) Radiographic appearances of implanted transvenous endocardial pacing electrodes. Chest 72(3): 323-326.
-
Kshettry VR (1996) Coronary sinus injury during retrograde cardioplegia: a report of three cases. J Card Surg 11(5): 359-362.
-
Kurusz M, Girouard MK, Brown PS (2002) Coronary sinus rupture with retrograde cardioplegia. Perfusion 17(1): 77-80.
-
Berger TJ (1994) Coronary sinus rupture (letter). Ann Thorac Surg 58: 121-1218.
-
Shapira N, Lemole GM, Spagna PM, Bonner FJ, Fernandez J, et al (1987) Antegrade and retrograde infusion of cardioplegia: assessment by thermovision. Ann Thorac Surg 43(1): 92-97.
-
Masuda M, Yonenaga K, Shiki K, Morita S, Kohno H, (1986) Myocardial protection in coronary occlusion by retrograde cardioplegic perfusion via the coronary sinus in dogs. Preservation of high-energy phosphates and regional function. J Thorac Cardiovasc Surg 92(2): 255-263.
-
Bolling SF, Flaherty JT, Bulkley BH, Gott VL, Gardner TJ (1983) Improved myocardial preservation during global ischemia by continuous retrograde coronary sinus perfusion. J Thorac Cardiovasc Surg 86(5): 659- 666.
-
Mori F, Ivey TD, Tabayashi K, Thomas R, Misbach GA (1986) Regional myocardial protection by retrograde coronary sinus infusion of cardioplegic solution. Circulation 74(5): 116-124.
-
Novick RJ, Stefaniszyn HJ, Michele RP, Burdon FD, Salerno TA (1985) Protection of the hypertrophied pig myocardium: a comparison of crystalloid, blood and Fluosol-DA cardioplegia during prolonged aortic clamping. J Thorac Cardiovasc Surg 89(4): 547-566.
-
Chowdhury UK, Rao K, Narang R, Kapoor PM, Choudhury M, et al. (2017) An alternative technique of coronary button implantation in patients undergoing modified Bentall’s procedure. J Card Crit Care 1(1): 51-54.
-
Chowdhury UK, Sheil A, Kapoor PM, Narang R, Gharde P, et al. (2016) Short-term prognostic value of perioperative coronary sinus-derived-serum cardiac troponin-I, creatine kinase-MB, lactate, pyruvate, and lactate-pyruvate ratio in adult patients undergoing open heart surgery. Ann Card Anaesth 19(3): 439- 453.
-
Shiki K, Masuda M, Yonenaga K, Asou T, Tokunaga K (1986) Myocardial distribution of retrograde flow through the coronary sinus of the excised normal canine heart. Ann Thorac Surg 41(3): 265-271.
-
Fiore AC, Naunheim KS, Kaiser GC, Willman VL, Mc Bride LK, et al. (1989) Coronary sinus versus aortic root perfusion with blood cardioplegia in elective myocardial revascularization. Ann Thorac Surg 47(5): 684-688.
-
Roberts JY, Browne RS, Roberts G (1943) Nourishment of the myocardium by way of the coronary veins. Fred Proct 2: 90.
-
Ludinghausen MV (1986) Nomenclature and distribution pattern of cardiac veins in man. In Mohl W, et al. (Eds.), Clinics of CSL Steinkopff Verlag Darmstadt Inc, Darmstadt, pp: 13-32.
-
Netter FH (1997) Atlas of human anatomy, second edition. East Hanover, NJ: Novartis, pp: 202-208.
-
Kalmbach T, Bhayana JN (1989) Cardioplegia delivery by combined aortic root and coronary sinus perfusion. Ann Thorac Surg 47(2): 316-317.
-
Schaper J, Walter P, Scheld H, Hehrlein F (1985) The effects of retrograde perfusion of cardioplegic solution in cardiac operations. J Thorac Cardiovasc Surg 90(6): 882-887.
-
Walter PJ, Flameng W, Kindl R, Podzuweit T (1988) Preservation of myocardial energy-rich phosphates by retrograde application of Bretschneider cardioplegia during aortocoronary bypass surgery. Eur J Cardiothorac Surg 2(1): 25-30.
-
Orihashi K (1992) Coronary arteries and veins. In: Oka Y, et al. (Eds.), Transesophageal Echocardiography. JB Lippincott Company, Philadelphia, pp: 227-235.
-
Lebon JS, Couture P, Rochon AG, Laliberté E, Harvey J, et al. (2010) The endovascular coronary sinus catheter in minimally invasive mitral and tricuspid valve surgery: a case series. J Cardiothorac Vasc Anesth 24(5): 746-751.
-
Manasse E, Barbone A, Gallotti R (2002) How to determine the correct placement of the retrograde cardioplegia catheter. Interactive Cardiovascular and Thoracic Surgery 1(1): 28-29.
-
Aldea GS, Connelly G, Fonger JD, Dobnick D, Shemin RJ (1992) Directed atraumatic coronary sinus cannulation for retrograde cardioplegia administration. Ann Thorac Surg 54(4): 789-790.
-
Poirier NC, Ugolini P, Pellerin M, Petitclerc R, Tardif JC (1982) Transesophageal echocardiographic evaluation of perioperative coronary sinus trauma. Ann Thorac Surg 66(2): 573-575.
-
Langenberg CJ, Pietersen HG, Geskes G, Wagenmakers AJ, Soeters PB, et al. (2003) Coronary sinus catheter placement: assessment of placement criteria and cardiac complications. Chest 124(4): 1259-1265.
-
de Cock CC, van Campen CM, Visser CA (2004) Major dissection of the coronary sinus and its tributaries during lead implantation for biventricular stimulation: angiographic follow-up. Europace 6(1): 43-47.
-
Cordell H Bahn (1991) Simplified placement of retrograde cardioplegic catheter. Ann Thorac Surg 52(4): 879-880.
-
Slater AD, Gott JP, Tobin GR II, Gray LA (1990) Management of extensive right ventricular injury or rupture. Ann Thorac Surg 49(5): 810-813.
-
Curry GR, Ullyot DJ, Wood M, Zapolanski AJ, Berry W (1991) Transesophageal echo-guided placement of coronary sinus, retrograde cardioplegia catheter. J Cardiothorac Vasc Anesth 5(6): 646.
-
Higami T, Ogawa K, Asada T, Mukohara N, Nishiwaki M (1991) Pressure monitoring of the coronary sinus during retrograde cardioplegia. Nihon Kyobu Geka Gakkai Zasshi 39(6): 848-854.
-
Frogel JK, Weiss SJ, Kohl BA (2009) Transesophageal echocardiography diagnosis of coronary sinus thrombosis. Anesth Analg 108(2): 441-442.
-
Katabathina VS, Restrepo CS, Martinez-Jimenez S, Riascos RF (2011) Nonvascular, nontraumatic mediastinal emergencies in adults: a comprehensive review of imaging findings. Radiographics 31(4): 1141-1160.
-
Reichert CLA, Visser CA, Koolen JJ, vd Brink RB, van Wezel HB, et al: (1992) Transesophageal echocardiography in hypotensive patients after cardiac operations. Comparison with hemodynamic parameters. J Thorac Cardiovasc Surg 104(2): 321- 326.
-
Ramsaran EK, Sadigh M, Miller D (1996) Sudden cardiac death due to primary coronary sinus thrombosis. South Med J 89(5): 531-533.
-
Suarez-Penaranda JM, Rico-Boquete R, Munoz JI, Rodríguez-Núñez A, Martínez Soto MI, et al. (2000) Unexpected sudden death from coronary sinus thrombosis. An unusual complication of central venous catheterization. J Forensic Sci 45(4): 920-922.
-
Neri E, Tripodi A, Tucci E, Capannini G, Sassi C (2000) Dramatic improvement of LV function after coronary sinus thromboembolectomy. Ann Thorac Surg 70(3): 961-963.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study