Mastering the Electrocardiogram to Distinguish SVT from VT with Confidence: A Mini-Review
Precisely differentiating supraventricular tachycardia (SVT) from ventricular tachycardia (VT) is paramount for optimal therapeutic management. This critical distinction often hinges on the meticulous application of validated diagnostic algorithms. Over time, diverse groups have devised numerous algorithms, each striving for improved specificity, sensitivity, and reduced complexity. To facilitate differentiation, we provide a concise overview of these algorithms within this document.
Introduction
Wide complex tachycardia (WCT) is characterized by a cardiac dysrhythmia exceeding 100 beats per minute, accompanied by a QRS complex duration of 120 milliseconds or greater. The primary challenge encountered in emergency settings pertains to the differentiation of supraventricular tachycardia (SVT) from ventricular tachycardia (VT), a distinction of paramount importance for therapeutic decision-making. Different groups have described different algorithms with improved specificity or sensitivity and reduced complexity over time. We briefly described the various algorithms here to differentiate the same.
Discussion
Wide complex tachycardias (WCTs) are traditionally categorized into regular and irregular forms, with irregularity defined as a beat-to-beat variation in tachycardia cycle length exceeding 40 milliseconds. Table 1 comprehensively enumerates the most frequently observed etiologies of WCTs. A crucial element in differentiating ventricular tachycardia (VT) from supraventricular tachycardia (SVT) lies in the detailed history and physical examination, the salient features of which are depicted in Table 2.
| Regular | Irregular |
| Ventricular tachycardia (80% of WCT)SVT with aberrancy (2nd most common)SVT with BBBSVT with drug or electrolyte-induced QRS wideningAntidromic AVRT (1-5%)PMT | Pre-excited AFIrregular SVT with aberrancyVT in first few seconds, on antiarrhythmic therapy – cycle length variation |
Table 1: Clinical differentiation of wide-complex tachycardia. Note: WCT – wide complex tachycardia, MI – myocardial infarction,
- Note: WCT – wide complex tachycardia, SVT – supraventricular tachycardia, BBB – bundle branch block, AVRT – atrioventricular reciprocating tachycardia, PMT – pacemaker-mediated tachycardia, AF – atrial fibrillation, VT – ventricular tachycardia.
- Clinical differentiation of WCTs
- History of heart disease
- •
- Prior MI (98% PPV for VT)
- •
- Angina or CHF (near 100% PPV for VT)
- Age > 35years (92% PPV for VT)
- History of previous recurrent episodes (>3 years history) - SVT likely
- Haemodynamically unstable – VT likely
- Examination for atrioventricular dissociation
- Termination of tachycardia with physical manoeuvres and AVN blockers - SVT likely
Table 2: Clinical differentiation of wide-complex tachycardia.
The Basic principles of various algorithms are (Table 3):
| Comments | Exceptions | |
|---|---|---|
| QRS duration | QRSd of >160mS with LBBB and >140mS with RBBB – likely VT >120 mS in structurally normal heart | Antiarrhythmic drug effect, Fascicular VT Upper septal VT |
| QRS axis | North-west axis – likely VT RBBB with LAD or LBBB with RAD - likely VT | Complex congenital heart disease Cardiac malposition |
| Concordance | Positive or negative - likely VT | The left posterior accessory pathway might have positive concordance |
| Morphological criteria | Discussed in subsequent images | |
| Ambiguous chest lead pattern | Atypical LBBB or RBBB – likely VT | Bundle branch re-entrant VT |
| Q wave | Q wave during tachycardia – likely VT, suggests old MI | Pre-excited tachycardia with posterior pathways – may have inferior lead Q wave |
| AV dissociation | Most specific, low sensitivity (20-50%) Clues: Irregular Cannon a wave Variable S1 intensity Variation in systolic blood pressure unrelated to respiration QRS amplitude variation during VT V more than A Fusion or capture beat | Slower VT might have 1:1 conduction (V=A) AF/ VT coexistence – AVD can not be diagnosed |
Table 3: Parameters helping in the differentiation of SVT vs VT. Note: WCT – wide complex tachycardia, SVT – supraventricular tac
Table 3: Parameters helping in the differentiation of SVT vs VT. Note: WCT – wide complex tachycardia, SVT – supraventricular tachycardia, VT – ventricular tachycardia, CHF – congestive heart failure, RBBB – right bundle branch block, LBBB – left bundle branch block, LAD – left axis deviation, RAD – right axis deviation, AVD – atrioventricular dissociation.
QRS Duration
Ventricular tachycardia (VT) typically presents with a widened QRS duration (>120 ms) due to the slower conduction properties of the myocardium compared to the specialised His-Purkinje system. Cell-to-cell conduction within the ventricular muscle further delays depolarisation, manifesting as the extended QRS complex. However, exceptions exist:
Fascicular VT: Originating from the conduction system itself, fascicular VT can exhibit a narrower QRS duration due to the relatively faster conduction in these specialized tissues.
Upper septal VT: Early capture of the His-Purkinje system by VT originating near the atrioventricular node can also result in a narrow QRS complex due to rapid activation of the conduction system.
QRS Axis
Normal ventricular depolarization follows a left anterior vector due to the anatomical arrangement of the conduction system. VT, originating directly from the ventricular myocardium, disrupts this activation pattern and alters the QRS axis. A shift of the QRS axis by more than 40 degrees compared to normal suggests VT. Notably, a northwest QRS axis, directly opposite the usual left anterior vector, is highly suggestive of VT as it cannot occur in normal antegrade (atrium to ventricle) conduction.
Concordant Pattern
Uniform QRS morphology across all precordial leads, either all positive (positive concordance) or all negative (negative concordance), indicates a free wall (non-septal) origin of the tachycardia, implying VT.
Atrioventricular Dissociation (Figure 1): The absence of a consistent relationship between atrial and ventricular rates is known as atrioventricular (AV) dissociation. In VT, the ventricular rate often exceeds the atrial rate due to an independent automatic focus or re-entrant circuit within the ventricles. This finding strongly supports the diagnosis of VT.
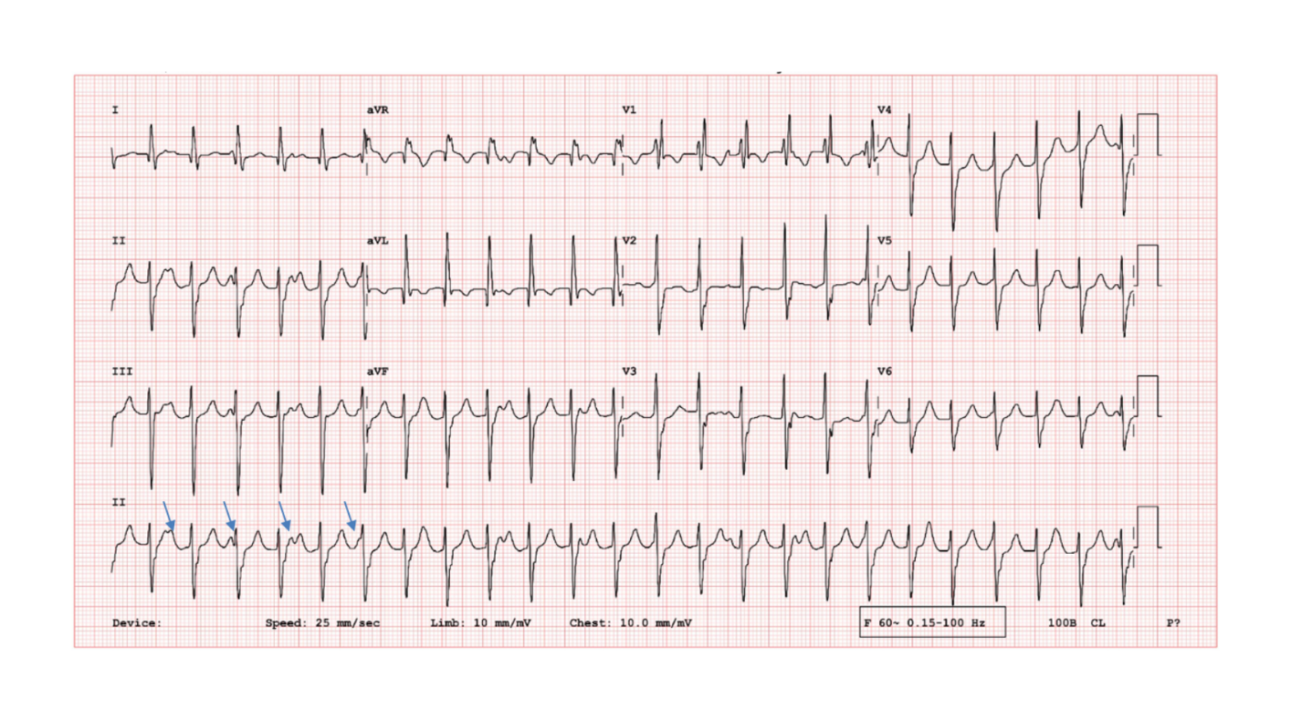
Figure 1: 12-lead electrocardiogram showing regular WCT with AV dissociation. Note that the ventricular rate is higher than atrial rate (arrows). Relatively narrower complex, RBBB and superior axis suggestive of posterior fascicular VT. Note: WCT – wide complex tachycardia, RBBB – right bundle branch block, VT – ventricular tachycardia, AV – atrioventricular.
aVR or Lead II Changes (Figures 2 & 3): Initial myocardial activation in VT is relatively slow, followed by rapid conduction through the specialized tissues during the terminal portion of the QRS complex. This phenomenon manifests as a lower voltage in the initial 40 ms of the QRS complex compared to the terminal 40 ms, particularly noticeable in leads aVR and II. The Vereckei aVR algorithm and Pava’s lead II criteria leverage this feature to support the diagnosis of VT [1, 2, 3].
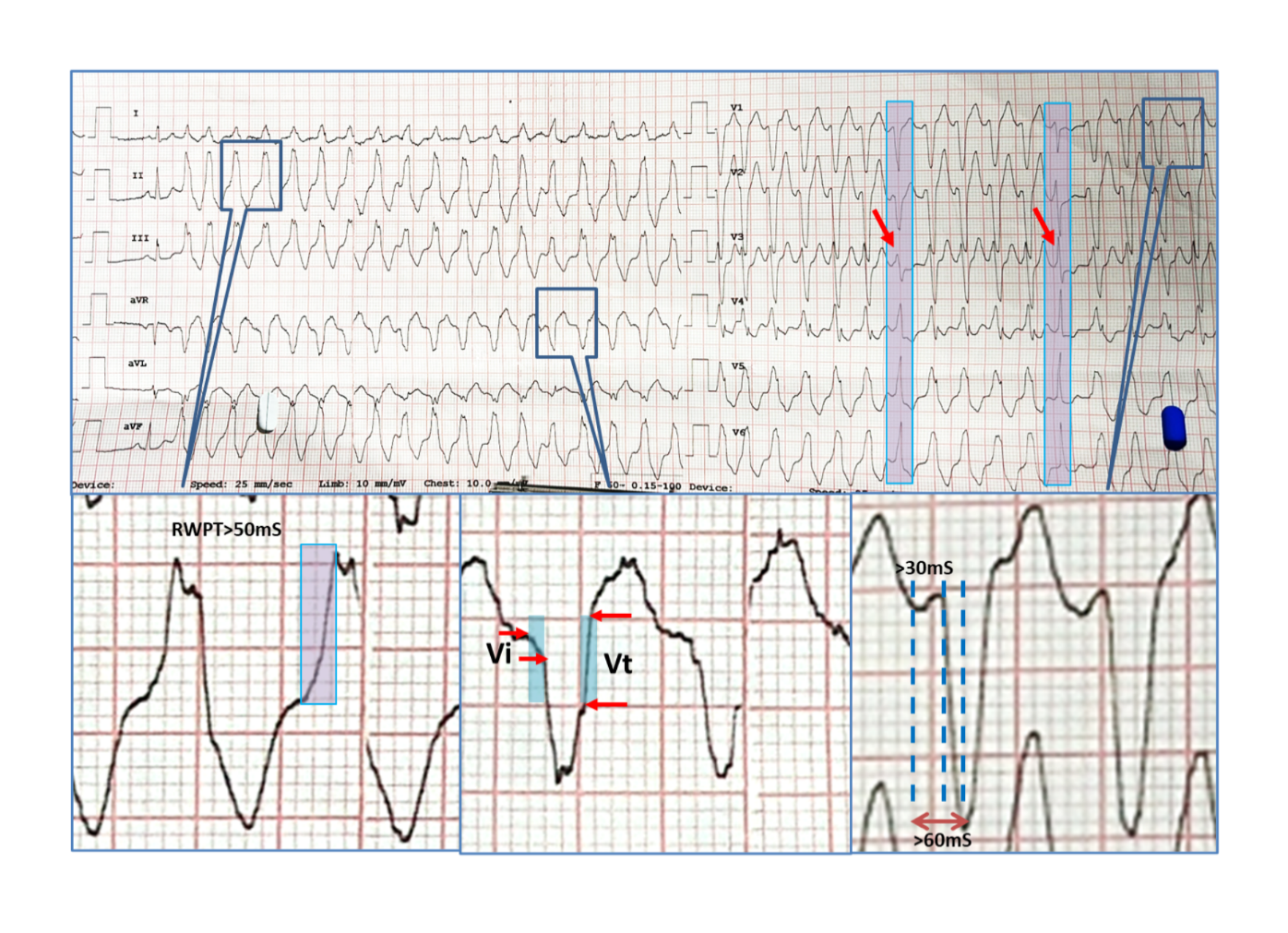
Figure 2: 12-lead electrocardiogram showing regular wide complex tachycardia initiating with PVC after the first sinus beat. Fusion beat (first arrow) and capture beat (next arrow) were present. RWPT was 80mS (>50mS), Vt>Vi in lead aVR. Lead V1 was having LBBB morphology with QRS onset to nadir of S was nearly 110mS. All these morphological criteria point towards ventricular tachycardia. It was case of right ventricular outflow tachycardia on electrophysiological study.
![Figure 3: Diagnostic approaches and algorithms [1-5]. Note: SVT – supraventricular tachycardia, VT – ventricular tachycardia, RBBB – right bundle branch block, LBBB – left bundle branch block, AV – atrioventricular, Sen – sensitivity, Sp – specificity.](/fulltextimages/12035/fig_3.png)
These ECG criteria, when considered collectively, can significantly enhance the accuracy of VT diagnosis in the setting of wide-complex tachycardia. However, it is crucial to emphasize that these features are not absolute, and interpretation should be done with caution in conjunction with the clinical context and other diagnostic modalities.
A comprehensive representation of the diverse criteria and their practical application is provided in Table 4 and Figures 1-3 [1, 2, 3, 4, 5]. Algorithmic assessment involves the sequential interrogation of specific questions, with an affirmative response to any query culminating in the categorization of the tachycardia as ventricular in origin. Notably, during morphological evaluation, a predominantly Diagnostic algorithms for wide complex tachycardia negative QRS complex in lead V1 is classified as exhibiting left bundle branch block (LBBB) morphology. In contrast, a positive complex is designated as right bundle branch block (RBBB) morphology, even in instances where traditional criteria for these conduction disturbances are not fully satisfied.
- •
- AV dissociation - VT
- •
- QRS width > 140ms - VT
- •
- Left axis deviation > -30 degrees - VT
- •
- RBBB morphology:
- Monophasic R, qR, QR, RS in V1 or
- R/S < 1 in V6 - VT, monophasic R, QR, QS in V6
- •
- LBBB morphology: qR, QS in V6
- Wellen (1978)
- •
- AV dissociation
- •
- Ventriculoatrial block
- •
- Positive QRS concordance
- •
- Northwest QRS axis
- •
- LBBB with RAD (> +90)
- •
- QRS duration > 140ms for RBBB morphology and >160ms for LBBB morphology
- •
- Dissimilar QRS morphology during tachycardia compared to baseline bundle branch block
- Akhtar (1988)
- •
- Absence of RS complex in all precordial leads - VT
- •
- Longest R/S interval > 100ms in any precordial lead - VT
- •
- AV dissociation - VT
- •
- RBBB morphology: monophasic R or qR in V1; R taller than R’; rS or QS in V6 - VT
- •
- LBBB morphology: initial R >30ms; slurred or notched S in V1 or V2; qR or QS in V6 - VT
- Griffith (1994)
- Consider VT as the default diagnosis if classical LBBB/RBBB features are absent
- Brugada (1991)
- •
- Bayesian diagnostic algorithm with following criteria:
- QRS width (< 0.14, 0.14 to 0.16, > 0.16 sec)
- QRS axis (left, right, northwest, none of the above)
- V1 morphology in RBBB pattern (taller left peak, biphasic Rs or qR, triphasic rsR’ or rR’, none of the above)
- V1 or V2 morphology in LBBB pattern (r > 40 msec, notched S downstroke, delayed S nadir > 60 msec, none of the above)
- Interval to intrinsicoid deflection in V6 (≥0.08 sec, >0.04 sec)
- V6 morphology (monophasic QS, biphasic rS, Triphasic qRs, none of the above) Precordial concordance and AV dissociation
- Lau (2000)
- Step 1: A-V dissociation present - VT
- Step 2: Initial R wave in aVR - VT
- Step 3: QRS morphology unlike bundle branch block or fascicular block
- Step 4: Vi/Vt < 1
- Vereckei (2007)
- In lead aVR:
- Step 1: Initial R wave in aVR - VT
- Step 2: Width of an initial r or q wave > 40ms
- Step 3: Notching on the initial downstroke of a predominantly negative QRS complex
- Step 4: Vi/Vt < 1
- Pava (2010)
- R wave peak time in lead II > 50ms suggestive of VT aVR Vereckei (2008)
Table 4: Diagnostic approaches and algorithms.
Conclusion
Accurate differentiation between supraventricular tachycardia (SVT) and ventricular tachycardia (VT) is crucial for optimal therapeutic decision-making, and can often be achieved through the meticulous application of validated diagnostic algorithms. However, even with rigorous evaluation, definitive rhythm diagnosis may remain elusive in certain cases. When faced with such ambiguity, a prevailing recommendation suggests treating the rhythm as VT due to the potentially catastrophic consequences of mistaking VT for SVT.
References
-
Vereckei A, Duray G, Szénási G, Altemose GT, Miller JM (2007) Application of a new algorithm in the differential diagnosis of wide QRS complex tachycardia. European Heart Journal 28(5): 589-600.
-
Vereckei A, Duray G, Szénási G, Altemose GT, Miller JM (2008) New algorithm using only lead aVR for differential diagnosis of wide QRS complex tachycardia. Heart Rhythm 5(1): 89-98.
-
Pava LF, Perafán P, Badiel M, Arango JJ, Mont L, et al. (2010) R-wave peak time at DII: a new criterion for differentiating between wide complex QRS tachycardias. Heart Rhythm 7(7): 922-926.
-
Brugada P, Brugada J, Mont L, Smeets J, Andries EW (1991) A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation 83(5): 1649-1659.
-
Jastrzebski M, Kukla P, Czarnecka D, Kawecka Jaszcz K (2012) Comparison of five electrocardiographic methods for differentiation of wide QRS-complex tachycardias. EP Europace 14(8): 1165-1171.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study