The Token Transition-Minimal Deviation Adenocarcinoma Uterine Cervix
Gastric type adenocarcinoma is a high grade, frequently discerned mucinous adenocarcinoma with gastric differentiation incriminating the endocervical canal. Of obscure aetiology, neoplasm depicts STK11 genetic mutations with chromosome 3q gain and chromosome 1p loss. Tumefaction exhibits cytological and histological features of gastric differentiation as tumour cells incorporated with voluminous, clear or pale, foamy, eosinophilic cytoplasm, tall, abundant, apical mucin, miniature, spherical, elliptical or enlarged, basal nuclei, irregular, vesicular chromatin and prominent nucleoli. The well differentiated neoplasm is comprised of well defined glandular articulations and minimal to absent stromal desmoplastic reaction. Neoplastic glands of variable outline, magnitude and irregular or claw-like glandular contour are observed. Tumour cells appear immune reactive to HIK1083, MUC6, p53, carcinoembryonic antigen (CEA) or mCEA, CK7, PAX8, CAIX or HNF-1B. Minimal deviation adenocarcinoma requires segregation from neoplasms such as human papillomavirus (HPV) associated endocervical adenocarcinoma, human papillomavirus (HPV) associated endocervical adenocarcinomas intestinal(goblet cell) type, clear cell adenocarcinoma, invasive stratified mucin producing adenocarcinoma, metastatic gastric or pancreaticobiliary carcinoma, lobular endocervical glandular hyperplasia, atypical lobular endocervical glandular hyperplasia, diffuse laminar endocervical glandular hyperplasia, tunnel clusters, florid deep glands, microglandular hyperplasia, pseudo-infiltrative tubal metaplasia, endocervicosis, endosalpingosis or endocervical type adenomyoma. Minimal deviation adenocarcinoma can be adequately categorized upon histological examination of tissue obtained with surgical sampling. Stage I tumours may be managed with surgical procedures as trachelectomy or radical hysterectomy and regional lymphadenectomy upon initial disease representation.
Introduction
Gastric type adenocarcinoma is a frequently exemplified, mucinous adenocarcinoma with gastric differentiation incriminating the uterine cervix. The inherently high grade, endocervical neoplasm is non- concurrent with human papilloma virus (HPV) infection. Appropriate disease discernment may be challenging within accrued miniature tissue samples or cytological preparations. Prognostic outcomes are inferior, in contrast to human papilloma virus (HPV) associated conventional endocervical adenocarcinoma. Well differentiated gastric type adenocarcinoma is additionally designated as minimal deviation adenocarcinoma or adenoma malignum. Minimal deviation adenocarcinoma with gastric differentiation commonly incriminates the endocervix [1]. Gastric type adenocarcinoma configures an estimated 10% of endocervical adenocarcinomas. Mean age of disease emergence is 50 years although tumour may appear within 30 years to 66 years [2, 3].
Non-Essential Precursor Lesions of Gastric type Adenocarcinoma may Configure as
- Gastric metaplasia associated with type A tunnel clusters.
- Lobular endocervical glandular hyperplasia appears adjoining to ~50% of minimal deviation adenocarcinomas and ~20% of gastric type adenocarcinomas.
- Atypical lobular endocervical glandular hyperplasia may concur with ~30% of minimal deviation adenocarcinomas.
- Gastric type adenocarcinoma in situ [2, 3].
Of obscure aetiology, neoplasm depicts STK11 genetic mutations with chromosome 3q gain and chromosome 1p loss. Around 50% lesions delineate TP53 genetic mutations. Although neoplasm is associated with sporadic disease emergence, lesion may concur with germline STK11 genomic mutations or Peutz-Jeghers syndrome [2, 3]. Asymptomatic subjects with gastric type adenocarcinoma manifest with aberrant features on cervical cytology. Besides, clinical symptoms as mucoid or profuse, watery vaginal discharge, vaginal bleeding and abdominal discomfort may be observed. Uterine cervix appears barrel shaped or demonstrates a tumefaction. Distant metastasis into uterine adnexa may emerge [2, 3].
Cytological examination exhibits crowded clusters and singularly disseminated tumour cells incorporated with pale, foamy or vacuolated cytoplasm and moderately pleomorphic, spherical to elliptical nuclei with singular or multiple nucleoli. Cytoplasmic margins are well defined. An acute inflammatory cell exudate of neutrophils appears admixed with the necrotic debris. Intracytoplasmic mucins delineate yellowish orange hue upon Papanicolaou stain.
Atypical glandular epithelial cells discerned with Papanicolaou stained smears appear immune non reactive to human papilloma virus (HPV), a feature indicative of gastric type adenocarcinoma of uterine cervix. Smears obtained from minimal deviation adenocarcinoma may be challenging to interpret as demarcation from reactive endocervical cells may be infeasible [3, 4]. Generally, sheets of glandular cells delineating a ‘honeycomb’ pattern are observed. Tumour cells are pervaded with abundant, non vacuolated cytoplasm and cytoplasmic extensions or cytoplasmic tails, uniform spherical to elliptical nuclei, fine nuclear chromatin and miniature nucleoli.
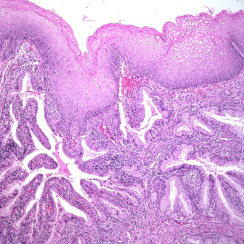
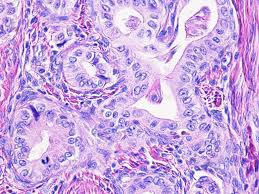
Neoplastic cells appear devoid of significant cellular or nuclear pleomorphism. Mitotic figures are infrequent to absent. Occasionally, prominent and displaced hyperchromatic nuclei pervaded with clumped nuclear chromatin may be observed [3, 4]. Grossly, minimal deviation adenocarcinoma is associated with an unremarkable uterine cervix. Alternatively, cervical hypertrophy with multiple cystic lesions may ensue. Tumefaction represents as an exophytic, papillary, polypoid or ulcerated tumour mass. Cervical wall appears indurated or demonstrates diffuse or nodular enlargement. Cut surface exhibits tan or yellow, haemorrhagic, friable or mucoid neoplastic foci. Upon microscopy, lesion delineates cytological and histological features of gastric differentiation denominated as ~tumour cells incorporated with voluminous, clear or pale, foamy, eosinophilic cytoplasm, tall, abundant, apical mucin, miniature, spherical, elliptical or enlarged, basal nuclei, irregular, vesicular chromatin and prominent nucleoli. Cellular perimeter is distinct. Mitotic activity is variable. Foci of intestinal differentiation as goblet cells and Paneth-like neuroendocrine cells may be observed.
Exceptionally, foci of mucin extravasation, adenocarcinoma in situ or gastric metaplasia may be exemplified [4, 5]. Cogent architectural features appear as well differentiated neoplasm comprised of well defined glandular articulations and minimal to absent stromal desmoplastic reaction. Besides, poorly differentiated configurations comprised of infiltrative, inadequately articulated glands, tumour cell nests or disseminated singular cells and goblet cells may be associated with stromal desmoplastic reaction. Tumour grading of gastric type adenocarcinoma of uterine cervix is not recommended as well differentiated tumours may enunciate aggressive biological behaviour. Commingling of well differentiated and poorly differentiated areas may be discerned [4, 5].
Poorly differentiated gastric type adenocarcinoma delineates significantly atypical tumour cells with an absence of abundant cytoplasm. Disseminated singular cells and cellular clusters may be exemplified. Aforesaid neoplasms are designated as ‘gastric type’ on account of discernible pyloric gland type mucin. Upon morphological assessment, immunoreactivity and phenotype, tumour appears reminiscent of pancreatobiliary adenocarcinoma. Tumefaction is associated with lymphatic, vascular or perineural invasion. Morphologic concurrence between human papillomavirus associated conventional endocervical adenocarcinoma and gastric type adenocarcinoma of uterine cervix is encountered. Human papillomavirus (HPV) associated neoplasms delineating few virus associated morphological features, simulating gastric type adenocarcinoma of uterine cervix are documented [4, 5]. Minimal deviation adenocarcinoma characteristically displays neoplastic glands of variable outline, magnitude and irregular or claw-like glandular contour. Deep seated invasion of cervical stroma with haphazard dissemination of glandular structures and minimal to absent desmoplastic reaction may be exemplified. The low grade tumefaction demonstrates accumulation of abundant, apical intracytoplasmic mucin and minimal to absent cytological atypia. ‘Pure’ minimal deviation adenocarcinoma can be misinterpreted on account of bland morphological countenance. However, appropriate tissue sampling may identify complex neoplastic evolution with focal cytological atypia [4, 5]. Upon ultrastructural examination, neoplastic cells configuring minimal deviation adenocarcinoma demonstrate HIK1083 reactive mucin confined to the matrix and lysozyme into mucin granules cores, indicative of gastric phenotype [4, 5] (Figures 1 & 2).
TNM Staging of Carcinoma Cervix 2021 as per American Joint Committee on Cancer (Version 9)
Primary Tumour
- TX: primary tumour cannot be assessed [3, 4]
- T0: no evidence of primary tumour
- Tis: carcinoma in situ
- T1: carcinoma cervix confined to the uterus and subcategorized as
- T1a: invasive carcinoma singularly diagnosed by microscopy with depth of invasion < 5 millimetres
- T1b: clinically visible lesion confined to the cervix
- T2: carcinoma cervix which invades beyond the uterus with absent extension to pelvic wall or lower third of vagina
- T2a: tumour with absence of parametrial invasion
- T2b: tumour associated with parametrial invasion
- T3: tumour extends into pelvic wall and/or involves lower third of vagina, and/or causes hydronephrosis
- T3a: tumour involves lower third of vagina with absent extension into pelvic wall
- T3b: tumour extends into pelvic wall and/or causes hydronephrosis or nonfunctioning kidney
- T4: tumour invades mucosa of urinary bladder or rectum and/or extends beyond true pelvis
Regional Lymph Nodes
- NX: regional lymph nodes cannot be assessed
- N0: regional lymph node metastasis absent
- N1: regional lymph node metastases singularly confined to pelvic lymph nodes
- N2: regional lymph node metastasis into para-aortic lymph nodes along with or devoid of pelvic lymph node metastasis
Distant Metastasis
- M0: distant metastasis absent
- M1: distant metastasis into sites such as pulmonary parenchyma, hepatic parenchyma, distant or inguinallymph nodes, bone or intraperitoneal disease. Tumour metastasis into pelvic lymph nodes, para-aortic lymph nodes or vagina are to be excluded.
Minimal deviation adenocarcinoma can be subjected to Periodic acid Schiff(PAS)- Alcian blue stain which stains neutral mucin of gastric type mucinous epithelium red or magenta. Tumour cells appear immune reactive to HIK1083, MUC6, p53, carcinoembryonic antigen (CEA) or mCEA, CK7, PAX8, CAIX or HNF-1B. Focal immune reactivity to CK20, CDX2, CA19-9 or CA-125 may be observed. Neoplastic cells appear immune non-reactive to p16, oestrogen receptor(ER), progesterone receptor (PR) or PAX2. Human papilloma virus (HPV) appears non-reactive upon in situ hybridization(ISH) or polymerase chain reaction (PCR) [5, 6].
Minimal deviation adenocarcinoma requires segregation from neoplasms such as human papillomavirus (HPV) associated endocervical adenocarcinoma, human papillomavirus (HPV) associated endocervical adenocarcinomas intestinal(goblet cell) type, clear cell adenocarcinoma, invasive stratified mucin producing adenocarcinoma, metastatic gastric or pancreaticobiliary carcinoma, lobular endocervical glandular hyperplasia, atypical lobular endocervical glandular hyperplasia, diffuse laminar endocervical glandular hyperplasia, tunnel clusters, florid deep glands, microglandular hyperplasia, pseudo- infiltrative tubal metaplasia, endocervicosis, endosalpingosis or endocervical type adenomyoma [5, 6].
Appropriate discernment of the benign appearing minimal deviation adenocarcinoma may be challenging. Minimal deviation adenocarcinoma can be adequately categorized upon histological examination of tissue obtained with surgical sampling. Upon ultrasonography, a hypoechoic, heterogeneous tumefaction is observed. Ultrasonography of minimal deviation adenocarcinoma depicts multi-locular cystic masses. Upon colour Doppler, intralesional vascularity is occasionally enhanced. Magnetic resonance imaging (MRI) exhibits a mass lesion demonstrating elevated signal intensity, in contrast to minimal signal intensity delineated by surrounding cervical stroma. Magnetic resonance imaging (MRI) demonstrates multiple, irregular, cystic lesions or cysts configuring floret-like pattern with aggregates of miniature cysts exemplifying a ‘cosmos’ pattern [5, 6].
Cogent therapeutic strategies appear contingent to factors such as stage of disease representation and recapitulates treatment modalities applicable to varieties of adenocarcinoma. Majority of subjects manifest with advanced, stage II to stage IV neoplasms upon initial tumour discernment. Stage I tumours may be managed with surgical extermination procedures as trachelectomy or radical hysterectomy and regional lymphadenectomy upon initial disease representation. Advanced grade neoplasms may be aptly treated with neoadjuvant chemotherapy or radiotherapy. Aggressive neoplasms unresponsive to chemotherapy appear associated with propensity for peritoneal and abdominal tumour dissemination. Stage I neoplasms exhibit 5 year disease specific survival at 62%. In contrast, stage I human papilloma virus (HPV) associated, conventional endocervical adenocarcinoma delineates 5 year disease specific survival at 96%. Additionally, 5 year disease specific survival within comprehensive stages emerges at 32% [5, 6].
References
-
Nucci MR, Clement PB, Young RH (1999) Lobular endocervical glandular hyperplasia, not otherwise specified: a clinicopathologic analysis of thirteen cases of a distinctive pseudoneoplastic lesion and comparison with fourteen cases of adenoma malignum. Am J Surg Pathol 23(8): 886-891.
-
Guo N, Liu H (2023) A rare case of minimal-deviation adenocarcinoma of the uterine cervix with ovarian metastasis. Asian J Surg 46(7): 2733-2734.
-
You X, He L, Lin Y, Huang L, Wang X, et al. (2023) Case Report: A rare case of gastric-type adenocarcinoma of stumps of duplicated cervices in a 49-year-old woman: A case with hidden focus confused us a lot. Front Oncol 13: 1109731.
-
Kobara H, Miyamoto T, Ando H, Asaka R, Takatsu A, et al. (2020) Limited frequency of malignant change in lobular endocervical glandular hyperplasia. Int J Gynecol Cancer 30(10): 1480-1487.
-
Nishio S, Mikami Y, Tokunaga H, Yaegashi N, Satohet T, et al. (2019) Analysis of gastric-type mucinous carcinoma of the uterine cervix-an aggressive tumor with a poor prognosis: a multi-institutional study. Gynecol Oncol 153(1): 13-19.
-
Yoshino A, Kobayashi E, Tsuboyama T, Fukui H, Tomiyama N, et al. (2023) Novel Strategy for the Management of Cervical Multicystic Diseases. Ann Surg Oncol 30(5): 2964-2973.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma