Role of Closure of Patent Foramen Ovale in Children with Cryptogenic Stroke: Incidence, Evidence and Guidelines
Patent foramen ovale (PFO) is post-natal persistence of interatrial communication and have shown to have association with various clinical manifestations including transient ischemic attack and strokes. The diagnosis of PFO requires transthoracic and transesophageal Echocardiogram. Closure of PFO with percutaneous device closure can prevent recurrence of strokes in selected patients with cryptogenic stroke and it has been included in recent guidelines also. In this mini review, we will discuss couple of cases of PFO closures followed by discussion upon recent guidelines on the same.
Abbreviations
PFO: Patent Foramen Ovale; TIA: Transient Ischemic Attack; ASD: Atrial Septal Defect; TOE: Trans Esophageal ECHO; TTE: Trans Thoracic ECHO.
Introduction
Patent foramen ovale (PFO) is persistent interatrial shunt with autopsy prevalence of as high as 27% [1]. PFO have been shown to be associated with migraine, decompression sickness, platypnea-orthpnea syndrome and even transient Ischemic Attack (TIA) or stroke. In cases involving brain infarction of indeterminate cause in young people, PFO has been confirmed in 40% of the cases [2]. We report 2 cases of cryptogenic strokes which were diagnosed with PFO during further evaluation.
Case Study
Case no. 1
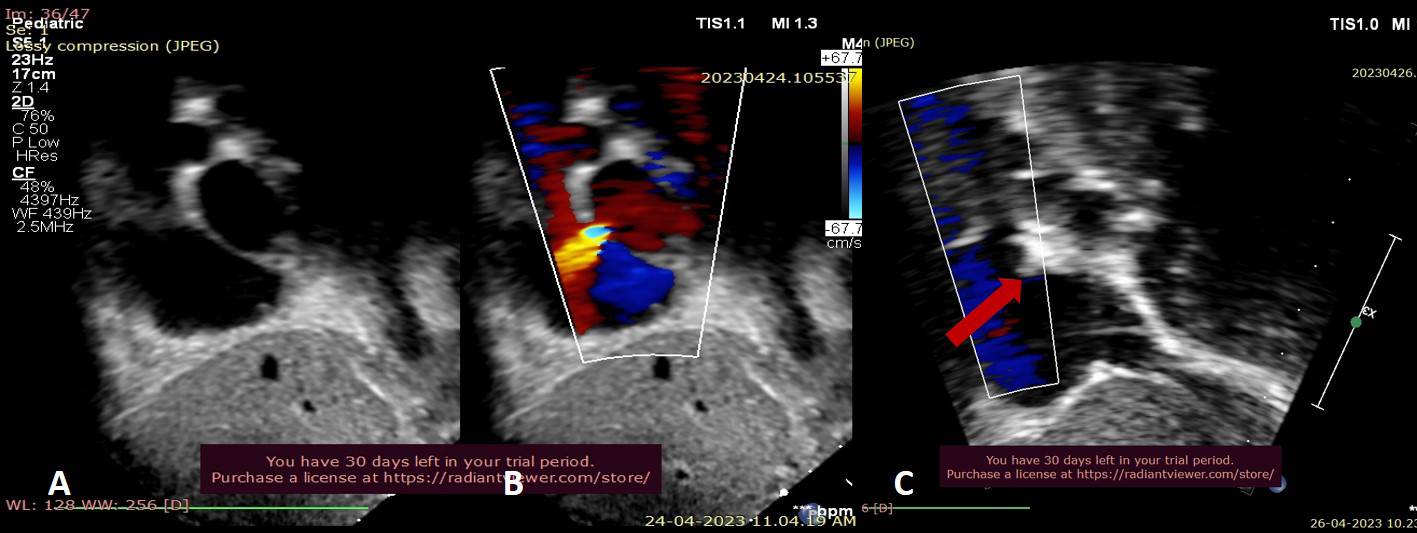
An 8 year old girl had history of transient weakness of right half of body without loss of consciousness and each episode was lasting for about 30 minutes. She had 4 such episodes in last 2 years. Further workup showed normal brain MRI and electroencephalogram (EEG) but, echocardiogram showed small (4mm) Fossa ovalis atrial septal defect (ASD) with left to right shunt (Figure 1) and no other cardiac anomaly. She was started on Aspirin at antiplatelet doses in view of frequent episodes of TIA. She underwent device closure of ASD in April 2023 and is on follow up. At 1year after the procedure, she is asymptomatic and off Aspirin.
Case no. 2
13year old boy had an episode of TIA in the form of right sided hemiparesis and heaviness in tongue. The episode lasted for 10 minutes with spontaneous recovery. He underwent MRI brain which was inconclusive and sleep and awake EEG was normal. Echocardiogram was suggestive of 5mm fossa ovalis atrial septal defect with no other cardiac structural defect. He was started on tab Aspirin and subsequently underwent successful ASD device closure. He is on follow up for 9 months after the procedure and there are no further episode of TIA.
Discussion
PFO is a remnant of normal fetal circulation, causing apparently no symptoms in infancy and can persist into adult life. The majority of the adults with PFO remain asymptomatic but transient episodes of right or left shunting across PFO exposes them to potential risks of cryptogenic stroke, acute embolic limb ischemia, migraine, decompression sickness and platypnea-orthopnea syndrome [3]. For the diagnosis of PFO, is highly specific but less sensitive and trans esophageal ECHO (TOE) is gold standard. In multi-centric Child-PFO study by Miton N, et al. [4] 41 children had underwent PFO closure out of which 31 were for TIA/stroke and none of their patients had delayed complications or recurrence of stroke during median follow up of 568 days [4]. 3 landmark trials RESPECT, REDUCE and CLOSE were major turning points after which PFO closure has been recommended by multiple guidelines like European Society of Cardiology published in Eurointervention (2018) and American Heart Association published in 2021 [3, 5]. 2021 AHA guidelines recommend PFO closure in patients with non-lacunar cryptogenic ischemic stroke after multidisciplinary team discussion [5].
Some of the clues of PFO being possible etiology for paradoxical embolic events include stroke at high altitude or during decompression, event that occurs shortly after Valsalva maneuver, the presence of atrial septal aneurysm or, large PFO with significant shunt and these patients should be considered for PFO closure after multidisciplinary team discussion.
Conclusions
The majority of the patients with PFO remain asymptomatic but few may develop critical and at times fatal symptoms. Patients with stroke require multidisciplinary team approach involving Pediatricians, Cardiologists, Neurologists etc, and about 50% of patients with cryptogenic stroke can have PFO. TOE is gold standard for the diagnosis of PFO and PFO closure can help in reducing risk of recurrent stroke in patients with cryptogenic stroke.
Conflicting Interest: None
References
-
Hagen PT, Scholz DG, Edwards WD (1984) Incidence and size of patent foramen ovale during the first 10 decades of life: an autopsy study of 965 normal hearts. Mayo Clin Proc 59(1): 17-20.
-
Lechat P, Mas JL, Lascault G, Loron P, Theard M, et al. (1988) Prevalence of patent foramen ovale in patients with stroke. N Engl J Med 318(18): 1148-1152.
-
Pristipino C, Sievert H, D’Ascenzo F, Mas JL, Meier B, et al. (2021) European position paper on the management of patients with patent foramen ovale. General approach and left circulation thromboembolism. Eur Heart J 40(38): 3182-3195.
-
Miton N, Godart F, Milani G, Jalal Z, Karsenty C, et al. (2020) Patent foramen ovale closure in children without cardiopathy: Child-PFO study. Archives of Cardiovascular Diseases 113(8-9): 513-524.
-
Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, et al. (2021) Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 52(7): e364-e467.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study