Real World Evidence: Treatment of Patients with Non- Metastatic Colon Cancer in a Community Hospital in Argentina: A Retrospective Cohort Study
Background: The addition of adjuvant chemotherapy (ACT) to the surgical treatment of locally advanced colon cancer (CC) was shown to reduce relapses in stage III disease, although it remains controversial in stage II. However, an underutilization of ACT in stage III patients was reported. Data on use of ACT in stage II and in older patients in the “real world†in developing countries are limited. We aimed to describe management and outcome of non-metastatic colon cancer patients in a community hospital in Argentina. Methods: We retrospectively reviewed clinical charts of 99 patients with non-metastatic CC admitted in our Department between 2007 and 2016 extracting data on surgical treatment and chemotherapy use. Results: Emergency surgery was performed in 36.2% of cases. Near 72% of patients had 12 or more lymph nodes examined. Adjuvant chemotherapy was delivered to 93.1% of patients with stage III, to 38.1% of patients with stage II disease, and to 94.1% of stage III patients older than 70 years. Ninety six percent of patients with stage III disease received oxaliplatin-based chemotherapy. Similar proportions (near 50%) of patients <70 and > 70 years completed chemotherapy. After the median follow up of 2.1 years, (Interquartile range, 1.4 to 4.4 years), 16.2% of patients had a relapse. Conclusion: A guideline-compliant lymphadenectomy and ACT were performed in the majority of patients with CC in the routine practice in a developing country. The proportion of emergency surgical interventions is high. High proportion of older patients received ACT, and its completion rate in this subgroup is similar to younger patients.
Background
Colorectal cancer (CRC) is the third most common neoplasia and the fourth most common cause of cancer mortality worldwide [1]. Although the disease is more frequent in high-income countries, in the last decades the incidence of CRC also increased in developing countries, including Latin America. In Argentina, CRC is the second most frequent malignancy and the second cause of cancer related deaths [2, 3]. Near 82% of all CRC occurs in non- rectal subsites. About 20 % of them are non-metastatic at initial diagnosis [4]. Although surgery is the mainstay of the treatment of localized and locally advanced colon cancer (CC), the addition of adjuvant chemotherapy (ACT) reduces the risk of relapse. While for patients with stage III disease ACT is the standard of care, its benefit in stage II is a matter of debate and in this group ACT might be reserved for those patients with features of high risk of recurrence or even only for those with T4 [5, 6, 7]. However, data on the proportion of patients with stage II, treated with adjuvant chemotherapy in daily practice are scarce and disparate [5].
Recently, Grothey, et al. published a pooled analysis of six adjuvant randomized clinical trials (RCT), which found non-inferiority of three months of capecitabine plus oxaliplatin treatment compared with the six months in the general stage III population, challenging the established knowledge about the optimal duration of the ACT [8].
However, even in high-income countries, population- based studies reported underutilization of adjuvant chemotherapy in the routine practice due either to the failure to initiate or to insufficient rates of completion of guidelines-recommended adjuvant chemotherapy in stage III, particularly among the elderly, in patients with comorbidities and in those living in low-income neighborhoods [9, 10, 11]. In stage II, significant between- country differences in the interpretation of the risk of relapse and the perception of the need for ACT were reported in Europe [5].
Some aspects of safety and efficacy of adjuvant chemotherapy in the elderly population are less well- depicted, as these patients were underrepresented in randomized trials. Although analyses of large population- based datasets showed a benefit of ACT in older patients with stage III, the use of oxaliplatin in this subgroup is controversial [12, 13, 14]. Greater age was associated with inferior cancer specific and overall survival [15].
To our knowledge, in Latin America, in the absence of large region or nation-wide registries, data on treatment of non-metastatic colorectal cancer are scarce and limited to a handful of retrospective cohorts [16, 17]. Classical RCTs show results from a narrow patient group with an “artificial” care. Patients with “real-life” co-morbidities and lifestyle factors receiving usual care often have different responses to medication which will not be captured by RCTs if they are excluded by strict selection criteria. Evidence from real-world studies, including observational retrospective studies, can be combined with RCT evidence to provide a fuller picture of intervention effectiveness. Also, it can allow uncover potential hurdles in the implementation of the best evidence-based practice, helpful for optimizing the care at population level [18].
We aimed to describe the characteristics of patients with non-metastatic CC, the degree of compliance with guidelines- recommended standards of surgical and medical care and their results in a community hospital in Argentina, in the general population and in the subgroup of patients more than 70 years old.
Methods
We retrospectively analyzed non-electronic clinical records of patients with histopathologically confirmed diagnosis of non-metastatic colon cancer admitted in the Department of Oncology of Juan A Fernandez Hospital between January of 2007 and December of 2016. CC was defined as any primary malignant tumor of colon. The tumor stage was determined following the American Joint Committee on Cancer pathological TNM staging system, seventh edition [19].
We included patients with stages I to III CC, who underwent surgical treatment of their disease with a curative intention, as their first treatment, and had more than one visit in the Department of Oncology. We decided to exclude patients who had only one consultation due to the impossibility to know for sure, if those patients continued their treatment in another hospital, were unable to be treated, or have declined treatment. Other exclusion criteria were diagnosis of lymphoid or neuroendocrine neoplasms of colon.
Patients with a second primary tumor, either colonic or extra-colonic were included. Aside from demographic and tumor-related characteristics, we extracted data on type of surgery, number of lymph nodes removed, adjuvant chemotherapy regimen used, number of cycles completed, length of the follow-up, and disease status at the end of the follow-up period. Due to the high proportion of patients either lost to follow-up or with a short follow-up length, analyses of the overall survival were judged to be biased and thus not performed.
We treated variables such as type of surgery (urgent versus scheduled), histologic grade (well-differentiated versus moderate and poor differentiated), type of adjuvant chemotherapy (oxaliplatin plus fluoropirimidines versus fluoroprimidines alone), completeness of chemotherapy, and proportion of patients with relapse at the end of follow-up as dichotomous. If regimens of chemotherapy with the duration different from 21 day were used, the number of cycles was normalized to a 21-days schedule. We assumed that the adjuvant chemotherapy program was complete, if six to eight cycles of the 21 day cycle were completed, similar to the definition of the completeness used by Dobie, et al. [11].
Tumors localized at splenic flexure or below were classified as left-sided, otherwise, as right sided. Planned subgroup analyses were performed by age, with the 70-year cut off point, and tumor stage (II versus III).
Disease-free survival (DFS) was defined as the time from admission to relapse or death from any cause. To estimate DFS Kaplan-Meier analysis was used.
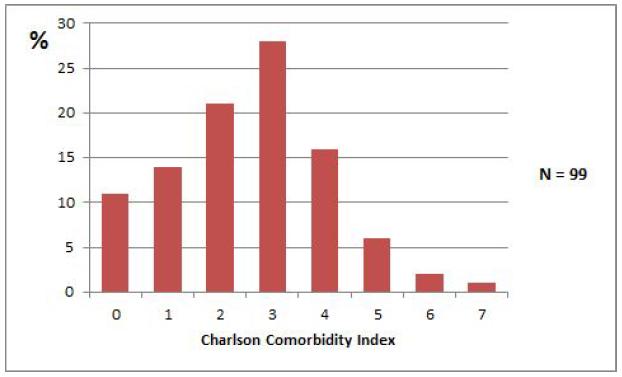
The severity of comorbid states was assessed with Charlson Comorbidity Index (CCI) [20].
To explore the associations between the probability of relapse and tumor sidedness, histologic grade, type of surgery (planned versus urgent), completeness of the lymphadenectomy and completeness of ACT a multivariate analysis using Fisher’s exact test was performed.
Subgroups of younger and older patients were compared using chi-square test. Alpha level was set at 0.05. For simple statistics Microsoft Excel 2010 was used. Subgroup analysis was carried out using Stata version 12.0 (StataCorp LP, Texas, USA).
Study protocol was approved by institutional board on medical ethics.
Results
After the exclusion of 10 patients 99 were eligible for analysis. Table 1 shows the clinical features of included patients. Fifty-eight percent of patients were males. The mean age was 65.0 years (95% CI, 61.3–68.7). Twenty seven percent of patients were current or former smokers. Arterial hypertension, observed in more than 30%, was the most common comorbidity. The presence of a synchronic or meta-chronic second primary tumor was noted in 12.1% of patients. A more detailed description of comorbidities and second primaries is shown in Tables 2 and 3, and Figure 1.
| 45 (46.4%) | 24 (39.3%) | 21 (58.3%) | ||
| Right | 52 (53.6%) | 37(60.7%) | 15 (41.5%) | |
| Left | ||||
| Tumor stage | ||||
| II | 42 (42.4%) | 25 (59.5%) | 17(40.5%) | 0.82 |
| III | 44 (44.4%) | 27(44.3%) | 17 (44.7%) | |
| Histologic gradeb | 0.36 | |||
| Well differentiated | 14 (15.4%) | 7(13.0%) | 7 (18.9%) | |
| Moderately differentiated | 68 (74.7%) | 41(75.9%) | 27 (73.0%) | |
| Poorly differentiated | 9 (9.9%) | 6 (11.1%) | 3 (8.1%) | |
| Type of surgeryc | 0.57 | |||
| Emergency | 34 (36.2%) | 23 (37.7%) | 11 (33.3%) | |
| Scheduled | 60 (63.8%) | 38 (62.3%) | 22 (66.7%) | |
| Lymph nodes numberd | ||||
| Examined, meanmean (CI 95%) | 20 (17.6-20.3) | 21 (IC 95%17.7-24.3) | 17 (IC 95%13.6-19.6) | |
| >= 12 | 71 (73.2%) | 47 (78.3%) | 24(64.9%) | |
| < 12 | 26 (26.8%) | 13 (21.7%) | 13(35.1%) | 0.15 |
| Positive lymph nodes, mean (CI 95%) | 2 (1.3-2.7) | 2 (1.1-2.9) | 2 (0.85-3.15) | |
| Adjuvant chemotherapy delivered, stage III | 41 (93.1%) | 26 (96.2%) | 16 (94.1%) | 0.73 |
| Type of chemotherapy, stage III | ||||
| FP + Oxaliplatine | 36 (85.7%) | 25 (96.1%) | 11 (68.8%) | 0.01 |
| FP alone | 6 (14.3%) | 1 (3.9%) | 5 (31.2%) | |
| Adjuvant chemotherapy completed, stages II and III | 50 (50.9%) | 18(50%) | 11 (50%) | 0.66 |
Table 1: Comorbidities in patients with non-metastatic colon cancer.
Abbreviations: *ECOG PS – Eastern Cooperative Oncology Group Performance Status; **FP – Fluoropirimidines a) Not available for two patients. b) Not available for eight patients. c) Not available for five patients. d) Not available for two patients.
| Condition | Number of patients (%) | |
|---|---|---|
| Rectum | Arterial Hypertension | 30 (30.3%) |
| Colon | Heart Disease* | 12 (12.1%) |
| Stomach | Diabetes Mellitus | 9 (9.1%) |
| Prostate | COPD/Asthma | 6 (6.1%) |
| Breast | Rheumatoid Arthritis | 2 (2.0%) |
| Kidney | Hypothyroidism | 2 (2.0%) |
| Maxillary sinus | Stroke | 1 (1.0%) |
| Endometrium | Aorta Aneurysm | 1 (1.0%) |
| Melanoma | Others | 5 (5.1%) |
| Skin non-melanoma |
Table 2: Clinicopathological features of included patients and their treatment.
| Anatomic site | Number |
|---|---|
| Rectum | 3 |
| Colon | 1 |
| Stomach | 1 |
| Prostate | 1 |
| Breast | 1 |
| Kidney | 1 |
| Maxillary sinus | 1 |
| Endometrium | 1 |
Table 3: Data on second primary tumors in patients with non-metastatic colon cancer.
Tumors were left-sided in 53.6% of patients and right- sided in 46.4%. Adenocarcinoma histology was observed in 99.0% (16.2% mucinous) and undifferentiated carcinomas in 1% of tumors. Data on carcinoembryonic antigen (CEA) value before surgery was available in 60 out of 99 (60.6%) of patients. Median of the baseline CEA was 2.2 UI/ml, (interquartile range (IQR), 1.2-5.4)) Forty four percent of patients had stage III, 42.2% had stage II and 13.2% stage I disease. All the patients underwent curative resection as their first treatment. Scheduled surgery was performed in 63.8% of patients, while emergency procedure in 36.2%. The mean number of lymph nodes removed was 19.6 (95% CI: 17.3 – 22). Near 72% of patients had 12 or more lymph nodes examined. Among stage II patients, 10 out of 42 (23.8%) had T4. The prevalence of other poor prognostic factors, potentially influencing the indication of the adjuvant chemotherapy is shown in Table 4.
| Risk factor | Number of patients (% | ) | |||
|---|---|---|---|---|---|
| T4 | 10/42 (23.8%) | ||||
| Less than 12 lymph nodes examined | 12/42 (28.6%) | ||||
| Poor differentiated histology | 5/42 (11.9%) | ||||
| Elevated baseline CEA | 10/42 (23.8%) | ||||
| Emergency surgery* | 17/42 (40.5%) |
Table 4: Prevalence of poor risk prognostic factors among stage II patients.
Data on chemotherapy was available in 98 out of 99 (99%) of patients. Globally, adjuvant chemotherapy was delivered to 58.2% of patients. Of them, 50.9% completed adjuvant chemotherapy. Seventy nine percent were treated with the combination of oxaliplaitin and a fluoropirimidine, 21.0% with a fluoropirimidine alone. The proportion of patients, who received adjuvant chemotherapy were 93.1% in the stage III and 38.1% in the stage II. There was no treatment related death.
In the subgroup of aged patients, emergency surgery was performed in 37.3%. In this subgroup adjuvant chemotherapy was carried out in 94.1% of patients with stage III disease and 35.2% with stage II whereas in younger patients in 56.8% and 24.4% respectively. Fifty percent of them finished a complete program. Toxicity was the main cause of the desertion.
A comparison between subgroups of patients older and younger of 70 years is shown in Table 1. A similar distribution of variables like initial state, and histological grade was noted. The proportion of right-sided tumors was greater among older patients, 58.3 vs 39.3%. More frequent use of emergency surgery in the older subgroup (37.7 % versus 33.3 %, p= 0.04) was observed. The proportions of patients, who received adjuvant chemotherapy in stage III in patients <70 and > 70 years old were 96.2 % and 94.1 % respectively (p =0.82). Fifty percent of patients in both subgroups completed ACT. In the subgroup of the older patients 31.2% were treated with fluoropirimidine monotherapy while in the younger subgroup 3.9 %. Age > 70 years was negatively associated with the oxaliplatin use, (Chi square test, p=0.01). No statistically significant association between CCI and ACT indication and ACT completeness was observed (not shown, available on demand).
Median follow-up time was 2.1 years, (IQR, 1.4 to 4.4). Thirty-one percent of patients were lost to follow-up. At the end of the follow-up period recurrence took place in 16.2% of patients. Median time to relapse was 1.1 years (IQR, 0.95 to 2.25). In the multivariate analysis only moderate/poor histologic grade (Fisher´s exact test, p = 0.04) and emergency surgery (Fisher´s exact test, p= 0.02) had a statistically significant association with an increased probability of relapse.
Discussion
The study describes the management and outcomes of patients with resectable colon cancer in a community hospital in Argentina. An adequate lymphadenectomy, with 12 or more lymph nodes retrieved, was achieved in 72% of patients, which is not inferior to figures reported in randomized control trials and observational studies from Europe [21, 22].
Although 95% of patients with stage III disease, eligible for analysis, had started adjuvant chemotherapy, only near a half of them completed the program. Reasonably, the proportion of patients with stage III treated with adjuvant chemotherapy appears as too high, when compared with that reported in retrospective population-based studies from US and Canada, which found that only 55% to 63% of patients with stage III received it [9, 11]. This can be explained by the hospital- based nature of our data, but probably only partly. For instance, a hospital-based observational study from Chile reported that near 70% of patients with stage III disease received adjuvant chemotherapy [16].
A high proportion of T4 and emergency surgical interventions observed in our study likely reflect the failure to timely detect asymptomatic and/or properly diagnose early symptomatic tumors. A high proportion of stage III patients (86%) were treated with oxaliplatin- based chemotherapy. Even among older patients the oxaliplatin-based therapy were used more frequently than fluoropirimidines alone. Kaplan-Meier estimate of the disease-free survival is shown in Figure 2.
The rate of completion of chemotherapy in our study was lower than in the study by Dobie et al. which found that 78% of Medicare patients completed adjuvant chemotherapy. However, this study is referred to a period of time previous to the oxaliplatin use, which potentially can account for the difference [11].
The proportion of the stage II patients who received adjuvant chemotherapy was as high as 38%, significantly superior to European population based study, which had been reported rates between 9% (Netherlands) and 24% (Belgium). In two hospital-based studies from Chile, adjuvant chemotherapy was delivered to 20% and 22% of stage II patients respectively [16, 17]. The difference can be attributed, at least partially, to the high prevalence of adverse prognostic factors, especially T4, among stage II patients in our study, (Table 4). For comparison, in the Chilean study by Mondaco, et al. the proportion of patients with T4 was only 13% [16].
![Figure 2: The rate of completion of chemotherapy in our study was lower than in the study by Dobie et al. which found that 78% of Medicare patients completed adjuvant chemotherapy. However, this study is referred to a period of time previous to the oxaliplatin use, which potentially can account for the difference [11].](/fulltextimages/2970/fig_2.png)
Due to the short median follow-up time and high percentage of the patients lost to follow-up (31%) we considered the data on relapse rate too biased to be compared with other studies without the comparison may being misleading.
When subgroups of patients younger and older than 70 years were compared, the proportion of patients with stage III disease delivered chemotherapy and the rate of completion of chemotherapy was similar.
The lack of association with established prognostic factors, like number of lymph nodes involved and sideness with disease-free survival is likely due to the design of our study which is not an appropriate for prognostic factor assessment and these result are need to be interpreted with extreme caution.
The main limitations of the study are its retrospective nature, the high rate of loss to follow-up, and the small number of participants, which make it prone to some biases, especially chance, selection bias and confounding. However, in the absence of published large population- based retrospective or hospital-based prospective data in Argentina, it allows a useful insight into the patterns of care of the non-metastatic CC in the”real world”.
Conclusions
A guideline- compliant lymphadenectomy and ACT were accomplished in the majority of patients with colon cancer in the routine practice in a developing country. The proportion of emergency surgical interventions is high. A high proportion of older patients received ACT and its completion rate in this subgroup is similar to younger patients. The use of oxaliplatin-based chemotherapy in older patients may be excessive. Acknowledgements: We would like to acknowledge to our families for their tolerance. We would like to acknowledge to Laura Svidler Lopez, MD, Department of Surgery, Juan A Fernandez Hospital for her assistance in some surgical issues. Conflict of Interest Statement: None to declare
References
-
Cancer Today. Population fact sheets: World.
-
Sierra MS, Forman D (2016) Burden of colorectal cancer in Central and South America. Cancer epidemiology 44(1): S74-S81.
-
Presidencia de la Nación. Ministerio de Salud. Instituto Nacional de Cáncer. Cancer colorectal. Argentina 2018.
-
Cheng X, Chen VW, Steele B, Ruiz B, Fulton J, et al. (2001) Subsite-specific incidence rate and stage of disease in colorectal cancer by race, gender, and age group in the United States, 1992–1997. Cancer 92(10): 2547-2554.
-
Babaei M, Balavarca Y, Jansen L, Lemmens V, van Erning FN, et al. (2018) Administration of adjuvant chemotherapy for stage II-III colon cancer patients: An European population-based study. International Int J Cancer 142(7): 1480-1489.
-
Salem ME, Yin J, Goldberg RM, Pederson L, Wolmark N, et al. (2018) Outcomes over time (1998-2009) of stage II colon cancer patients (pts) receiving adjuvant FOLFOX: Pooled analysis of 1,122 pts in the ACCENT database. J Clin Oncol 36(4): 728-728.
-
Network NCC (2017) NCCN Guidelines Version
-
2017 Giant Cell Tumor of Bone.
-
Grothey A, Sobrero AF, Shields AF, Yoshino T, Paul J, et al. (2018) Duration of adjuvant chemotherapy for stage III colon cancer. N Engl J Med 378(13): 1177- 1188.
-
Winget M, Hossain S, Yasui Y, Scarfe A (2010) Characteristics of patients with stage III colon adenocarcinoma who fail to receive guideline- recommended treatment. Cancer 116(20): 4849- 4856.
-
Hines RB, Bimali M, Johnson AM, Bayakly AR, Collins TC (2016) Prevalence and survival benefit of adjuvant chemotherapy in stage III colon cancer patients: Comparison of overall and age-stratified results by multivariable modeling and propensity score methodology in a population-based cohort. Cancer epidemiology 44: 77-83.
-
Dobie SA, Baldwin LM, Dominitz JA, Matthews B, Billingsley K, et al. (2006) Completion of therapy by Medicare patients with stage III colon cancer. J Nat Cancer Inst 98(9): 610-619.
-
Yothers G, O'Connell MJ, Allegra CJ, Kuebler JP, Colangelo LH, et al. (2011) Oxaliplatin as adjuvant therapy for colon cancer: updated results of NSABP C- 07 trial, including survival and subset analyses. J Clin Oncol 29(28): 3768-3774.
-
Mack CDF, Brookhart MA, Glynn RJ, Meyer AM, Carpenter WR, et al. (2015) Comparative Effectiveness of Oxaliplatin vs. 5-flourouricil in Older Adults: An Instrumental Variable Analysis. Epidemiology 26(5): 690-699.
-
National Cancer Comprehensive Network. NCCN Guidelines Version 3.2018. Colon Cancer.
-
Booth CM, Nanji S, Wei X, Peng Y, Biagi JJ, et al. (2016) Use and effectiveness of adjuvant chemotherapy for stage III colon cancer: a population-based study. J Natl Compr Canc Netw 14(1): 47-56.
-
Mondaca S, Villalón C, Leal JL, Zúñiga A, Bellolio F, et al. (2016) Beneficio de la quimioterapia adyuvante en pacientes con cáncer de colon: cohorte retrospectiva de un hospital clinic universitario. Rev Chil Cir 144(2): 145-151.
-
Bannura G, del castillo C, Barrera A, Soto CD, Contreras PJ, et al. (2008) Resultados de la quimioterapia adyuvante en cáncer de colon. Rev Chil Cir 60(5): 403-409.
-
Roche N, Reddel HK, Agusti A, Bateman ED, Krishnan JA, et al. (2013) Integrating real-life studies in the global therapeutic research framework. The Lancet Respiratory Medicine 1(10): e29-e30.
-
American Joint Comettee on Cancer. Colon and Rectum Cancer Staging. 7th edition.
-
André T, Boni C, Mounedji-Boudiaf L, Navarro M, Tabernero J, et al. (2004) Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med 350(23): 2343-2351.
-
Betge J, Harbaum L, Pollheimer MJ, Lindtner RA, Kornprat P, et al. (2017) Lymph node retrieval in colorectal cancer: determining factors and prognostic significance. Int J Colorectal Dis 32(7): 991-998.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma