Ganglioneuronal Differentiation in Ewings Sarcoma of the Chest Wall (Askin Tumour): An Uncommon Post-Chemotherapy Change
Ewing sarcoma is classified under undifferentiated small round cell sarcomas of bone and soft tissue. Such tumours arising in the chest wall were previously called Askin’s tumour, however this terminology is not preferred at present. These tumours classically have a small round cell morphology and fusion of FET family of genes (usually EWSR1) with a member of the ETS family of transcription factors. Rare cases of Ewing sarcoma are found to have extensive neural differentiation with ganglion cells and neuropil at diagnosis as well as following chemotherapy. We report a 12 year old boy who presented with a large mass in the right hemi-thorax, which was diagnosed as Ewing sarcoma with EWSR1 translocation by FISH. However, following four cycles of chemotherapy (Vincristine, Doxorubicin, Cyclophosphamide alternating with ifosphamide and etoposide), the resection specimen showed predominantly neural differentiation mimicking a ganglioneuroma with only small areas of small round cell component. EWSR1 translocation was also demonstrated in the resection specimen. After a period of nine months, the child presented with recurrence at the same site and was treated with Irinotecan, cyclophosphamide with topotecan and temozolamide giving excellent clinical response. In this paper, we emphasize the rare occurrence of extensive neural differentiation in Ewing sarcoma and the need to revisit the upfront chemotherapy protocols for patients who exhibit this rare phenomenon
Introduction
Ewing sarcoma is the second most common sarcoma of bone and soft tissue in children and adolescents, the most common sarcoma being osteosarcoma. It can occur at various extra-osseous sites like the thorax (Askin tumour), lung, kidney, etc [1]. Classically, Ewing sarcoma has an excellent response to conventional chemotherapy using vincristine, doxorubicin, cyclophosphamide, iphosphamide, etoposide with significant reduction in tumour size after the first cycle [2]. Rarely, the tumour exhibits extensive neural differentiation following chemotherapy [3, 4, 5, 6].
Here, we present a molecularly proven case of Ewing sarcoma with ganglioneuroma-like differentiation after chemotherapeutic treatment. Although the data on follow up and survival is limited, our patient presented with a local recurrence at the same site and was treated with irinotecan, cyclophosphamide alternating with topotecan and temozolamide yielding excellent clinical outcome and no evidence of residual disease.
Case Report
A 12 year old previously healthy and well grown boy presented with right sided chest pain and breathing difficulty which progressed gradually over 2 weeks. On examination the child had tachycardia (heart rate 130/min) and tachypnea (respiratory rate 42/min). Breath sounds were absent on the right side causing severe respiratory distress. X-ray chest showed complete opacification of right hemithorax with left shift of mediastinum (Figure 1A). CECT chest revealed a large heterogeneous lobulated mass measuring 14.2 x 11.8 x 8.9cm in right mid hemi-thorax with involvement of right lateral chest wall and erosion of lateral aspect of right third rib with moderate pleural effusion. A provisional diagnosis of Ewings tumour was considered and ultrasound guided trucut biopsy was performed. Histopathology revealed a tumour arranged in sheets and composed of small round cells with hyperchromatic nuclei and scant cytoplasm. Scattered large cells with prominent nucleoli were seen. The tumour cells showed diffuse and strong membranous positivity for CD99 and EWSR1 translocation was demonstrated by break apart FISH.
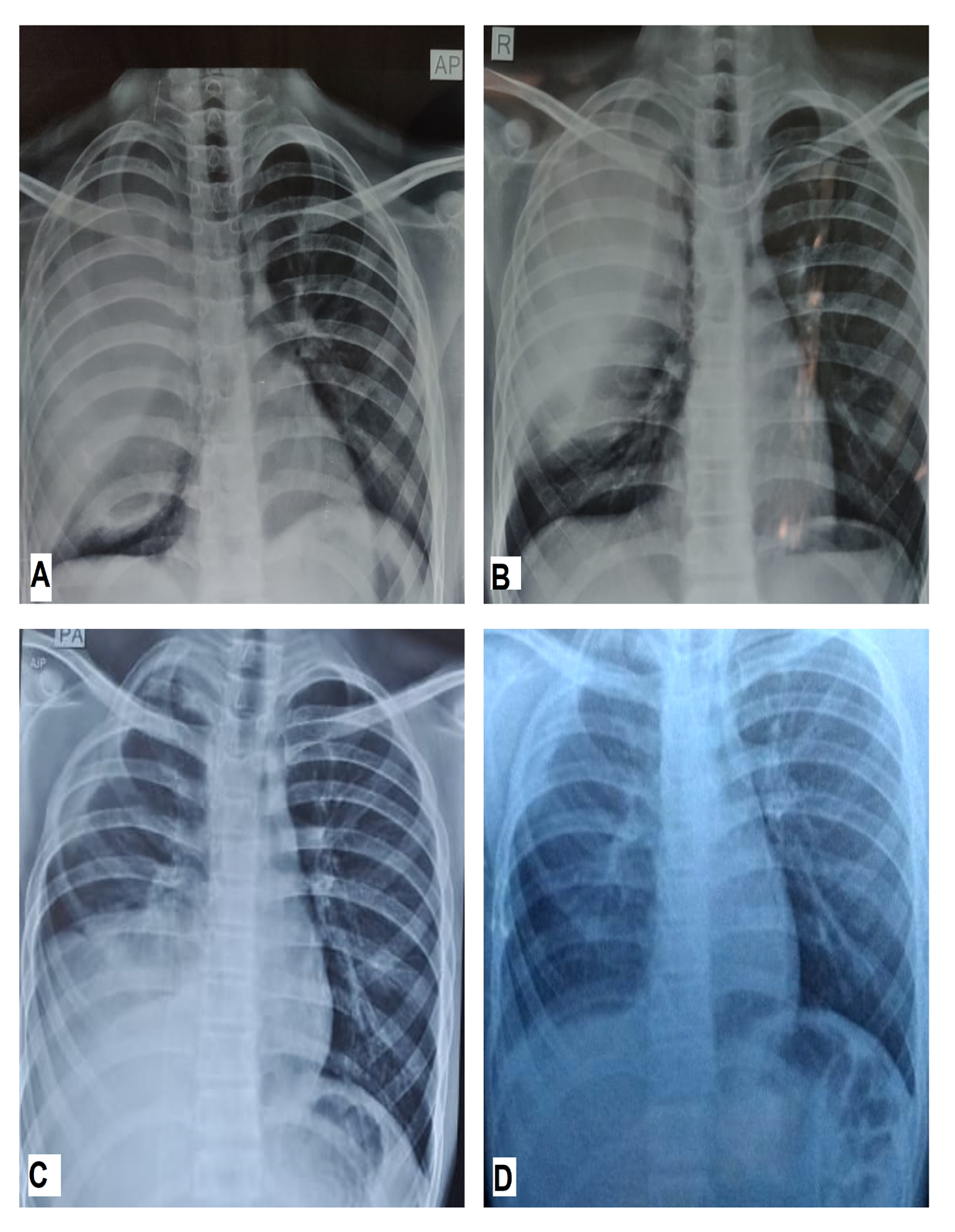
Whole body PET scan confirmed localised disease without distant metastasis. The child was treated with neo-adjuvant chemotherapy using cycles of Vincristine, Doxorubicin, Cyclophosphamide alternating with ifosphamide and etoposide as per COG protocol. The tumor showed reduction in size after the first cycle with resolution of the pleural effusion helping in symptomatic relief for the child. However after the second cycle, no significant shrinkage in the tumor size could be appreciated on the chest X-ray (Figure 1B). In spite of four cycles of neo-adjuvant chemotherapy, there was no decrease in the size of the tumor. For local control of the disease, surgery with complete excision of the tumor was done. The gross examination the resected specimen showed a large, well circumscribed tumour, with a grayish brown pseudo-capsule (Figure 2). On sectioning, the tumour showed a fleshy gray white cut surface. Tumour was seen arising from the rib focally. On microscopic examination, low- power view showed two distinct tumour components. The first component is small round blue cells arranged in clusters and nests with brisk mitosis. These areas represented classic Ewing sarcoma, which were seen merging with the predominant loosely cellular areas with a ‘pink’ appearance on low power. The latter on high power examination showed neuropil like fibrillary material, within which were many large cells with eccentric nucleus, prominent nucleoli and moderate to abundant eosinophilic cytoplasm resembling ganglion cells. EWSR1 translocation was once again confirmed on the resection specimen.
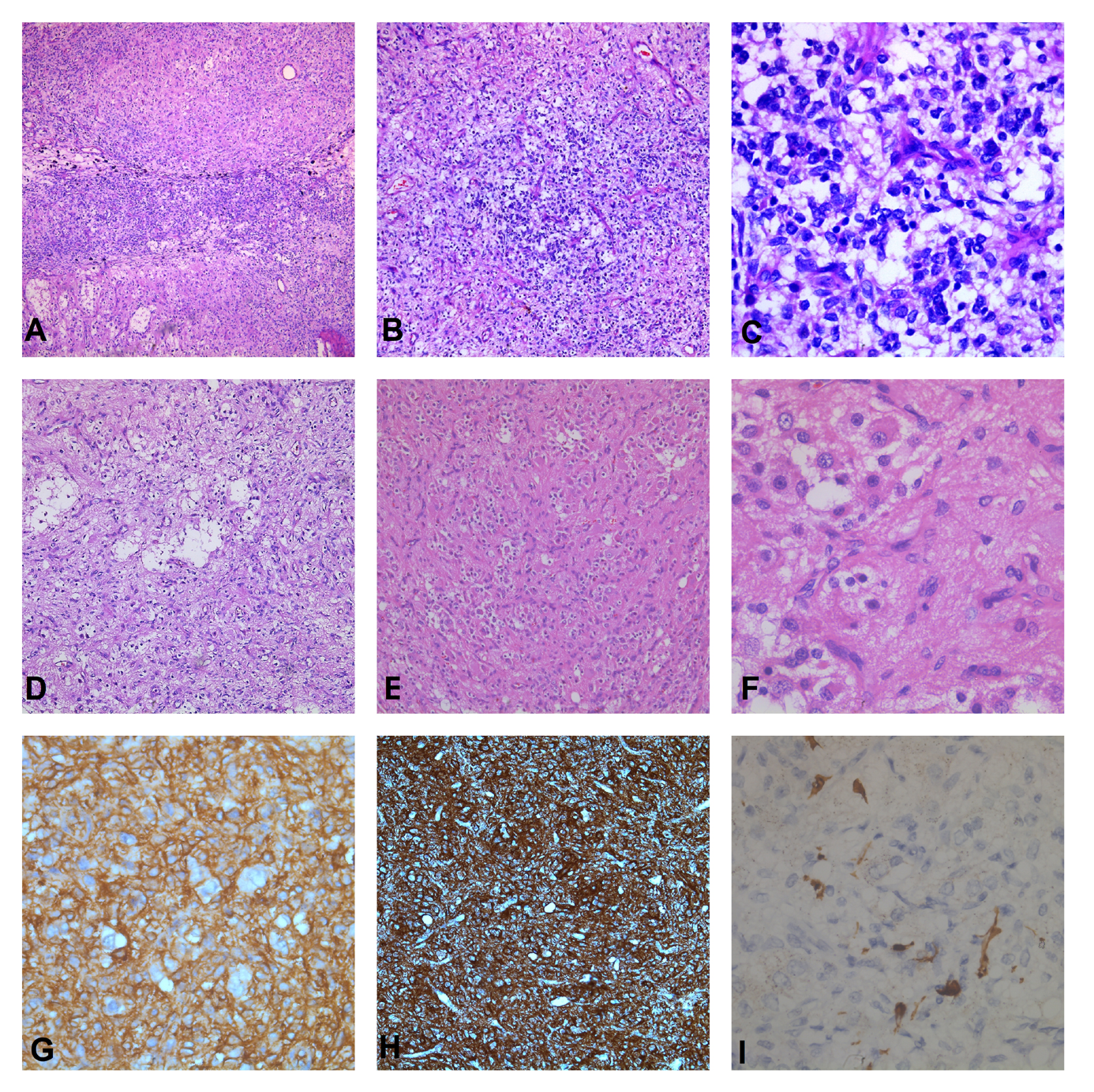
Figure 2: A-F) Histopathology of the resection specimen, H&E stain. A&B) Two components of the tumour with loosely cellular ‘pink’ areas (black star) and ‘blue’ cell areas (red star), 40X and 100X C) Small cells with hyperchromatic, round to mildly ovoid nuclei and scant cytoplasm, 400X. D) Loosely cellular areas, 100X E) Large neuronal cells in a fibrillary matrix, 200X F) Ganglion cells (arrow) set in a fibrillary matrix, 400X.
G-I) Immunohistochemistry stain. G) Diffuse and strong membrane positivity for CD99, 200X. H) Neural matrix showing strong positivity for synaptophysin, 100X. I) Cell bodies of ganglion cells highlighted by S100 stain, 400X.
Adjuvant radiation was given to the post-operative site in a dose of 50.4Gy in 28 fractions, 1.8Gy/ fraction for 5 days in a week for 5 weeks. Rapid arc technique was used with deep inspiratory breath hold and daily image guidance using cone beam CT and 6D couch correction on True beam STx. The patient was given remaining 10 cycles of adjuvant chemotherapy completing the total 14 cycles as per COG protocol. PET CT scan was done 6 months after completion of treatment and showed no metabolically active disease anywhere in the body. However 3 months after the PET scan (9 months after completion of treatment) the child presented with chest pain and breathing difficulty. CECT chest was suggestive of recurrence of the tumor at the same site. PET scan revealed only localised disease without any distant metastasis. Again, keeping the curative intent in mind second line chemotherapy using Irinotecan, cyclophosphamide with topotecan and temozolamide was used for induction. This time the tumor showed significant reduction in size after first two cycles of induction chemotherapy. The patient has completed four cycles of induction chemotherapy with good response.
Discussion
Differentiation of primitive stem cells/ neural crest cells de novo or following chemotherapy are known to occur in certain tumours like teratoma and neuroblastoma [7]. However this type of differentiation is rare in Ewing sarcoma and has been published sporadically as single case reports. In our patient, the tumour showed extensive neural differentiation with many ganglion cells and microscopically, the low power appearance was mimicking a ganglioneuroma. High grade small cell areas were scanty and seen only as small patches. Presence of isolated high grade, small round cell areas may pose a diagnostic challenge, especially in small biopsies when representative tissue is not obtained. In these circumstances, resection of the entire tumour may be needed to reach the correct diagnosis.
In Ewing sarcoma, some authors have reported presence of ganglion like cells and neural differentiation following chemotherapy [3, 4, 5, 6]. In our patient, when we reviewed the slides of the initial biopsy, we could find scattered large cells with prominent nucleoli, which were distinctly seen apart from the small round cells. However, the exact nature of these cells could not be delineated since the tissue was scanty for any further immunohistochemical evaluation. Also, in view of inadequate clinical response to chemotherapy and extensive neural differentiation, we reconfirmed the diagnosis of Ewing sarcoma by repeating the FISH on the resection specimen. Other important feature that is worth to be noted in our case is that it is extremely rare for ganglioneuroma to arise from the rib and present as a chest wall mass. Spectrum of neuroblastic tumours including ganglioneuroma are common in the posterior mediastinum, while isolated cases have been reported in the lung (primary pulmonary ganglioneuroblastoma) [8].
Molecular diagnosis by FISH helped us reach the correct diagnosis of Ewing sarcoma of the chest wall, inspite of unclear morphology with extensive neuronal differentiation. Previous reports mention ganglioneuromatous differentiation in Ewings sarcoma of bone and soft tissue. To the best of our knowledge, our case is the first case of Askin tumour (Ewings sarcoma of chest wall) showing extensive neural differentiation. We have demonstrated EWSR1 translocation in the initial biopsy as well as in the resection specimen post-chemotherapy. It is important to keep in mind that such neural differentiation can occur in Ewing, especially following chemotherapy and one should not be misled in making a diagnosis. Because ganglion cells are the mature neuronal cells, they will be inherently resistant to first line chemotherapeutic regimen designed for a primitive round cell sarcoma such as Ewing sarcoma. However, whether addition of agents targeting mature neuronal cells will yield a better response in induction or during adjuvant chemotherapy phase, needs to be explored.
Many aspects are yet to be explored and addressed pertaining to this phenomenon of neuronal differentiation in Ewings sarcoma. The overall survival of Ewing sarcoma of chest wall is reported to be around 65% [9]. As more literature becomes available with time, it needs to be discussed if neuronal differentiation has impact on long term outcome of these patients. Whether to modify the chemotherapy post surgery or even at upfront diagnosis with presence of ganglion-like large cells, in an otherwise histologically and molecularly proven Ewing sarcoma is an important point to be addressed in the future.
References
-
(2020) WHO Classification of Tumours Editorial Board. WHO Classification of Tumours of Soft Tissue and Bone 5th (Edn.), Lyon, France: IARC.
-
Womer RB, West DC, Krailo MD, Dickman PS, Pawel BR, et al. (2012) Randomized controlled trial of interval- compressed chemotherapy for the treatment of localized Ewing sarcoma: a report from the Children’s Oncology Group. J Clin Oncol 30(33): 4148-4154.
-
Salet MC, Vogels R, Brons P, Schreuder B, Flucke U (2016) Maturation toward neuronal tissue in a Ewing sarcoma of bone after chemotherapy. Diagn Pathol 11(1): 74.
-
Weissferdt A, Kalhor N, Moran CA (2015) Ewing sarcoma with extensive neural differentiation: a clinicopathologic, immunohistochemical, and molecular analysis of three cases. Am J Clin Pathol 143(5): 659-664.
-
Collini P, Mezzelani A, Modena P, Dagrada P, Tamborini E, et al. (2003) Evidence of neural differentiation in a case of post-therapy primitive neuroectodermal tumor/ Ewing sarcoma of bone. Am J Surg Pathol 27(8): 1161- 1166.
-
Ushigome S, Shimoda T, Nikaido T, Nakamori K, Miyazawa Y, et al. (1992) Primitive neuroectodermal tumors of bone and soft tissue with reference to histologic differentiation in primary or metastatic foci. Acta Pathol Jpn 42(7): 483-493
-
Lowichik A, Zhou H, Pysher TJ, Smith L, Lemons R, et al. (2000) Therapy associated changes in childhood tumors. Adv Anat Pathol 7(6): 341-359.
-
Hochholzer L, Moran CA, Koss MN (1998) Primary pulmonary ganglioneuroblastoma: a clinicopathologic and immunohistochemical study of two cases. Ann Diagn Pathol 2(3): 154-158.
-
Esiashvili N, Goodman M, Marcus RB Jr (2008) Changes in incidence and survival of Ewing sarcoma patients over the past 3 decades: Surveillance Epidemiology and End Results data. J Pediatr Hematol Oncol. 30(6): 425-430.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma