Efficacy and Safety of a Novel Nanosomal Docetaxel Lipid Suspension as an Anticancer Agent - A Retrospective Study
This retrospective study evaluated the efficacy and safety of nanosomal docetaxel lipid suspension (NDLS; DoceAqualip®) in advanced solid tumors. Medical charts of adults with solid tumors treated with DoceAqualip® (75-100mg/m2 IV q3week) at Noora Hospital between June 2014 and June 2016 were analyzed. Of 69 patients, 54% were men; majority had stages III (47.82%) and IV (31.88%) cancer; gastric adenocarcinoma was most common (34.8%) type. Efficacy data was available for 56 patients, which showed best overall response in 58.9% (BOR; complete response [CR, 12.5%] + partial response [PR, 46.4%], p
Introduction
Docetaxel is one of the most active and extensively used cytotoxic agent for the treatment of several types of cancers including locally advanced or metastatic breast cancer, non-small-cell lung cancer, hormone refractory prostate cancer, head and neck cancer and advanced gastric cancer [1]. The most common challenge with conventional docetaxel formulation is the requirement of corticosteroid premedication to prevent severe hypersensitivity reactions, fluid retention, fatal anaphylaxis, and infusion related toxicities due to the use of polysorbate 80 [1, 2, 3, 4, 5].
Several novel formulations such as taxane analogues and prodrugs, nanoparticle-aptamer bioconjugate, albumin nanoparticles, polyglutamates, emulsions, liposomes, docetaxel fibrinogen-coated olive oil droplets and submicronic dispersion have been developed to eliminate the toxicities of the carrier used in docetaxel formulations [6]. However, most of these agents are in the development stages. The novel nanosomal docetaxel lipid suspension (NDLS; DoceAqualip®) is the only such novel formulation approved and is being used for the treatment of several cancers. DoceAqualip® has nano-carriers in suspension form composed of lipids Generally Regarded As Safe (GRAS) by the US FDA based on the ‘Aqualip’ technology, which eliminates the need for polysorbate 80 and ethanol, and thus, associated hypersensitivity reactions and infusion-related toxicities [7, 8]. Furthermore, corticosteroid premedication is not needed due to the negligible risk of hypersensitivity reactions with DoceAqualip® administration as compared with the conventional docetaxel formulations [9]. The novel ‘Aqualip Technology’ is patented in Europe, Japan and Canada, while the filed US patent is under review.
DoceAqualip® has demonstrated good response rates and better tolerability than conventional docetaxel in locally advanced or metastatic breast cancer [8]. DoceAqualip® has been approved by the Drug Controller General of India (DCGI) for the treatment of breast cancer, hormone refractory prostate cancer, gastric adenocarcinoma, squamous cell carcinoma of the head and neck, and non-small cell lung cancer. The current retrospective analysis in advanced solid tumors was conducted to further evaluate the efficacy, safety of the novel formulation of docetaxel i.e., DoceAqualip® in real life scenario.
Methods
Study Population
Patients of either sex, ≥18 years of age, with histopathologically or cytologically confirmed tumors and an Eastern Cooperative Oncology Group (ECOG) performance status score of 0-2 [10], and at least 1 measurable lesion according to Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 criteria [11], who were treated with DoceAqualip® as part of their clinical care between June 2014 and June 2016, were included in the analysis.
The study protocol was approved by the Institutional Ethics Committee of Noora Hospital, Umer Abad, Zainakote, Srinagar. This study was conducted in accordance with the ethical principles that have their origin in the Declaration of Helsinki, and in accordance with the International Conference on Harmonization’s Good Clinical Practice guidelines, applicable regulatory requirements, and in compliance with the protocol.
Study Design
This study evaluated the medical records retrospectively to analyze the efficacy and safety of DoceAqualip® in patients who had received 1-hour intravenous infusion of DoceAqualip® every 3 weeks at a dose determined by the physicians (range: 75 to 100 mg/m2) according to the tumor type. The data of the patients considered for this analysis included those who underwent treatment between June 2014 and June 2016 at Noora Hospital, Umer Abad, Zainakote, Srinagar. The patients received a maximum of 6 cycles of DoceAqualip®. The follow-up data till August 2016 was used for the analysis.
Study Assessments
Efficacy
The primary efficacy evaluation was the best overall response rate (BOR), defined as the total number of patients showing complete response (CR) and partial response (PR). The secondary efficacy endpoint was the disease control rate (DCR), defined as the total of BOR and patients with stable disease (SD). Patients without a confirmed CR, PR or SD were considered as failure in computing the BOR. The RECIST 1.1 criteria was used to assess the disease status and tumor response. Safety Safety evaluation was based on ECOG, hepatic screening, hematology, biochemistry, and urine analysis. Incidences of adverse events (AEs) were recorded during every cycle and graded according to the National Cancer Institute Common Toxicity Criteria 4.02 [12]. Data on death and discontinuations were collected throughout the study [12]. Statistical analyses Demographic and baseline characteristics were summarized descriptively. Response rate was evaluated as per RECIST 1.1 criteria and presented as frequency and percentage of patients for CR, PR, SD, and progressive disease (PD) categories. Chi-square test was used to compare the distribution of patients in each category. Overall response was evaluated using computerized tomography (CT), magnetic resonance imaging (MRI), ultrasonography (USG), tumor markers and endoscopy (esophagus/stomach). Adverse events (AEs) were summarized by System Organ Class (SOC) and Preferred Term (PT). The AEs were summarized as frequencies and percentages by type of reactions.
Results
Patients Disposition and Demographics
A total of 69 patients received DoceAqualip® between June 2014 and June 2016, and were included in the study. The baseline characteristics of the patients are summarized in Table 1. Overall, 47.82% (33/69) patients had stage III disease and 31.88% (22/69) had stage IV disease. Gastric adenocarcinoma was the most common (24/69, 34.8%) cancer, followed by ovarian cancer (14/69, 20.3%), and non-small cell lung cancer (13/69, 18.8%). Metastatic was the most common setting in which DoceAqualip was used (28/69, 40.57%).
| Parameters | DoceAqualip®(N=69) |
| Age (years), Mean (SD) | 55.2 (14.9) |
| Sex | |
| Men, n (%) | 37 (53.6) |
| Women, n (%) | 32 (46.4) |
| Setting, n (%)† | |
| Neo-Adjuvant | 24 (34.78) |
| Adjuvant | 14 (20.28) |
| Metastatic | 28 (40.57) |
| Cancer Stage, n(%)‡ | |
| Stage I | 4 (5.79) |
| Stage II | 2 (2.89) |
| Stage III | 33 (47.82) |
| Stage IV | 22 (31.88) |
| Type of Cancer, n (%) | |
| Breast cancer | 7 (10.1) |
| Gastric adenocarcinoma | 24 (34.8) |
| Hormone refractory prostate cancer | 3 (4.3) |
| Non-small cell lung cancer | 13 (18.8) |
| Esophagus carcinoma | 2 (2.9) |
| Soft tissue sarcoma | 3 (4.3) |
| Urinary bladder cancer | 2 (2.9) |
| Small cell lung cancer | 1 (1.4) |
| Ovarian cancer | 14 (20.3) |
Table 1: Patient Disposition and Baseline Characteristics.
Efficacy
The efficacy evaluation data was available for 56 patients with data missing for 13 patients. The BOR was achieved in 33/56 (58.9%) patients (CR: 7 [12.5%], PR: 26 [46.4%], p<0.0001; Table 2). The DCR was 98.2% (CR: 7 [12.5%], PR: 26 [46.4%], SD: 22 [39.3%], p<0.0001) and only 1 patient had PD. The highest BOR (100%) was reported in urinary bladder cancer and DCR (100%) in hormone refractory prostate cancer, urinary bladder cancer and soft tissue sarcoma. For a pool of all 69 patients, the BOR was 47.82% (CR, 10.14% + PR, 37.68%; p<0.0001), and DCR was 79.71% (p<0.0001); 1 patient had PD and efficacy response was not available for 18.9% patients. Median follow-up period was 13 weeks (range: 7-34 weeks).
| Overall Response | ||||||||
|---|---|---|---|---|---|---|---|---|
| Outcome | CR | PR | SD | PD | BOR | DCR | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||
| No. (%) of Patients (N=56) | 7 (12.5) | 26 (46.4) | 22 (39.3) | 1 (1.8) | 33 (58.9) | 55 (98.2) | ||
| No. (%) of Patients (N=69) | 7 (10.1) | 26 (37.7) | 22 (31.9) | 1 (1.4) | 33 (47.8) | 55 (79.7) | ||
| By Type of Cancer | ||||||||
| Cancer Type | CR | PR | SD | PD | BOR | DCR | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Breast cancer (n=7) | 1 (14.28) | 2 (28.57) | 2 (28.57) | 0 | 3 (42.85) | 5 (71.42) | ||
| Esophagus cancer (n=2) | 0 | 0 | 1 (50) | 1 (50) | 0 | 1 (50) | ||
| Ovarian cancer (n=14) | 4 (28.57) | 4 (28.57) | 3 (21.42) | 0 | 8 (57.14) | 11 (78.57) | ||
| Gastric adenocarcinoma (n=24) | 0 | 13 (54.16) | 6 (25) | 0 | 13 (54.16) | 19 (79.16) | ||
| Hormone refractory prostate cancer (n=3) | 0 | 1 (33.33) | 2 (66.66) | 0 | 1 (33.33) | 3 (100) | ||
| Non-small cell lung cancer (n=13) | 1 (7.69) | 4 (30.76) | 6 (46.15) | 0 | 5 (38.36) | 11 (84.61) | ||
| Urinary bladder cancer (n=2) | 1 (50) | 1 (50) | 0 | 0 | 2 (100) | 2 (100) | ||
| Soft tissue sarcoma (n=3) | 0 | 1 (33.33) | 2 (66.66) | 0 | 1 (33.33) | 3 (100) |
Table 2: Efficacy Evaluation of NDLS.
Safety & Tolerability
At least 1 AE was reported in 45 out of 69 (65.2%) patients during the study. Of the total 371 postdose AEs, 198 (53.4%) were of Grades 1 to 3 and 77 (20.8%) were of Grade >3. Primary hematologic toxicity was neutropenia with anemia (66 episodes, n=29 [Grades 1 to 3: 51 {77.3%}; Grade >3: 15 {22.7%}]), followed by isolated neutropenia (47 episodes, n=17 [Grades 1 to 3: 30 {63.8%}; Grade >3: 17 {36.2%}]) and isolated anemia (15 episodes, n=5 [Grades 1 to 3: 7 {46.7%}; Grade >3: 8 {53.3%}).
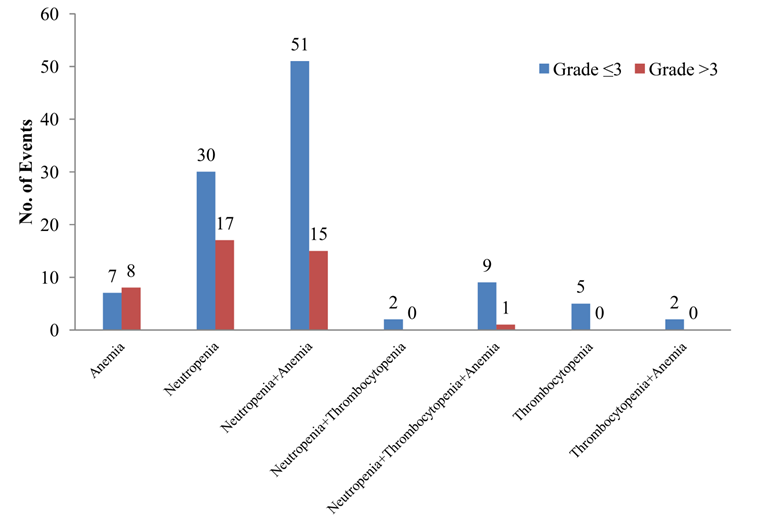
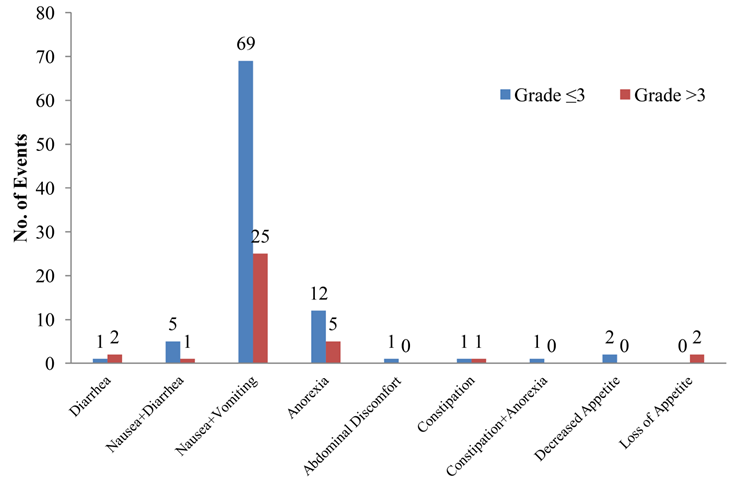
Among nonhematological toxicities, nausea with vomiting was the most commonly observed AE (94 episodes, n=33 [Grades 1 to 3: 69 {73.4%}; Grade >3: 25 {26.6%}]). No events of peripheral neuropathy, allergic reactions, or death were reported. Figures 1 and 2 represents the number of AEs that occurred along with their severity. Other AEs (96 out of 371) observed were hyperpigmentation, anorexia, fatigue, body ache, and back pain, but were not clinically significant.
Granulocyte colony-stimulating factor (G-CSF) support was not required with DoceAqualip® monotherapy (n=6) at a dose of 75 mg/m2. In total, 20 patients receiving triplet chemotherapy (DoceAqualip® in combination with platinum derivative, 5-fluorouracil, gemcitabine or capecitabine) required G-CSF support. Average 2 to 3 doses of 300 µg filgrastim were sufficient to maintain the counts in an acceptable range. In one patient who received doublet chemotherapy (DoceAqualip® plus carboplatin) for non-small cell lung cancer, febrile neutropenia was encountered after the third cycle of chemotherapy. This patient recovered after receiving 300 µg filgrastim for 6 consecutive days. Patients receiving doublet chemotherapy containing gemcitabine 1000- 1200 mg/m2 (n=4) required 2 to 3 doses of 300 µg filgrastim to keep the counts in an acceptable range during subsequent cycles. Patients receiving DoceAqualip® in combination with doublet chemotherapy containing capecitabine did not require G-CSF support for the first 2 cycles of chemotherapy (n=3); after the third cycle, 300 µg of filgrastim for 2 days was administered to maintain the counts at an acceptable level for additional cycles Table 3.
| G-CSF Support in patients who received | Patients | G-CSF support | Average dose of G-CSF | ||||||
|---|---|---|---|---|---|---|---|---|---|
| DoceAqualip based regimen | (N) | (300 µg) required | |||||||
| DoceAqualip® monotherapy | 6 | 0 | 0 | ||||||
| Triplet platinum-containing chemotherapy | 20 | 20 | 2 to 3 | ||||||
| Doublet platinum-containing chemotherapy | 38 | 38 | 6 | ||||||
| Doublet gemcitabine-containing chemotherapy | 4 | 4 | 2 to 3 | ||||||
| Doublet capecitabine-containing regimen | 3 | 3 | 2 | ||||||
| Doublet or triplet non-platinum, non-gemcitabine therapy | 5 | 5 | 2 to 3 |
Table 3: Requirement of G-CSF Support with NDLS (alone or in combination with other agents).
Discussion
The conventional docetaxel formulation (Taxotere®) is a widely used agent in the management of different types of solid tumors, including prostate, non-small cell lung, breast, and head and neck cancer in the advanced settings either as a single agent or in combination with other agents [1]. The surfactant polysorbate 80 used in the conventional docetaxel formulation is known to cause hypersensitivity, fatal anaphylaxis, and infusion related toxicities, which warrant anti-allergic treatment and corticosteroid premedication. However, corticosteroids are also known to cause hyperglycemia and increased episodes of infectious complications [13, 14]. Furthermore, the ethanol content in the marketed formulation of docetaxel can cause a state like that of intoxication and driving or operating machinery need to be avoided for at least one to two hours after an infusion. Also, pain relievers or sleep aids may interact with ethanol in the docetaxel infusion and worsen the intoxicating effects [15]. Hence, the solvent (polysorbate 80 and ethanol) free GRAS lipid formulation of docetaxel, DoceAqualip® was developed to eliminate these AEs or at least decrease the risk of AEs to negligible proportions, thereby totally eliminating the need of corticosteroid premedication [8].
Ahmad et al., also conducted a randomized comparative study to assess the efficacy and safety of DoceAqualip® with Taxotere® in metastatic breast cancer patients. DoceAqualip® administered via I.V. infusion over 1 hour (10-minute deviation was allowed) at a dose of 75 mg/m2, demonstrated higher overall response rate (CR+PR) rate compared to Taxotere® (35.5% vs. 26.3%). The safety profile was comparable for DoceAqualip® and Taxotere® despite the fact that there was no corticosteroid premedication in the DoceAqualip arm [8].
Furthermore, published reports have highlighted the use of DoceAqualip® in several other cancers including prostate, ovarian, cervical and penile cancers [13, 16, 17, 18]. A panel of oncology experts across India opined that DoceAqualip® has shown better therapeutic outcomes compared with the conventional formulations and is useful in patients with metastatic disease and those at risk of hypersensitivity reactions, diabetes and patients in whom steroid needs to be avoided [19].
The current retrospective analysis was performed to assess the efficacy and safety of DoceAqualip® in several types of advanced cancer. Overall, the results demonstrated that DoceAqualip® has an acceptable safety profile and antitumor activity in patients with different solid tumors including breast cancer, gastric adenocarcinoma, hormone refractory prostate cancer, non-small cell lung cancer, esophageal cancer, urinary bladder cancer, soft tissue sarcoma and ovarian cancer. The efficacy of DoceAqualip in this analysis is in agreement with the results of the randomized study conducted by Ahmad, et al. [8]. In this analysis, the BOR achieved was significant (p<0.0001) in 33 (58.9%) patients (CR: 7 [12.5%], PR: 26 [46.4%], p<0.0001) with different advanced solid tumors as compared to 35.5% in the study published by Ahmad, et al. [8].
Overall, in this study, DoceAqualip® was found to be well-tolerated in all advanced solid tumor types, with only 20.8% AEs of non-anaphylactic nature being Grade >3, despite the fact that DoceAqualip® was administered without any cortico steroid premedication. This safety profile is superior to that observed with conventional docetaxel [47% AEs being Grade 4] in advanced breast cancer [20]. Neutropenia with anemia (17.8%), isolated neutropenia (12.7%) and isolated anemia (4%) were the major hematologic toxicities observed with DoceAqualip®. Nausea with vomiting was the most common nonhematological toxicity observed [8]. DoceAqualip treatment did not lead to any episode of peripheral neuropathy or allergic reactions, generally seen with conventional docetaxel treatment (Grade 3 or 4 peripheral neuropathy: <10%, and allergic reactions: 25- 50% [any Grade]) [1].
Neutropenia (<2000 neutrophils/mm3) occurs in nearly all patients given 60 mg/m2 to 100 mg/m2 of docetaxel and grade 4 neutropenia (<500 cells/mm3) occurs in 85% of patients given 100 mg/m2 and 75% of patients with 60 mg/m2 [1]. Hence, primary prophylaxis with G-CSF is required to reduce neutropenia associated with conventional polysorbate 80 based docetaxel. Neutrophil count <1500 cells/mm3 require continuous G- CSF support in all subsequent cycles [1]. However, in this study, DoceAqualip® as a single agent did not require G- CSF support in various advanced solid tumor patients. Whereas, only 2 to 3 doses of G-CSF was required to normalize counts with DoceAqualip® in dual/triple combination therapy with platinum derivative, 5FU, gemcitabine, or capecitabine; only 1 patient who was on DoceAqualip® and carboplatin combination required 6 doses.
The retrospective nature of the study and a small sample size are the limitations of this study.
Conclusions
DoceAqualip® demonstrated a promising overall response in the dose range of 75-100 mg/m2 in advanced disease setting. DoceAqualip as monotherapy did not require G-CSF support. DoceAqualip® treatment is safe and well-tolerated by the patients, and obviates the need for routine corticosteroid premedication.
Acknowledgments
We would like to thank Mr. Shreekant Sharma (Lambda Therapeutic Research Ltd., Ahmedabad, Gujarat, India) for providing writing assistance and Dr. Venugopal Madhusudhana (Lambda Therapeutic Research Ltd., Ahmedabad, Gujarat, India) for additional editorial assistance for the development of this manuscript.
Conflict of Interests
Drs. Mujtaba Khan and Nisarg Joshi are employees of Intas Pharmaceuticals Ltd.
Previous Presentations
The data was presented as a poster at 2016 EUROPEAN SOCIETY FOR MEDICAL ONCOLOGY (ESMO) conference on December 16-19, 2016 at Singapore.
Funding
The manuscript development is funded by Intas Pharmaceuticals Ltd., Ahmedabad, Gujarat, India.
Authors Contributions
AM (the principal author): conceived and designed the study, collected and analyzed/interpreted data, performed data analysis and interpretation and reviewed the manuscript; SR, WZ, MS and BY: collected and analyzed/interpreted data and reviewed the manuscript. KM and JN: conceptualized the idea, reviewed the data and the manuscript. All authors met ICMJE criteria and all those who fulfilled those criteria are listed as authors. All authors had access to the study data and contributed to the development of this article. All authors read and approved the manuscript. All contributing authors approved the submission of this version of the manuscript and asserted that the document represent valid work.
Availability of Data and Materials
The datasets generated during and/or analyzed during this study are included in this published article, otherwise available from the corresponding author on reasonable request.
References
-
Taxotere Prescribing Information. Sanofi-aventis U.S. LLC, Bridgewater, NJ, Revised: 12/2015.
-
Norris LB, Qureshi ZP, Bookstaver PB, Raisch DW, Sartor O, et al. (2010) Polysorbate 80 hypersensitivity reactions: A renewed call to action. Commun Oncol 7(9): 425-428.
-
Alken S, Kelly CM (2013) Benefit risk assessment and update on the use of docetaxel in the management of breast cancer. Cancer Manag Res 5: 357-365.
-
ten Tije AJ, Verweij J, Loos WJ, Sparreboom A (2003) Pharmacological effects of formulation vehicles: implications for cancer chemotherapy. Clin Pharmacokinet 42(7): 665-685.
-
Loos WJ, Baker SD, Verweij J, Boonstra JG, Sparreboom A (2003) Clinical pharmacokinetics of unbound docetaxel: role of polysorbate 80 and serum proteins. Clin Pharmacol Ther 74(4): 364-371.
-
Zhang L, Zhang N (2013) How nanotechnology can Eastern Cooperative Oncology Group. Am J ClinOncol 5(6): 649-655.
-
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, et al. (2009) New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 45(2): 228-247.
-
U.S. Department of Health and Human Services, National Institutes of Health National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Version 4.02.
-
Naik R, Khan MA (2017) Doceaqualip in a patient with prostate cancer who had an allergic reaction to conventional docetaxel: A case report. Mol Clin Oncol 6(3): 341-343.
-
Yoo KE, Kang RY, Lee JY, Lee YJ, Suh SY et al. (2015) Awareness of the adverse effects associated with prophylactic corticosteroid use during docetaxel therapy. Support Care Cancer 23(7): 1969-1977.
-
FDA Drug Safety Communication (2014) FDA warns that cancer drug docetaxel may cause symptoms of alcohol intoxication after treatment.
-
Vyas V, Joshi N, Khan MA (2018) Novel Docetaxel Formulation (NDLS) in Low Cardiac Reserve Ovarian Cancer. J Cancer Oncol 2(2): 000122.
-
Prasanna R, Bunger D, Khan MA (2018) Efficacy and safety of DoceAqualip in a patient with locally advanced cervical cancer: A case report. Mol Clin Oncol 8(2): 296-299. enhance docetaxel therapy. Int J Nanomedicine 8: 2927-2941.
-
Ahmad A, Sheikh S, Ali SM, Ahmad M, Paithankar M et al. (2015) Development of Aqueous Based Formulation of Docetaxel: Safety and Pharmacokinetics in Patients with Advanced Solid Tumors. J Nanomed Nanotechnol 6: 295.
-
Ahmad A, Sheikh S, Taran R, Srivastav SP, Prasad K, et al. (2014) Therapeutic efficacy of a novel nanosomal docetaxel lipid suspension compared with taxotere in locally advanced or metastatic breast cancer patients. Clin Breast Cancer 14(3): 177-181.
-
McKeage K (2017) Nanosomal Docetaxel Lipid Suspension: A Guide to Its Use in Cancer. Clin Drug Investig 37(4): 405-410.
-
Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, et al. (1982) Toxicity and response criteria of the
-
Rajappa S, Joshi A, Doval DC, Batra U, Rajendranath R, et al. (2018) [Experts' Opinion] Novel formulations of docetaxel, paclitaxel and doxorubicin in the management of metastatic breast cancer. Oncol Lett 16(3): 3757-3769.
-
Bergh J, Bondarenko IM, Lichinitser MR, Liljegren A, Greil R, et al. [2012] First-line treatment of advanced breast cancer with sunitinib in combination with docetaxel versus docetaxel alone: results of a prospective, randomized phase III study. J Clin Oncol 30(9):921-929.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma