Clinicopathological Association of DNA Repair Gene Polymorphisms in Colorectal Cancer Patients
Several polymorphisms in DNA repair genes, especially ERCC1 C118T, ERCC2 Lys751Gln and XRCC1 Arg399Gln have been found to affect treatment efficacy and prognosis in patients with colorectal cancer (CRC). However, scarce reports available on the association of these polymorphisms with clinicopathological parameters. As clinicopathological factors provide important information to determine prognosis in CRC, present study evaluated association of DNA repair gene polymorphisms with clinicopathological parameters. ERCC1 C118T, ERCC2 Lys751Gln and XRCC1 Arg399Gln polymorphisms were studied by PCRRFLP in 143 primary CRC patients. For ERCC1 C118T polymorphism, predominance of heterozygous C/T (56%) was noted compared to wild type C/C (29%) and variant T/T (15%) genotypes. ERCC2 Lys751Gln polymorphism showed 44% of wild type A/A, 40% of heterozygous A/C, and 16% of variant C/C genotypes. XRCC1 Arg399Gln polymorphism displayed wild type G/G (48%), heterozygous G/A (42%), and variant A/A (10%). In relation to clinicopathological parameters, ERCC1 C118T polymorphism was significantly associated with tumor site (P=0.021); tumor location (P=0.039); and tumor differentiation (P=0.041). Moreover, a significant correlation of ERCC2 Lys751Gln polymorphism was noted with lymphocytic stromal response (P=0.026) and necrosis (P=0.041). However, XRCC1 Arg399Gln polymorphism was not significantly associated with clinicopathological factors. Further, a significant positive correlation was observed between ERCC2 and XRCC1 polymorphism (P=0.002). To conclude, higher frequency of ERCC1 118 variant C/T and T/T genotypes was noted in patients with colon cancer and right side located tumors. Variant C allele of ERCC2 751 polymorphism was associated with less aggressive colorectal tumors. Moreover, significant association between ERCC2 and XRCC1 polymorphisms proposes interlink of genes of different DNA repair pathways in CRC.
Introduction
Colorectal cancer (CRC) is a major health burden with approximately 1.8 million incident cases each year worldwide [1]. Clinical outcome of CRC has been improved effectively with the use of novel chemotherapeutic drugs.
Currently, platinum agent- oxaliplatin in combination with 5-Flourouracil (5-FU) has been used as a standard first-line treatment in metastatic CRC and it has significantly improved overall survival (OS) in the adjuvant treatment of stage II/III CRC patients with a response rate of over 40% [2]. However, the hindrance for the effective oxaliplatin-based treatment is tumor cell drug resistance in which DNA- repair plays a crucial role [3].
DNA repair has an essential function in maintaining genome integrity and preventing carcinogenesis. Defects in DNA repair pathways such as nucleotide excision repair (NER) and base excision repair (BER) may result in accumulation of DNA damage, carcinogenesis, and may reduce chemotherapeutic sensitivity [4]. Evidence suggests that single nucleotide polymorphisms (SNPs) in DNA repair genes could alter DNA repair function, modulate its capacity, and thus induce genetic instability and subsequently tumor formation and progression [5, 6]. These SNPs especially in DNA repair genes- ERCC1, ERCC2 and XRCC1 are known to affect cancer susceptibility, prognosis, and therapeutic outcomes [2, 3, 7, 8, 9]. The ERCC1 and ERCC2 proteins are highly conserved rate-limiting enzymes in the NER pathway. They participate in the key steps of NER such as the damage recognition and removal of DNA lesions induced by substances such as platinum [2]. Several common and putatively functional SNPs of ERCC1 and ERCC2 have been identified, of which ERCC1 rs11615 SNP (C118T) has some effects on ERCC1 mRNA expression, whereas ERCC2 rs13181 SNP (Lys751Gln, [T>G]) is associated with suboptimal DNA repair capacity [10]. On the other hand, the DNA repair gene XRCC1 is known to play a critical role in BER pathway. It acts as a scaffold protein in BER of oxidative DNA and single- strand break (SSB) repair [11, 12]. It corrects damage to bases and SSBs in DNA induced by ionizing radiation and alkylating agents [13]. The most extensively investigated XRCC1 Arg399Gln polymorphism on exon 10 leads to G→A amino acid substitution (Arg399Gln) may alter BER activity causing the alteration of the phenotype of XRCC1 protein resulting in deficient DNA repair capacity [14].
Many studies showed role of ERCC1, ERCC2 and XRCC1 polymorphisms as prognostic and predictive markers in CRC [15, 16, 17, 18, 19, 20]. Fundamentally, it has been described that prognosis and appropriate management in CRC is strongly related to individual patient characteristics. Additionally, the anatomical extent of the disease, as assessed by clinicopathological staging, provide essential information regarding likely prognosis to guide management [21]. Thus, studying correlation of DNA repair gene polymorphisms with clinicopathological parameters might aid in determining prognosis in CRC. However, rare studies described association of these polymorphisms with clinicopathological factors in patients with CRC. Hence, we aimed to study the correlation of various clinicopathological variables such as age, gender, tumor location, stage, tumor differentiation, nodal status, etc. with DNA repair gene polymorphisms- ERCC1 C118T, ERCC2 Lys751Gln and XRCC1 Arg399Gln in CRC patients.
Materials & Methods
Patients
Present study enrolled a total of 143 untreated colorectal cancer patients at ‘The Gujarat Cancer & Research Institute’, Ahmedabad between 2007 and 2014. The study was approved by Institutional Scientific and Ethical Review committees. The detailed clinicopathological findings were noted from the case files maintained at the Medical Record Department of the institute. Based on TNM classification with World Health Organization (WHO) Grading System, pathologic staging of the CRC patients was performed. All patients were primarily treated with surgery or surgery followed by adjuvant chemotherapy and/or radiotherapy. Out of 143, 113 patients were treated with chemotherapeutic regimen. The main chemotherapeutic treatment included were 5-FU and leucovorin (LV), oral capecitabine, or in combination with Oxaliplatin (OX). The patient and tumor characteristics are shown in Table 2.
Sample Collection
Written consent of the patients who underwent surgery at the Department of Surgical Oncology was obtained prior to primary tumor tissue collection. Primary tumor tissue samples were collected on ice directly from the operation theatre for the detection of ERCC1, ERCC2 and XRCC1 polymorphisms. Pathologist selected tumor tissues and divided into two portions. One portion was submitted for the routine histopathological evaluation and the other portion was immediately snap frozen in liquid nitrogen and preserved at -80°C till DNA extraction.
Polymorphism Study of DNA Repair Enzymes by PCR-RFLP
DNA was extracted from the frozen tumor tissues by phenol-chloroform extraction method. For polymorphism study, polymerase chain reaction (PCR) analysis was performed in a ProFlex PCR system (Applied Biosystems, Life Technologies) using PCR core kit (Qiagen, USA) as per manufacturer protocol. The annealing temperatures used were 55.7°C for ERCC1, 60°C for ERCC2, 54°C for XRCC1. Primers used were as follows: ERCC1 C118T (Forward: 5’ GCA GAG CTC ACC TGA GGA AC 3’ Reverse: 5’ GAG GTG CAA GAA GAG GTG GA 3’) ERCC2 Lys751Gln (Forward: 5’ GCA GAG CTC ACC TGA GGA AC 3’ Reverse: 5’ GAG GTG CAA GAA GAG GTG GA 3’) and XRCC1 Arg399Gln (Forward: 5’ TTG TGC TTT CTC TGT GTC CA 3’ Reverse: 5’ TCC TCC AGC CTT TTC TGA TA
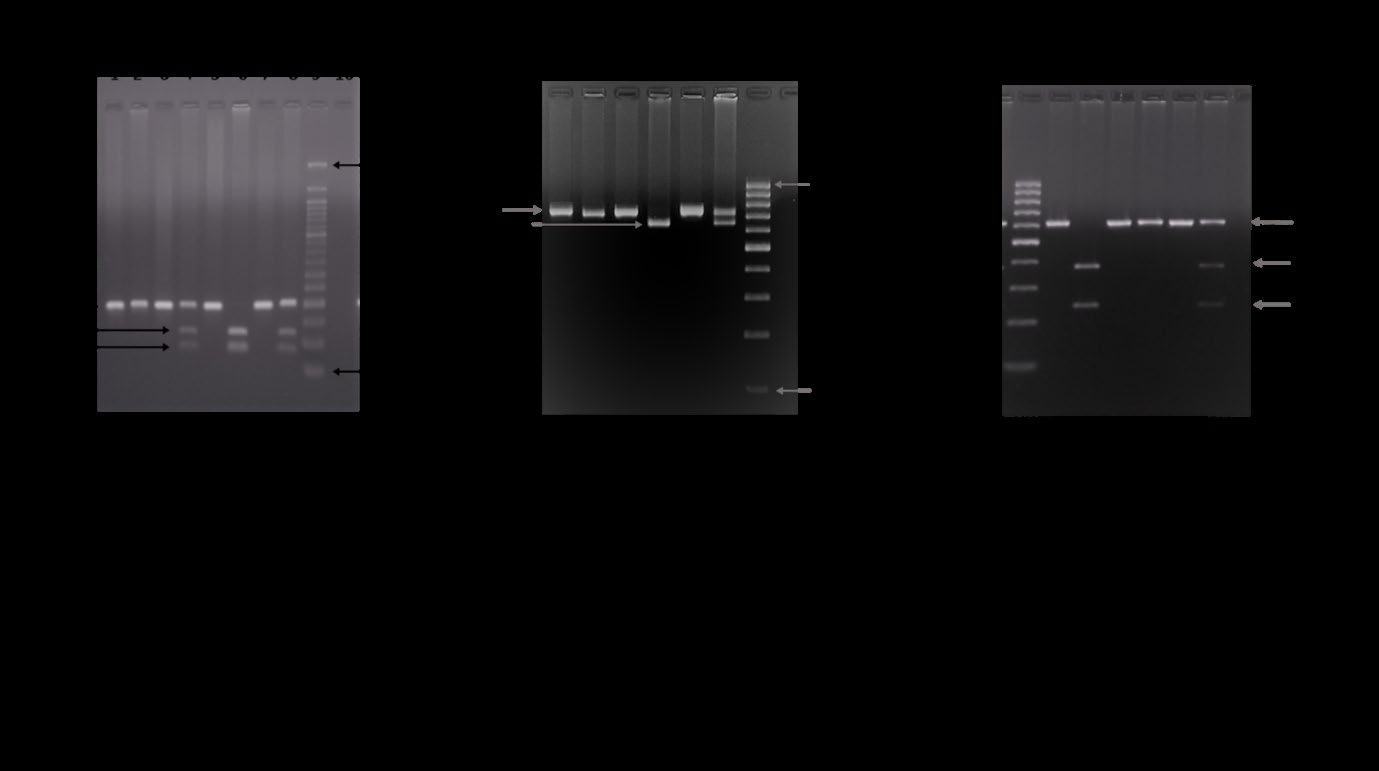
3’). PCR products were then digested with specific restriction enzymes (ERCC1- BsrDI at 65°C for 4 hrs, ERCC2-PstI at 37°C overnight, XRCC1-MspI at 37°C overnight). The digested products were separated on 2.5% ethidium bromide-stained agarose gel. Then, the genotypes of the DNA samples were examined for each polymorphism by visualizing the gel on UV transilluminator and image was captured on Gel documentation system (Alpha Innotech, USA).
Statistical Analysis
The data was statistically analyzed using the Statistical Package for Social Sciences (SPSS) software version 17 (SPSS Inc., USA). The distribution of genotypes in patients was first tested for the Hardy-Weinberg equilibrium (HWE) by a goodness-of-fit Chi-square (χ2) test to compare the observed genotype frequencies to the expected ones. Two-tailed Chi- square test was used to assess the associations between gene polymorphisms and clinicopathological parameters. Correlation between two parameters was calculated using Spearman’s correlation coefficient (r) method. P value ≤0.05 was considered to be significant.
Results
Incidence of ERCC1 C118T, ERCC2 Lys751Gln and XRCC1 Arg399Gln Polymorphisms in CRC Patients
The genotype frequencies observed for ERCC1 C118T, ERCC2 Lys751Gln and XRCC1 Arg399Gln polymorphisms are depicted in Table 1 [22]. Distribution of these polymorphisms in the studied CRC patients followed HWE (Table 1). The Representative gel images are shown in Figure 1.
| Genotypes | SNPs | ||
|---|---|---|---|
| ERCC1 C118T | ERCC2 Lys751Gln | XRCC1 Arg399Gln | |
| Homozygous wild type N (%) | C/C 42 (29) | A/A 63 (44) | G/G 68 (48) |
| Heterozygous variant N (%) | C/T 80 (56) | A/C 57 (40) | G/A 60 (42) |
| Homozygous variant N (%) | T/T 21 (15) | C/C 23 (16) | A/A 15 (10) |
| Combined variant N (%) | C/T+T/T 101 (71) | A/C+C/C 80 (56) | G/A+A/A 75 (52) |
| HWE | χ2=2.946 | χ2=2.611 | χ2=0.105 |
| P=0.086 | P=0.106 | P=0.744 |
Correlation of DNA Repair Gene Polymorphisms with Clinicopathological Parameters
For clinicopathological association, all three polymorphisms in DNA repair genes were grouped into wild type and combined variant type. Table 2 summarizes the correlation of these polymorphisms with clinicopathological parameters. When ERCC1 C118T polymorphism was correlated with clinicopathological parameters, it showed significant correlation with tumor site, tumor location and tumor differentiation. The incidence of combined variant genotypes (C/T+T/T) was significantly higher in colon cancer patients (80%) as compared to rectal cancer patients (62%, P=0.021); in patients having right side tumors (82%) as compared to those having left side tumors (65%, P=0.039); and in patients with moderately/poorly differentiated tumors (75%) as compared to those with well differentiated tumors (55%, P=0.041). On the other side, ERCC2 Lys751Gln polymorphism showed significant inverse correlation with lymphocytic stromal response and necrosis. The incidence of ERCC2 variant genotypes (A/C+C/C) was significantly higher in patients having absence of lymphocytic stromal response (60%, P=0.026) and absence of necrosis (59%, P=0.041) as compared their respective counterparts. However, the rest of the parameters such as age, gender, diet, family history, tumor size, nodal status, tumor stage, histopathologic type, lymphatic permeation, vascular permeation and perineural invasion did not show any significant association with ERCC1 and ERCC2 gene polymorphisms. Moreover, in relation to XRCC1 Arg399Gln polymorphism, no significant correlation with any of the parameters was noted. Only of a trend of higher incidence of XRCC1 variant genotypes (G/A+A/A) was observed in patients with pre-op circulating CEA levels ≥ 5.0 ng/ml (59%) as compared to those with pre-op CEA levels < 5.0 ng/ml (44%, P=0.096) (Table 2).
| Clinico pathological Characteristics | N | ERCC1 C118T polymorphism | ERCC2 Lys751Gln polymorphism | XRCC1 Arg399Gln polymorphism | |||
|---|---|---|---|---|---|---|---|
| Wild type C/C N (%) | Variant type C/T+T/T N (%) | Wild type A/A N (%) | Variant type A/C+C/C N (%) | Wild type G/G N (%) | Variant type G/A+A/A N (%) | ||
| Age (years) | |||||||
| <52 years | 68 | 16 (24) | 52 (76) | 30 (44) | 38 (56) | 33 (48) | 35 (52) |
| ≥ 52 years | 75 | 26 (35) | 49 (65) | 33 (44) | 42 (56) | 35 (47) | 40 (53) |
| χ2=2.133, r=-0.122, P=0.146 | χ2=0.000, r=+0.001, P=0.989 | χ2=0.050, r=+0.019, P=0.825 | |||||
| Gender | |||||||
| Female | 58 | 18 (31) | 40 (69) | 28 (48) | 30 (52) | 27 (47) | 31 (53) |
| Male | 85 | 24 (28) | 61 (72) | 35 (41) | 50 (59) | 41 (48) | 44 (52) |
| χ2=0.130, r=+0.030, P=0.721 | χ2=0.705, r=+0.070, P=0.405 | χ2=0.039, r=- 0.017, P=0.844 | |||||
| Habit* | |||||||
| No | 77 | 24 (31) | 53 (69) | 33 (43) | 44 (57) | 39 (51) | 38 (49) |
| Yes | 66 | 18 (27) | 48 (73) | 30 (45) | 36 (55) | 29 (44) | 37 (56) |
| χ2=0.260, r=+0.043, P=0.613 | χ2=0.097, r=-0.026, P=0.757 | χ2=0.642, r=+0.067, P=0.427 | |||||
| Family History | |||||||
| No | 133 | 38 (29) | 95 (71) | 57 (43) | 76 (57) | 62 (47) | 71 (53) |
| Yes | 10 | 04 (40) | 06 (60) | 06 (60) | 04 (40) | 06 (60) | 04 (40) |
| χ2=0.164, r=-0.064, P=0.685 | χ2=0.522, r=-0.088, P=0.470 | χ2=0.239, r=- 0.068, P=0.625 | |||||
| Diet | |||||||
| Vegetarian | 95 | 25 (26) | 70 (74) | 42 (44) | 53 (56) | 48 (51) | 47 (49) |
| Veg+Non-veg | 48 | 17 (35) | 31 (65) | 21 (44) | 27 (56) | 20 (42) | 28 (58) |
| χ2=1.273, r=-0.094, P=0.262 | χ2=0.003, r=+0.004, P=0.959 | χ2=1.004, r=+0.084, P=0.320 | |||||
| Tumor site | |||||||
| Colon | 69 | 14 (20) | 55 (80) | 35 (51) | 34 (49) | 32 (46) | 37 (54) |
| Rectum | 74 | 28 (38) | 46 (62) | 28 (38) | 46 (62) | 36 (49) | 38 (51) |
| χ2=5.300, r=-0.193, P=0.021 | χ2=2.406, r=+0.130, P=0.123 | χ2=0.074, r=- 0.023, P=0.788 | |||||
| Tumor Location# | |||||||
| Right side | 45 | 8 (18) | 37 (82) | 23 (51) | 22 (49) | 23 (51) | 22 (49) |
| Left side | 98 | 34 (35) | 64 (65) | 40 (41) | 58 (59) | 45 (46) | 53 (54) |
| χ2=4.254, r=-0.172, P=0.039 | χ2=1.326, r=+0.096, P=0.253 | χ2=0.333, r=+0.048, P=0.567 | |||||
| Tumor Size | |||||||
| T2 | 36 | 07 (19) | 29 (81) | 16 (44) | 20 (56) | 16 (44) | 20 (56) |
| T3 | 95 | 20 (21) | 75 (79) | 39 (41) | 56 (59) | 39 (41) | 56 (59) |
| T4 | 12 | 02 (17) | 10 (83) | 08 (67) | 04 (33) | 08 (67) | 04 (33) |
| χ2=0.148, r=+0.002, P=0.983 | χ2=2.839, r=-0.056, P=0.508 | χ2=2.839, r=- 0.056, P=0.508 | |||||
| Nodal Status | |||||||
| Negative | 90 | 27 (30) | 63 (70) | 38 (42) | 52 (58) | 40 (44) | 50 (56) |
| Positive | 53 | 15 (28) | 38 (72) | 25 (47) | 28 (53) | 28 (53) | 25 (47) |
| χ2=0.046, r=+0.018, P=0.831 | χ2=0.331, r=-0.048, P=0.568 | χ2=0.941, r=- 0.081, P=0.336 | |||||
| TNM Stage | |||||||
| I | 24 | 08 (33) | 16 (67) | 12 (50) | 12 (50) | 13 (54) | 11 (46) |
| II | 64 | 19 (30) | 45 (70) | 24 (38) | 40 (62) | 26 (41) | 38 (59) |
| III | 51 | 14 (27) | 37 (73) | 23 (45) | 28 (55) | 27 (53) | 24 (47) |
| IV | 4 | 01 (25) | 03 (75) | 04 (100) | 00 (00) | 02 (50) | 02 (50) |
| χ2=0.312, r=+0.045, P=0.591 | χ2=6.562, r=-0.058, P=0.490 | χ2=2.256, r=- 0.035, P=0.676 | |||||
| Early (I+II) | 88 | 27 (31) | 61 (69) | 36 (41) | 52 (59) | 39 (44) | 49 (56) |
| Advanced (III+IV) | 55 | 15 (27) | 40 (73) | 27 (49) | 28 (51) | 29 (53) | 26 (47) |
$$ \begin{array}{l} \chi 2 = 0. 1 9 0, \\ \mathrm {r} = + 0. 0 3 6, \\ \mathrm {P} = 0. 6 6 6 \\ \end{array} $$ $$ \begin{array}{l} \chi 2 = 0. 9 1 9, \\ \mathrm {r} = - 0. 0 8 0, \\ \mathrm {P} = 0. 3 4 1 \\ \end{array} $$ Tumor Differentiation Well 29 13 (45) 16 (55) 11 (38) 18 (62) 13 (45) 16 (55) Moderate/Poor 114 29 (25) 85 (75) 52 (46) 62 (54) 55 (48) 59 (52) $$ \begin{array}{l} \chi 2 = 4. 1 9 0, \\ \mathrm {r} = + 0. 1 7 1, \\ \mathrm {P} = 0. 0 4 1 \\ \end{array} $$ $$ \begin{array}{l} \chi 2 = 0. 5 5 4, \\ \mathrm {r} = - 0. 0 6 2, \\ \mathrm {P} = 0. 4 6 0 \\ \end{array} $$ Histologic Type Adenocarcinoma 103 29 (28) 74 (72) 45 (44) 58 (56) 48 (47) 55 (53) Mucinous/Signet ring cell 40 13 (33) 27 (67) 18 (45) 22 (55) 20 (50) 20 (50) $$ \begin{array}{l} \chi 2 = 0. 2 6 2, \\ \mathrm {r} = - 0. 0 4 3, \\ \mathrm {P} = 0. 6 1 2 \\ \end{array} $$ $$ \begin{array}{l} \chi 2 = 0. 0 2 0, \\ \mathrm {r} = - 0. 0 1 2, \\ \mathrm {P} = 0. 8 8 8 \\ \end{array} $$ Lymphatic Permeation Absent 112 30 (27) 82 (73) 48 (43) 64 (57) 55 (49) 57 (51) Present 31 12 (39) 19 (61) 15 (48) 16 (52) 13 (42) 18 (58) $$ \begin{array}{l} \chi 2 = 1. 6 6 4, \\ \mathrm {r} = - 0. 1 0 8, \\ \mathrm {P} = 0. 2 0 0 \\ \end{array} $$ $$ \begin{array}{l} \chi 2 = 0. 3 0 1, \\ \mathrm {r} = - 0. 0 4 6, \\ \mathrm {P} = 0. 5 8 6 \\ \end{array} $$ Vascular Permeation Absent 136 40 (29) 96 (71) 61 (45) 75 (55) 67 (49) 69 (51) Present 7 02 (29) 05 (71) 02 (29) 05 (71) 01 (14) 06 (86) $$ \begin{array}{l} \chi 2 = 0. 0 0 0, \\ \mathrm {r} = + 0. 0 0 4, \\ \mathrm {P} = 1. 0 0 0 \\ \end{array} $$ $$ \begin{array}{l} \chi 2 = 0. 2 0 8, \\ \mathrm {r} = + 0. 0 7 1, \\ \mathrm {P} = 0. 6 4 8 \\ \end{array} $$ Lymphocytic Stromal Response Absent 120 36 (30) 84 (70) 48 (40) 72 (60) 58 (48) 62 (52) Present 23 06 (26) 17 (74) 15 (65) 08 (35) 10 (43) 13 (57) $$ \begin{array}{l} \chi 2 = 0. 1 4 2, \\ \mathrm {r} = + 0. 0 3 2, \\ \mathrm {P} = 0. 7 0 8 \\ \end{array} $$ $$ \begin{array}{l} \chi 2 = 4. 9 8 0, \\ \mathrm {r} = - 0. 1 8 7, \\ \mathrm {P} = 0. 0 2 6 \\ \end{array} $$ Perineural Invasion Absent 126 36 (29) 90 (71) 58 (46) 68 (54) 58 (46) 68 (54) Present 17 06 (35) 11 (65) 05 (29) 12 (71) 10 (59) 07 (41) χ2=0.083, r=-0.048, P=0.774 χ2=1.679, r=+0.108, P=0.198 Necrosis χ2=0.960, r=- 0.082, P=0.331 χ2=0.108, r=- 0.028, P=0.744 χ2=0.133, r=- 0.031, P=0.717 $$ \begin{array}{l} \chi 2 = 0. 5 0 1, \\ \mathrm {r} = + 0. 0 5 9, \\ \mathrm {P} = 0. 4 8 3 \\ \end{array} $$ $$ \begin{array}{l} \chi 2 = 2. 0 1 4, \\ \mathrm {r} = + 0. 1 5 1, \\ \mathrm {P} = 0. 1 5 6 \\ \end{array} $$ $$ \begin{array}{l} \chi 2 = 0. 1 8 2, \\ \mathrm {r} = + 0. 0 3 6, \\ \mathrm {P} = 0. 6 7 2 \\ \end{array} $$ χ2=0.983, r=- 0.083, P=0.325
| Absent | 133 | 41 (31) | 92 (69) | 55 (41) | 78 (59) | 65 (49) | 68 (51) |
|---|---|---|---|---|---|---|---|
| Present | 10 | 01 (10) | 09 (90) | 08 (80) | 02 (20) | 03 (30) | 07 (70) |
| χ2=1.070, r=+0.117, P=0.301 | χ2=4.177, r=-0.199, P=0.041 | χ2=0.679, r=+0.096, P=0.410 | |||||
| Pre-op circulating CEA (ng/ml) (N=131) | |||||||
| < 5.0 | 68 | 21 (31) | 47 (69) | 30 (44) | 38 (56) | 38 (56) | 30 (44) |
| ≥ 5.0 | 63 | 19 (30) | 44 (70) | 30 (48) | 33 (52) | 26 (41) | 37 (59) |
| χ2=0.008, r=+0.008, P=0.929 | χ2=0.162, r=-0.035, P=0.691 | χ2=2.795, r=+0.146, P=0.096 |
Table 3: Correlation of ERCC1 C118T, ERCC2 Lys751Gln, XRCC1 Arg399Gln polymorphisms with clinicopathological parameters. *Alcohol
| ERCC2 Lys751Gln | XRCC1 Arg399Gln | |
|---|---|---|
| Individual three genotypes | ||
| ERCC1 C118T | r=-0.053 | r=-0.083 |
| ERCC1 C118T | P=0.533 | P=0.323 |
| ERCC2 Lys751Gln | - | r=+0.288 |
| ERCC2 Lys751Gln | - | P<0.001 |
| Wild vs variant type | ||
| ERCC1 C118T | r=-0.016 | r=-0.061 |
| ERCC1 C118T | P=0.854 | P=0.472 |
| ERCC2 Lys751Gln | - | r=+0.255 |
| ERCC2 Lys751Gln | - | P=0.002 |
Table 4: Intercorrelation of DNA repair gene polymorphisms.
Intercorrelation of Polymorphisms in DNA Repair Genes
When intercorrelation of polymorphisms (individual three genotypes) was performed, the nonparametric Spearman’s correlation revealed a significant positive correlation between ERCC2 and XRCC1 polymorphisms (P<0.001). Additionally, when wild vs combined variant type was intercorrelated, again a significant positive correlation of ERCC2 was observed with XRCC1 polymorphism (P=0.002) (Table 3).
Discussion
In cancer, disruption in DNA repair pathways predisposes cells to accumulate DNA damage, leading to biological aggressive tumors and also affecting the treatment response to cytotoxic drugs and survival [23]. Therefore, understanding the underlying mechanism of DNA repair pathways, particularly the role of DNA repair genes is an important avenue for today’s treatment. In CRC, various studies described that polymorphisms in DNA repair genes, especially ERCC1, ERCC2, and XRCC1 may affect the clinical outcome in patients treated with adjuvant oxaliplatin-based chemotherapy [22]. However, scarce reports available for the clinicopathological association of these polymorphisms in CRC. As clinicopathological factors of the tumor holds important value for prognosis of patients [21], present study aimed to evaluate the correlation of ERCC1 C118T, ERCC2 Lys751Gln and XRCC1 Arg399Gln polymorphisms with clinicopathological parameters in CRC patients.
In present study, ERCC1 C118T polymorphism demonstrated higher frequency of heterozygous variant C/T genotype (56%) as compared to wild type C/C (29%) and homozygous variant T/T (15%) genotypes in CRC patients. Accordingly, preponderance of C/T genotype was observed by several other studies in CRC [24, 25]. On the other side, there exist several reports on high incidence of C/C genotype in CRC patients. Fariada, et al. [26] reported 78% of C/C genotype as compared to 8% of C/T and 14% of T/T genotypes in CRC. Similar predominance of C/C genotypes was observed in numerous studies in patients with primary CRC [15, 27, 28], metastatic CRC [29], advanced gastric cancer [30], esophageal squamous cell carcinoma [31] and late stage bladder cancer [32]. The inconsistency in genotype distribution in different studies might be due to different sample size, variability in ethnicity and environmental and lifestyle related factors.
In relation to clinicopathological parameters, present study showed a significant higher incidence of ERCC1 118 variant genotypes (C/T+T/T) in colon cancer, in right side located tumors and in moderately/poorly differentiated tumors as compared to rectal cancer, left side located tumors and well differentiated tumors, respectively. This result proposes the higher occurrence of variant T allele of ERCC1 118 polymorphism in tumors located in colon as compared to rectum in studied patients. However, Huang, et al. [15] did not find any statistically significant correlations between ERCC1 C118T genotype distribution and gender, tumor location, depth of tumor invasion, lymph node metastasis, cancer stage or histology in CRC patients. Smith, et al. [25] also found no association between ERCC1 C118T genotypes and clinicopathologic variables in ovarian cancer. On the other side, Huang, et al. [33] in gastric cancer detected a trend of high incidence of variant genotypes (C/T+T/T) in advanced stage patients.
ERCC2 Lys751Gln polymorphism showed 44% of A/A (Lys/Lys), 40% A/C (Lys/Gln) and 16% C/C (Gln/Gln) genotypes in CRC patients. Consistent with present results, similar frequencies were observed by Le Morvan, et al. [34] and Gan, et al. [18] in CRC. While several other studies in CRC showed predominance of ERCC2 751 A/A genotype ranging from 69% to 92% [7, 15, 35, 36, 37]. On the other hand, some studies reported predominance of Lys/Gln genotype in CRC [38, 39]. Identical results were observed in esophageal cancer [40]. Present study was conducted in Western Indian population and in accordance with the frequencies of our study, Srivastava, et al. [41] in north Indian population showed the frequencies of A/A (40.4%), A/C (44.8%) and C/C (14.8%) genotypes in gallbladder cancer. While another study, in Kashmir Valley of India, reported 69% of A/A, 19% of A/C and 12% of C/C genotypes for ERCC2 Lys751Gln polymorphism in gastric cancer [42].
Correlation of ERCC2 Lys751Gln polymorphism with clinicopathological parameters reported significant association of combined variant genotypes (A/C+C/C) with absence of lymphocytic stromal response (P=0.026) and necrosis (P=0.041). This result proposes the link between variant C allele and less aggressiveness of tumor. In CRC, Huang, et al. [15, 43] found no statistically significant correlation between ERCC2 Lys751Gln genotype distributions and gender, tumor location, depth of tumor invasion, lymph node metastasis, cancer stage or histology. Lai, et al. [35] also found no significant association of ERCC2 Lys751Gln polymorphism with clinicopathological parameters in metastatic CRC. Similarly, Giachino, et al. [44] in lung cancer observed no association of ERCC2 751 genotypes with patient and tumor characteristics such as age, smoke, gender, performance status, histology, and disease stage.
Further, current study reported 48% G/G (Arg/Arg), 42% G/A (Arg/Gln) and and 10% A/A (Gln/Gln) frequencies for XRCC1 Arg399Gln polymorphism in CRC patients. In accordance, Ruzzo, et al. [45] observed 49% of G/G, 43% of G/A and 8% of G/G genotypes for XRCC1 399 in advanced CRC. Similar results were observed by Stoehlmacher, et al. [39] in CRC patients. Accordingly, Zhao and Chen [46] and Cheng, et al. [47] observed comparable results in NSCLC and ovarian cancer patients, respectively. On the other side, in patients with sporadic CRC, predominance of Arg/Gln (53.33%) was reported as compared to Arg/Arg (28%) and Gln/Gln (18.67%) [48]. Analogous frequencies were observed by Chua, et al. [49] showing predominance of G/A heterozygotes (53%) in metastatic CRC. In Indian population, Nissar, et al. [50] in a hospital-based case-control study of CRC patients in Kashmir, showed that among the CRC cases, the frequencies of the XRCC1 genotypes were 48.5% (G/G), 28.5% (A/G) and 23.0% (A/A). On other hand, another study conducted by Khan, et al. [51] on Kashmiri population, demonstrated a preponderance of G/A genotype in colorectal cases (66.7%) and controls (42.5%).
In present study, XRCC1 Arg399Gln polymorphism was not significantly correlated with any of the clinicopathological parameters. Only a trend of higher incidence of variant genotypes (G/A+A/A) was observed in patients with abnormal pre-op circulating CEA levels ≥5.0 ng/ml (P=0.096). Therefore, it can be suggested that variant A allele may be associated with aggressive behavior of tumor due to its correlation with abnormal high CEA levels in circulation. In accordance with our results, no significant association of Arg399Gln polymorphism with clinicopathological parameters was found in CRC patients [51]. Giachino, et al. [44] in lung cancer also observed that XRCC1 399 genotypes were not associated with patient and tumor characteristics such as age, smoke, gender, performance status, histology, and disease stage. However, Nissar, et al. [50] demonstrated a significant association of the A allele with age, gender, dwelling, tumor location, nodal status and tumor grade of the CRC patients. Further, Chen, et al. [13] in gastric cancer observed significant differences in terms of age, gender, and family history of cancer between the cases and controls.
When polymorphisms in DNA repair genes intercorrelated, ERCC2 and XRCC1 polymorphisms were significantly associated with each other suggesting the intercorrelation of different DNA repair pathways in CRC.
Conclusion
Present study showed higher occurrence of variant C/T and T/T genotypes of ERCC1 118 polymorphism in patients with colon cancer and right side located tumors in western Indian population. Furthermore, variant C allele of ERCC2 Lys751Gln polymorphism might be associated with less aggressiveness of tumor due to its higher frequency found in patients having absence of lymphocytic stromal response and necrosis. However, XRCC1 Arg399Gln polymorphism could not show any significant role in relation to clinicopathological parameters. In addition, significant positive correlation between ERCC2 and XRCC1 polymorphisms suggests the link between DNA repair genes of different DNA repair pathways, which might have a significant role in CRC.
Acknowledgement
We are extremely thankful to Medical Oncology Department and Surgical Oncology Department, The Gujarat Cancer & Research Institute, for providing their support to fulfil the present study
Conflict of Interest
None
References
-
Safiri S, Sepanlou SG, Ikuta KS, Bisignano C, Salimzadeh H, et al. (2019) The global, regional, and national burden of colorectal cancer and its attributable risk factors in 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Gastroenterol Hepatol 4(12): 913-933.
-
Salimzadeh H, Lindskog EB, Gustavsson B, Wettergren Y, Ljungman D (2020) Association of DNA repair gene variants with colorectal cancer: risk toxicity and survival. BMC cancer 20: 409.
-
Ma SC, Zhao Y, Zhang T, Ling XL, Zhao D (2015) Associa- tion between the ERCC1 rs11615 polymorphism and clinical outcomes of oxaliplatin-based chemotherapies in gastrointestinal cancer: a meta-analysis. Onco Targets Ther 8: 641- 648.
-
Isla D, Sarries C, Rosell R, Alonso G, Domine M, et al. (2004) Single nucleotide polymorphisms and outcome in docetaxel–cisplatin-treated advanced non-small-cell lung cancer. Ann Oncol 15(8): 1194-1203.
-
Jiraskova K, Hughes DJ, Brezina S, Gumpenberger T, Veskrnova V, et al. (2019) Functional polymorphisms in DNA repair genes are associated with sporadic colorectal cancer susceptibility and clinical outcome. Int J Mol Sci 20(1): 97.
-
Vodicka P, Vodenkova S, Buchler T, Vodickova L (2019) DNA repair capacity and response to treatment of colon cancer. Pharmacogenomics 20(17): 1225-1233.
-
Dong Y, Liu JW, Gao YJ, Zhou T, Chen YM (2015) Relationship between DNA repair gene XPD751 single- nucleotide polymorphisms and prognosis of colorectal cancer. Genetics and Molecular Research 14(2): 5390- 5398.
-
Lamas MJ, Duran G, Balboa E, Bernardez B, Touris M, et al. (2011) Use of a comprehensive panel of biomarkers to predict response to a fluorouracil–oxaliplatin regimen in patients with metastatic colorectal cancer. Pharmacogenomics 12(3): 433-442.
-
Siewchaisakul P, Suwanrungruang K, Poomphakwaen K, Wiangnon S, Promthet S (2016) Lack of Association between an XRCC1 Gene Polymorphism and Colorectal Cancer Survival in Thailand. Asian Pac J Cancer Prev 17(4): 2055-2060.
-
Yin M, Yan J, Martinez-Balibrea E, Graziano F, Lenz HJ, et al. (2011) ERCC1 and ERCC2 polymorphisms predict clinical outcomes of oxaliplatin-based chemotherapies in gastric and colorectal cancer: a systemic review and meta-analysis. Clin Cancer Res 17(6): 1632-1640.
-
Kiran M, Saxena R, Kaur J (2010) Distribution of XRCC1 genotypes in north Indian population. The Indian Journal of Medical Research 131(1): 71-75.
-
Huang Y, Li X, He J, Chen L, Huang H, et al. (2015) Genetic polymorphisms in XRCC1 genes and colorectal cancer susceptibility. World J Surg Oncol 13: 244.
-
Chen S, Zhu XC, Liu YL, Wang C, Zhang KG (2016) Investigating the association between XRCC1 gene polymorphisms and susceptibility to gastric cancer. Genetics and Molecular Research 15(3): gmr.15038342.
-
Uppal V, Mehndiratta M, Mohapatra D, Grover RK (2014) XRCC-1 gene polymorphism (Arg399Gln) and susceptibility to development of lung cancer in cohort of north Indian population: A pilot study. J Clin Diagn Res 8(11): CC17-CC20.
-
Huang MY, Wang JY, Huang ML, Chang HJ, Lin SR (2013) Polymorphisms in XPD and ERCC1 associated with colorectal cancer outcome. Int J Mol Sci 14(2): 4121- 4134.
-
Chai H, Pan J, Zhang X, Zhang X, Shen X, et al. (2012) ERCC1 C118T associates with response to FOLFOX4 chemotherapy in colorectal cancer patients in Han Chinese. Int J Clin Exp Med 5(2): 186-194.
-
Kumamoto K, Ishibashi K, Okada N, Tajima Y, Kuwabara K, et al. (2013) Polymorphisms of GSTP1, ERCC2 and TS3’UTR are associated with the clinical outcome of mFOLFOX6 in colorectal cancer patients. Oncol Lett 6(3): 648-654.
-
Gan Y, Li XR, Chen DJ, Wu JH (2012) Association between polymorphisms of XRCC1 Arg399Gln and XPD Lys751Gln genes and prognosis of colorectal cancer in a Chinese population. Asian Pac J Cancer Prev 13(11): 5721-5724.
-
Liang J, Jiang T, Yao RY, Liu ZM, Lv HY, et al. (2010) The combination of ERCC1 and XRCC1 gene polymorphisms better predicts clinical outcome to oxaliplatin-based chemotherapy in metastatic colorectal cancer. Cancer Chemother Pharmacol 66(3): 493-500.
-
Zaanan A, Dalban C, Emile JF, Blons H, Fléjou JF, et al. (2014) ERCC1, XRCC1 and GSTP1 single nucleotide polymorphisms and survival of patients with colon cancer receiving oxaliplatin-based adjuvant chemotherapy. J Cancer 5(6): 425-432.
-
Marks KM, West NP, Morris E, Quirke P (2018) Clinicopathological, genomic and immunological factors in colorectal cancer prognosis. Br J Surg 105(2): 99-109.
-
Gajjar K, Kobawala T, Vora H, Ghosh N (2020) The Ability of Polymorphisms in DNA Repair Enzymes to Predict Clinical Outcome in Colorectal Cancer Patients. Middle East Journal of Cancer 11(3): 260-272.
-
Kelley MR, Logsdon D, Fishel ML (2014) Targeting DNA repair pathways for cancer treatment: what’s new? Future Oncol 10(7): 1215-1237.
-
Viguier J, Boige V, Miquel C, Pocard M, Giraudeau B, et al. (2005) ERCC1 codon 118 polymorphism is a predictive factor for the tumor response to oxaliplatin/5- fluorouracil combination chemotherapy in patients with advanced colorectal cancer. Clin Cancer Res 11(17): 6212-6217.
-
Smith S, Su D, Rigault de la Longrais IA, Schwartz P, Puopolo M, et al. (2007) ERCC1 genotype and phenotype in epithelial ovarian cancer identify patients likely to benefit from paclitaxel treatment in addition to platinum-based therapy. J Clin Oncol 25(33): 5172-5179.
-
Fariada BAB, Elsheikh AE, Adila SE-O (2015) Diagnostic and predictive DNA markers in sudanese patients with colorectal cancer “The impact of ERCC1, XPD, Kras and APC gene’s polymorphism on sudanese patients with colorectal cancer”. World Journal of Pharmaceutical Research 4(7): 174-192.
-
Chao CT, Wu YL, Hsu TF, Wang JY, Chang LS, et al. (2014) Polymorphisms in EGFR, GSTP1, XPD, DPD, ERCC1, and UTG1A1 of colorectal cancer patients treated with 5-fluorouracil plus oxaliplatin or irinotecan chemotherapy. Biomarkers and Genomic Medicine 6(4): 183-185.
-
Ni M, Zhang WZ, Qiu JR, Liu F, Li M, et al. (2014) Association of ERCC1 and ERCC2 polymorphisms with colorectal cancer risk in a Chinese population. Sci Rep 4: 4112.
-
Chang PM, Tzeng CH, Chen PM, Lin JK, Lin TC, et al. (2009) ERCC1 codon 118 C→ T polymorphism associated with ERCC1 expression and outcome of FOLFOX‐4 treatment in Asian patients with metastatic colorectal carcinoma. Cancer Sci 100(2): 278-283.
-
Qi YJ, Cui S, Yang YZ, Han JQ, Cai BJ, et al. (2013) Excision repair cross-complementation group 1 codon 118 polymorphism, micro ribonucleic acid and protein expression, clinical outcome of the advanced gastric cancer response to first-line FOLFOX-4 in Qinghai- Tibetan plateau population. J Cancer Res Ther 9(3): 410- 415.
-
Yu X, Xiao H, Zhao B, Zhang X, Wang G, et al. (2015) DNA repair gene ERCC1 C118T polymorphism predicts sensitivity of recurrent esophageal cancer to radiochemotherapy in a Chinese population. Thorac Cancer 6(6): 741-748.
-
Xu ZC, Cai HZ, Li X, Xu WZ, Xu T, et al. (2016) ERCC1 C118T polymorphism has predictive value for platinum- based chemotherapy in patients with late-stage bladder cancer. Genet Mol Res 15(2): 7801.
-
Huang ZH, Hua D, Du X, Li LH, Mao Y, et al. (2008) ERCC1 polymorphism, expression and clinical outcome of oxaliplatin-based adjuvant chemotherapy in gastric cancer. World J Gastroenterol 14(41): 6401-6407.
-
Le Morvan V, Smith D, Laurand A, Brouste V, Bellott R, et al. (2007) Determination of ERCC2 Lys751Gln and GSTP1 Ile105Val gene polymorphisms in colorectal cancer patients: relationships with treatment outcome. Pharmacogenomics 8(12): 1693-1703.
-
Lai JI, Tzeng CH, Chen PM, Lin JK, Lin TC, et al. (2009) Very low prevalence of XPD K751Q polymorphism and its association with XPD expression and outcomes of FOLFOX‐4 treatment in Asian patients with colorectal carcinoma. Cancer Sci 100(7): 1261-1266.
-
Kumamoto K, Ishibashi K, Okada N, Tajima Y, Kuwabara K, et al. (2013) Polymorphisms of GSTP1, ERCC2 and TS3’UTR are associated with the clinical outcome of mFOLFOX6 in colorectal cancer patients. Oncol Lett 6: 648-654.
-
Dong Y, Chen XY, Liu JW, Chen YM (2016) Correlation between SNPs of XPD751, XPD312 and chemotherapeutic efficacy in colorectal carcinoma patients. Int J Clin Exp Med 9(7): 12967-12975.
-
Park DJ, Stoehlmacher J, Zhang W, Tsao-Wei DD, Groshen S, et al. (2001) A Xeroderma pigmentosum group D gene polymorphism predicts clinical outcome to platinum- based chemotherapy in patients with advanced colorectal cancer. Cancer Res 61(24): 8654-8658.
-
Stoehlmacher J, Park DJ, Zhang W, Yang D, Groshen S, et al. (2004) A multivariate analysis of genomic polymorphisms: prediction of clinical outcome to 5-FU/ oxaliplatin combination chemotherapy in refractory colorectal cancer. Br J Cancer 9(2)1: 344-354.
-
Bradbury PA, Kulke MH, Heist RS, Zhou W, Ma C, et al. (2009) Cisplatin pharmacogenetics, DNA repair polymorphisms, and esophageal cancer outcomes. Pharmacogenet Genomics 19(8): 613-625.
-
Srivastava K, Srivastava A, Mittal B (2010) Polymorphisms in ERCC2, MSH2, and OGG1 DNA repair genes and gallbladder cancer risk in a population of Northern India. Cancer 116(13): 3160-3169.
-
Ashraf R, Kadla SA, Wani HA, Bhatt AA, Majid S (2015) Gastric Cancer Risk and XPD/ERCC2 SNPS (LYS751GLN, ASP312ASN) Gene Polymorphism-An Experimental Study in Kashmir Valley of India. European Academic Research 2(11): 14146-14159.
-
Huang MY, Fang WY, Lee SC, Cheng TL, Wang JY, et al. (2008) ERCC2 2251A> C genetic polymorphism was highly correlated with early relapse in high-risk stage II and stage III colorectal cancer patients: a preliminary study. BMC Cancer 8: 50.
-
Giachino DF, Ghio P, Regazzoni S, Mandrile G, Novello S, et al. (2007) Prospective assessment of XPD Lys751Gln and XRCC1 Arg399Gln single nucleotide polymorphisms in lung cancer. Clin Cancer Res 13(10): 2876-2881.
-
Ruzzo A, Graziano F, Loupakis F, Rulli E, Canestrari E, et al. (2007) Pharmacogenetic profiling in patients with advanced colorectal cancer treated with first-line FOLFOX-4 chemotherapy. J Clin Oncol 25(10): 1247- 1254.
-
Zhao R, Chen G (2015) Role of GSTP1 Ile105Val and XRCC1 Arg194Trp, Arg280His and Arg399Gln gene polymorphisms in the clinical outcome of advanced non- small cell lung cancer. Int J Clin Exp Pathol 8(11): 14909- 14916.
-
Cheng CX, Xue M, Li K, Li WS (2012) Predictive value of XRCC1 and XRCC3 gene polymorphisms for risk of ovarian cancer death after chemotherapy. Asian Pac J Cancer Prev 13(6): 2541-2545.
-
Procopciuc LM, Osian G (2013) Lys751Gln XPD and Arg399Gln XRCC1 in Romanians. Association with sporadic colorectal cancer risk and different stages of carcinomas. Chirurgia 108(5): 711-718.
-
Chua W, Goldstein D, Lee CK, Dhillon H, Michael M, et al. (2009) Molecular markers of response and toxicity to FOLFOX chemotherapy in metastatic colorectal cancer. Br J Cancer 101(6): 998-1004.
-
Nissar S, Lone TA, Banday MZ, Rasool R, Chowdri NA, et al. (2013) Arg399Gln polymorphism of XRCC1 gene and risk of colorectal cancer in Kashmir: a case control study. Oncol Lett 5(3): 959-963.
-
Khan NP, Pandith AA, Yousuf A, Khan NS, Khan MS, et al. (2013) The XRCC1 Arg399Gln gene polymorphism and risk of colorectal cancer: a study in Kashmir. Asian Pac J Cancer Prev 14(11): 6779-6782.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma