Spectrum of Diabetic Kidney Disease in India - A Tertiary Care Centre Experience
Objectives / Aim of study: To assess the magnitude, clinico-social risk factors and associations of diabetic kidney disease in type 2 diabetes subjects attending a tertiary care centre in Eastern India. Materials and Methods: It was a cross-sectional hospital based observational study. Approximately two fifty (250) consecutive type 2 diabetes subjects aged 18 to 60 years attending the OPD of Endocrinology, Nilratan Sircar Medical College and Hospital were recruited and screened for DKD on the basis of urine ACR and eGFRvalues. Type 2 diabetes subjects with pregnancy, eGFR less than 15 ml/min /1.73 m2, urinary tract infection, hematuria, decompensated heart failure, liverfailure, systemic infections, debilitating illness were excluded from the study. After detailed history taking and clinical examination, necessary investigations were done for each patient and the results were analyzed. Results: The prevalence of DKD was 34% and moderately increased albuminuria (ACR 30 to 300 microgm/mg) was the commonest form of presentation of DKD. Patients with DKD had a significantly higher DM duration, higher BMI, lower HbA1c, higher serum potassium, more dylipidemia and anemia. Malesex, smoking, family history of DKD, erectile dysfunction, VPT abnormality and foot ulcer were significantly associated with DKD. Conclusion: The prevalence of albuminuria was considerably high among diabetes subjects in this area. Longer duration of diabetes, malesex, smoking, family history of DKD and neuropathy were the important risk factors for DKD. Regular screening for DKD and early intervention for multiple modifiable risk factors may prevent this dreaded complication of Type 2 Diabetes Mellitus.
Introduction
Type 2 diabetes mellitus is a highly prevailing disease in developing countries of South Asia including India. Global estimates for the year 2030 predict a further growth of almost 50%, with the greatest increase in the developing countries of Africa, South America and Asia [1]. It is estimated that ten years down the lane, one in every five diabetics will be an Indian [2]. Type 2 diabetes mellitus is associated with multiorgan damage, with renal and cardiovascular involvement being highly critical. Diabetic kidney disease (DKD), without timely intervention, can lead to end stage renal disease (ESRD). The earliest clinical evidence of DKD is albuminuria, which is also a strong risk factor for cardiovascular disease [3]. Routine screening for albuminuria is an easy and inexpensive predictive procedure for DKD and can guide appropriate intervention, thereby minimizing disease progression. In developing countries like India, 30% of chronic renal failures can be attributed to diabetic kidney disease [4] and the high cost of treating end stage renal disease precludes many such patients from availing optimal therapy. Early identification of patients at high risk for development and progression of DKD is therefore, important to intensify the treatment and modify associated risk factors. Till date there is sparse information and scarcity of data on the magnitude, risk factors and progression of diabetic nephropathy among type 2 diabetes subjects from developing countries like India, particularly from the eastern part, though being such a significant contributor to morbidity and mortality. This study was taken up to assess the magnitude, clinico- social risk factors and associations of diabetic nephropathy in type 2 diabetes subjects in a clinical referral hospital in eastern India.
Materials and Methods
It was a cross-sectional hospital based observational study. Approximately two fifty (250) consecutive type 2 diabetes subjects aged 18 to 60 years attending the outpatient department of Endocrinology, Nilratan Sircar Medical College and Hospital were recruited and screened for DKD on the basis of urine ACR and eGFRvalues. Type 2 diabetes subjects with pregnancy,urinary tract infection, hematuria, decompensated heart failure, liverfailure, systemic infections, debilitating illness and other comorbid conditions that may adversely affect renal function, and on drugs that may adversely affect renal function were excluded from the study. Informed consent was obtained from the subjects and Institutional Ethical Clearance was obtained for the study. All the patients were interviewed with pre-designed questionnaire. Type 2 diabetes was diagnosed according to recent American Diabetes Association (ADA) criteria. Demographic, anthropometric and haemodynamic details like age, gender, height, weight, systolic and diastolic blood pressure (SBP and DBP), family history of diabetes and duration of diabetes were recorded at baseline. Measurements of weight, height, and waist circumference were obtained using standardized techniques. All anthropomorphic measures reflect the average of two measurements (measured by the same person on the same instrument to avoid inter-instrument and interpersonal variation). Blood pressure (BP) was measured two times in the sitting position after 10 minutes of rest with a manual mercury sphygmomanometer and the two readings were averaged. Subjects with self reported hypertension and those who had a systolic blood pressure of 140 mmHg and/or diastolic blood pressure of 90 mmHg were considered to have hypertension. The BMI was calculated using the following formula: weight (kg)/height (m2). Details of oral hypoglycaemic agents (OHA), antihypertensives and other drugs prescribed and presence of other diabetic complications like diabetic retinopathy (DR) and diabetic neuropathy were noted at baseline.Screening for increased urinary albumin excretion was performed by measurement of the albumin-to-creatinine ratio (ACR) in a random spot collection following precautions as per recommendation of recent ADA guideline, after exclusion of factors that may elevate urinary albumin excretion over baseline values. Estimated glomerular filtration rate (eGFR) was calculated using CKD-EPI formula. All patients were under standard management with follow up as per recommendation of recent ADA guideline.Necessary investigations were done including complete hemogram,plasma glucose-fasting and two (2) hour post prandial,glycated hemoglobin (HbA1c), serum urea, creatinine, sodium, potassium, uric acid, lipid profile, urine routine & microscopic examination(R/E& M/E), spot urine for albumin/creatinine ratio (ACR), ECG, liver function tests and vibration perception threshold (VPT).
Statistical Analysis
Descriptive statistical analysis has been carried out for the present study. Results on continuous measurements are presented on Mean ± SD and results on categorical measurements are presented in Number (%). Significance is assessed at a level of 5 %. It was assumed that cases of the samples should be independent,the populations from which the samples are drawn have the same variance (or standard deviation), the samples drawn from different populations are random. Normality of data is tested by Anderson Darling test, Shapiro-Wilk, Kolmogorov- Smirnoff test and visually by QQ plot. Unpaired t-test has been used to find the significance of study parameters between two groups of patients. Chi-square/ Fisher Exact test has been used to find the significance of study parameters on categorical scale between two or more groups. The Statistical software namely SAS 9.2, SPSS 21.0 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc.
Results
Total 250 patients were included in the study out of which 85 had DKD on the basis of ACR and eGFR values. The prevalence of diabetic kidney disease (DKD) in this study was 34% (n=85) (Figure 1).
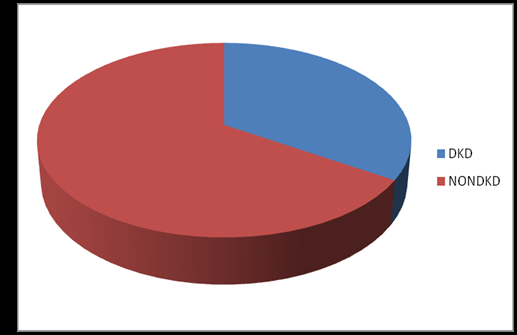
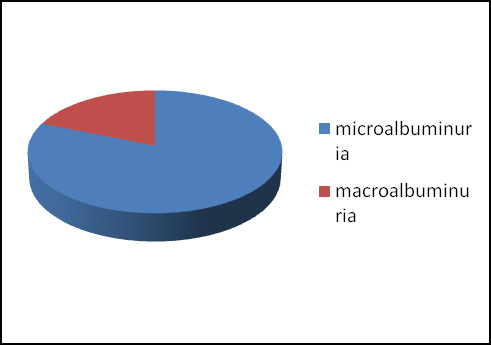
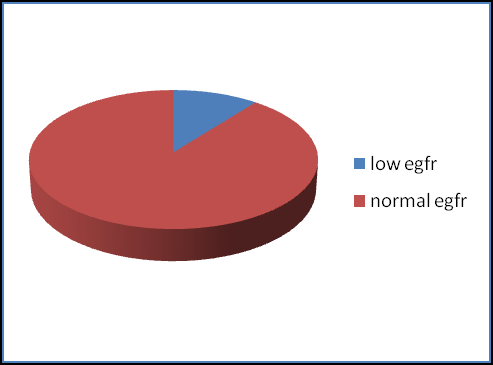
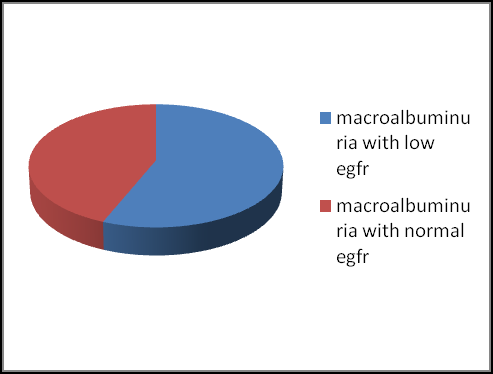
Figure 4: Mean age of presentation in non DKD patients was 49.8 years, average duration of diabetes 7.9 years, mean BMI 26.1 kg/m2, mean HbA1c 8.9%, mean ACR 15.69 microgm/mg. Mean lipid values were-HDL C- 48.4mg/dl, LDLC- 113.2 mg/dl, TG-165.7 mg/dl (Table 1). Mean age of presentation in DKD patients was 50.8 years, average duration of diabetes 9.8 years, mean BMI 27.5 kg/m2, mean HbA1c 8.0%, mean ACR 491 microgm/mg. Mean lipid values were-HDL C- 44.7 mg/dl, LDLC- 129 mg/dl, TG-197 mg/dl (Table 1).
| Variables | Cohort | N | Mean | Std. Deviation | Std. Error Mean | P |
|---|---|---|---|---|---|---|
| Age(years) | Non-Nephropathy | 165 | 49.85 | 7.490 | .585 | 0.28 |
| Age(years) | Nephropathy | 85 | 50.85 | 6.578 | .714 | 0.28 |
| DM duration(years) | Non-Nephropathy | 165 | 7.95 | 3.046 | .237 | <0.001 |
| DM duration(years) | Nephropathy | 85 | 9.86 | 4.141 | .449 | <0.001 |
| BMI(kg/m2) | Non-Nephropathy | 165 | 26.154 | 3.4988 | .2724 | 0.005 |
| BMI(kg/m2) | Nephropathy | 85 | 27.488 | 3.5835 | .3887 | 0.005 |
| SBP(mm Hg) | Non-Nephropathy | 165 | 144.84 | 20.989 | 1.634 | 0.057 |
| SBP(mm Hg) | Nephropathy | 85 | 150.14 | 20.332 | 2.205 | 0.057 |
| DBP(mm Hg) | Non-Nephropathy | 165 | 82.62 | 5.962 | .464 | 0.267 |
| DBP(mm Hg) | Nephropathy | 85 | 83.46 | 4.844 | .525 | 0.267 |
| FPG(mg/dl) | Non-Nephropathy | 165 | 130.72 | 25.498 | 1.985 | 0.167 |
| FPG(mg/dl) | Nephropathy | 85 | 135.61 | 28.237 | 3.063 | 0.167 |
| PPPG(mg/dl) | Non-Nephropathy | 165 | 193.19 | 38.589 | 3.004 | 0.053 |
| PPPG(mg/dl) | Nephropathy | 85 | 203.44 | 41.087 | 4.456 | 0.053 |
| Urea(mg/dl) | Non-Nephropathy | 165 | 27.51 | 8.388 | .653 | 0.014 |
| Urea(mg/dl) | Nephropathy | 85 | 31.01 | 13.964 | 1.515 | 0.014 |
| HbA1C (%) | Non-Nephropathy | 165 | 8.91 | 1.03 | 0.1 | <0.001 |
| HbA1C (%) | Nephropathy | 85 | 8.01 | 0.92 | 0.1 | <0.001 |
| Creatinine(mg/dl) | Non-Nephropathy | 165 | .886 | .2300 | .0179 | <0.001 |
| Creatinine(mg/dl) | Nephropathy | 85 | 1.100 | .5211 | .0565 | <0.001 |
| K+ | Non-Nephropathy | 165 | 3.639 | .5208 | .0405 | <0.001 |
| K+ | Nephropathy | 85 | 6.673 | 9.5400 | 1.03 | <0.001 |
| Uric acid | Non-Nephropathy | 165 | 5.298 | 1.2419 | .0967 | 0.109 |
| Uric acid | Nephropathy | 85 | 5.604 | 1.7165 | .1862 | 0.109 |
| Hb% | Non-Nephropathy | 165 | 12.23 | 2.194 | .171 | <0.001 |
| Hb% | Nephropathy | 85 | 11.10 | 3.248 | .352 | <0.001 |
| HDL(mg/dl) | Non-Nephropathy | 165 | 48.48 | 5.728 | .446 | <0.001 |
| HDL(mg/dl) | Nephropathy | 85 | 44.78 | 7.338 | .796 | <0.001 |
| LDL(mg/dl) | Non-Nephropathy | 165 | 113.29 | 30.621 | 2.384 | <0.001 |
| LDL(mg/dl) | Nephropathy | 85 | 128.94 | 38.491 | 4.175 | <0.001 |
Table 1: Nephropathy vs. non nephropathy.
In comparison with patients without kidney disease, patients with DKD had a significantly higher DM duration (p<0.001), higher BMI (p=0.005), lower HbA1c (p<0.001), higher serum potassium levels, lower HDL-C level, higher triglyceride, higher LDL-C levels (p<0.001) and lower Hemoglobin values (p<0.001). Male sex (p=0.008), family history of DKD and past history of foot ulcer were significantly associated with DKD.The DKD cohort had significantly more erectile dysfunction and active foot ulcer.Though symptoms of diabetic neuropathy were not reported with increased frequency in the DKD cohort, VPT abnormality was significantly more in this cohort(p=0.005). Both former and recent smoking status showed significant association with DKD, compared to the non DKD group (Table 1 & 2). The following parameters did not show any significant difference in the two cohorts after analysis: age of patient, history suggestive of hypoglycemia, exercise pattern of the subjects,retinopathy,ECG and USG abnormality (Table 1).
| Sex | Total | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | P | |||||||||||||
| F | M | |||||||||||||
| Cohort | Non-Nephropathy | Count | 88 | 77 | 165 100.0% 85 100.0% 250 100.0% | 0.008 | ||||||||
| % | 53.3% | 46.7% | ||||||||||||
| Nephropathy | Count | 30 | 55 | |||||||||||
| % | 35.3% | 64.7% | ||||||||||||
| Total | Count | 118 | 132 | |||||||||||
| % | 47.2% | 52.8% |
| F/H/O DKD | Total | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | P | ||||||||||
| No | Yes | ||||||||||
| Cohort | Non-Nephropathy | Count | 161 | 4 | 165 | <0.001 | |||||
| % | 97.6% | 2.4% | 100.0% | ||||||||
| Nephropathy | Count | 40 | 45 | 85 | |||||||
| % | 47.1% | 52.9% | 100.0% | ||||||||
| Total | Count | 201 | 49 | 250 | |||||||
| % | 80.4% | 19.6% | 100.0% |
Table 2B: F/H/O DKD.
| Neuropathic Symptoms | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | P | ||||||||||
| No | Yes | ||||||||||
| Cohort | Non-Nephropathy | Count | 106 | 59 | 165 | 0.63 | |||||
| % | 64.2% | 35.8% | 100.0% | ||||||||
| Nephropathy | Count | 52 | 33 | 85 | |||||||
| % | 61.2% | 38.8% | 100.0% | ||||||||
| Total | Count | 158 | 92 | 250 | |||||||
| % | 63.2% | 36.8% | 100.0% |
| VPT Abnormality Absent Present | VPT Abnormality | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | P | ||||||||||||
| Absent | Present | ||||||||||||
| Cohort | Non-Nephropathy | Count | 106 | 59 | 165 | 0.005 | |||||||
| % | 64.2% | 35.8% | 100.0% | ||||||||||
| Nephropathy | Count | 39 | 46 | 85 | |||||||||
| % | 45.9% | 54.1% | 100.0% | ||||||||||
| Total | Count | 145 | 105 | 250 | |||||||||
| % | 58.0% | 42.0% | 100.0% |
| H/O Foot Ulcer No Yes | Total | P | ||||
|---|---|---|---|---|---|---|
| Yes | ||||||
| Cohort | Non-Nephropathy | Count | 153 | 12 | 165 | <0.001 |
| % | 92.7% | 7.3% | 100.0% | |||
| Nephropathy | Count | 63 | 22 | 85 | ||
| % | 74.1% | 25.9% | 100.0% | |||
| Total | Count | 216 | 34 | 250 | ||
| % | 86.4% | 13.6% | 100.0% |
| Former Smoker | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | P | ||||||||||||
| No | Yes | ||||||||||||
| Cohort | Non-Nephropathy | Count | 136 | 29 | 165 | <0.001 | |||||||
| % | 82.4% | 17.6% | 100.0% | ||||||||||
| Nephropathy | Count | 45 | 40 | 85 | |||||||||
| % | 52.9% | 47.1% | 100.0% | ||||||||||
| Total | Count | 181 | 69 | 250 | |||||||||
| % | 72.4% | 27.6% | 100.0% |
| Current Smoker | P | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| No | Yes | Total | |||||||
| Cohort | Non-Nephropathy | Count | 123 | 42 | 165 | <0.001 | |||
| % | 74.5% | 25.5% | 100.0% | ||||||
| Nephropathy | Count | 36 | 49 | 85 | |||||
| % | 42.4% | 57.6% | 100.0% | ||||||
| Total | Count | 159 | 91 | 250 | |||||
| % | 63.6% | 36.4% | 100.0% |
Table 2G: Current smoking status.
| ED | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | P | ||||||||||||
| No | Yes | ||||||||||||
| Cohort | Non-Nephropathy | Count | 141 | 24 | 165 | <0.001 | |||||||
| % | 85.5% | 14.5% | 100.0% | ||||||||||
| Nephropathy | Count | 58 | 27 | 85 | |||||||||
| % | 68.2% | 31.8% | 100.0% | ||||||||||
| Total | Count | 199 | 51 | 250 | |||||||||
| % | 79.6% | 20.4% | 100.0% |
Discussion Type 2 diabetes mellitus (T2DM) is a growing epidemic world over, manifesting floridly with its macro vascular and micro vascular complications. Diabetic nephropathy is one of the micro vascular complications characterized by hypertension, a progressive increase in albuminuria, a high cardiovascular risk, and a relentless decline in GFR leading towards ESRD [5, 6, 7]. The pathogenic mechanisms underlying diabetic nephropathy involve generation of mitochondrial reactive PKC in a manner similar to reactive oxygen species (ROS) and accumulation of AGEs. Various epidemiologic studies have demonstrated that about 20-40% of diabetic subjects will develop proteinuria and progressive renal failure on an average of 15-20 years after the onset of diabetes. The prognosis of these patients is poor and without renal support therapy, the mean survival after the onset of clinical proteinuria is only 5 year [8, 9]. Many prospective observational studies have reported the initiation and progression of incipient nephropathy and predictors in type 1 diabetes patients [10, 11, 12]. The present study was designed to evaluate DKD in T2 DM in a subset of Indian population. Prevalence of diabetic kidney disease (DKD) in this study was 34%. Various epidemiology studies of type 2 diabetes patients showed that diabetic nephropathy prevalence ranges from 7.6% to 55% [13]. Various other Indian studies have reported the prevalence of diabetic nephropathy in type 2 diabetic subjects to be 5-9% [14]. However, this value is much less when compared with the prevalence of the same in Asian-Indians in the UK (22.3%) in a study conducted by Samanta et al. [15]. Evidence suggests that Asian ethnic group immigrants with type 2 diabetes had high incidence of end stage renal failure and a 40-fold increased risk for ESRD [16]. In the “Chennai Urban Rural Epidemiology Study,” the prevalence of overt nephropathy and micro-albuminuria was 2.2% and 26.9%, respectively, in the urban citizens with diabetes [17]. The prevalence being on the higher side in this study may be due to the study being conducted in a tertiary care referral hospital outdoor. Moderately increased albuminuria (formerly microalbuminuria) was commoner than markedly increased albuminuria (formerly macroalbuminuria) (81% vs. 19%) in this study. All subjects with microalbuminuria had a normal e GFR,whereas 44% of subjects with macroalbuminuria had a normal e GFR in the present study. 90% of DKD subjects in the present study were detected to have normal e GFR with albuminuria. Only nine patients (10%) had low eGFR. Subjects with low eGFR had markedly increased albuminuria. No patient with low eGFR but normoalbuminuria was found in this study.Several epidemiological studies have reported prevalence rates of microalbuminuria ranging from 7% to 42% [13, 14]. A cohort of type 2 diabetic patients reported by Mohan et al. [18] from India in the year 2000 showed a macroalbuminuria prevalence of 6.9%, and microalbuminuria of 2.5%.In the study by Vaishnava H et al. [19]. The prevalence of microalbuminuria in Indian patients has been reported to be around 37% in type 2 DM [19]. A study by Varghese et al. [20] has shown that the prevalence of microalbuminuria in Indian patients with type 2 DM is similar to that in the European population [20]. Islam et al. [21] have seen no difference in the prevalence of microalbuminuria among Indian, Malay, and Chinese patients, although urinary albumin excretion was higher in Indians [21]. The reported prevalence of microalbuminuria in India is 26.9 per cent among type 2 diabetes patients and the occurrence of proteinuria increases with duration of diabetes as reported by Schmitz A et al. [22] in their study in an urban south Indian population [22]. Prevalence of microalbuminuria and macroalbuminuria were 28% and 6% in their study. Studies conducted in neighboring Asian countries reported variability in the prevalence of microalbuminuria ranging from 14.2% in Iran to 36.3% in India. Recently, the MAP study had shown the alarming high prevalence of albuminuria. The highest prevalence of microalbuminuria was observed in Korea (56.5%) and the lowest in Pakistan (24.2%) [23]. In the United Kingdom Prospective Diabetes Study, the total prevalence of nephropathy was reported as 30.8%, which is lower than our results. In other European countries, the total prevalence was observed as 47% [23]. Compared with these studies and others, our study shows a higher prevalence. The large differences observed in the prevalence of nephropathy among different studies could be attributed to the differences in study design and methodologies adopted for defining the disease, setting, diagnostic criteria, methods for collection of urine, and its assessment of microalbuminuria and patient population. Many of the studies were clinic based, and this could have introduced a referral bias. One also cannot rule out the possibility of true ethnic differences in the prevalence of nephropathy due to decreased susceptibility to micro vascular disease in native Asian Indians. In support of this, an earlier study [24] had reported that the prevalence of diabetic retinopathy is lower in Indians compared with other ethnic groups.These findings, if confirmed by future studies, would be of great interest, as Asian Indians are known to have much higher rates of premature coronary artery disease compared with other ethnic groups [25]. Once overt nephropathy occurs without specific interventions, the glomerular filtration rate (GFR) gradually falls over a period of several years at a rate that is highly variable from individual to individual. In addition to its being the earlier manifestation of nephropathy, albuminuria is marker of greatly increased cardiovascular morbidity and mortality for patients with T2DM [26]. As a result, diabetes patients should be screened and monitored regularly for microalbuminuria to avoid the risk of diabetic nephropathy complications. In our study, the prevalence of DKD with low eGFR was only 3%. The various risk factors and that contribute to development of DKD include- ethnicity, glycemic status, genetic susceptibility hypertension, smoking, dyslipidaemia, retinopathy and obesity. Previous smaller studies of type 2 diabetic patients with nephropathy have, however, found conflicting results regarding the impact of hyperglycemia with some studies reporting an increased rate of decline in kidney function with poor metabolic control whereas other studies have not found that association [27, 28]. In the present study,patients with DKD had a lower HbA1c compared with non DKD cohort. This may be due to the inclusion of patients with low eGFR in the group,most of them being on insulin and a strict glycemic control and also the DKD cohort being more conscious about their prognosis and following a rigid lifestyle modification, as was evident during the one year followup. The DKD subjects also had a significantly higher DM duration, higher BMI, higher serum potassium levels, lower HDL-C level, higher triglyceride and LDL-C levels. Male sex, family history of DKD and past history of foot ulcer were significantly associated with DKD. The DKD cohort had significantly more erectile dysfunction, VPT abnormality and active foot ulcer, However hypertension, retinopathy, ECG and USG abnormality occurrence did not differ significantly between the two groups.It was observed that this subset of patients were extremely conscious about blood pressure control, sometimes the concern superceding the concern of glycemic control. It is becoming increasingly clear that anemia occurs at a high frequency early in the course of diabetic renal disease even before GFR is severely reduced. A causative role of anemia for progression of renal disease has been suggested in smaller interventional studies. Subjects with DKD in the present study had a significantly lower hemoglobin level than non DKD subjects, and most of DKD subjects had normal eGFR(89%) in this study. This may also explain the fact that HbA1c was significantly lower in the DKD group. In both type 1 and type 2 diabetes, smoking increases the risk of developing microalbuminuria and diabetic nephropathy. Both former and recent smoking status showed significant association with DKD compared to the non DKD group in the present study. Such an association has also been reported in other studies of type 2 diabetes patients with nephropathy [29, 30]. The probable limitation of this study was referral bias due to the study being conducted in a tertiary care centre.
However, this centre caters to a large geographic area and hence representative of a large section of population.
Conclusion
The prevalence of albuminuria is considerably high among diabetes subjects in this area. Prevalence of microalbuminuria and normal eGFR were much greater compared to macroalbuminuria and loweGFR respectively, which suggests a great scope of detecting these patients at the earliest stage of chronic kidney disease and improve their prognosis.Patients with DKD had a significantly higher DM duration, higher BMI, lower HbA1c, higher serum potassium, more dylipidemia and anemia. Malesex, smoking, family history of DKD, erectile dysfunction, neuropathy and foot ulcer were significantly associated with DKD. This study revealed various risk factors and associations of DKD in this geographical area, the knowledge of which might help us to formulate a holistic approach to fight against this dreaded micro vascular complication of diabetes.
References
-
Wild S, Roglic G, Green A, Sicree R, King H (2004) Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 27(5): 1047-1053.
-
Han-HenrickParving, Nish C, Gian CV, Carl EM (2002) Does microalbuminuria predict diabetic nephropathy? Diabetes Care 25(2): 406-407.
-
Young BA, Maynard C, Boyko EJ (2003) Racial differences in diabetic nephropathy, cardiovascular disease, and mortality in a national population of veterans. Diabetes Care 26(8): 2392-2399.
-
Volpe M (2008) Microalbuminuria screening in patients with hypertension: recommendations for clinical practice. Int J ClinPract 62(1): 97-108.
-
Dronavalli S, Duka I, Bakris GL (2008) The pathogenesis of diabetic nephropathy. Nat Clin Pract Endocrinol Metab 4(8): 444-452.
-
Soldatos G, Cooper ME (2008) Diabetic nephropathy: important pathophysiologic mechanisms. Diabetes Res Clin Pract 82: 75-79.
-
Kramer HJ, Nguyen QD, Curhan G, Hsu CY (2003) Renal insufficiency in the absence of albuminuria and retinopathy among adults with type 2 diabetes mellitus. JAMA 289(24): 3273-3277.
-
Thomas MC, Macisaac RJ, Jerums G, Andrew W, John M, et al. (2009) Nonalbuminuric renal impairment in type 2 diabetic patients and in the general population (National Evaluation of the Frequency of Renal Impairment Co-existing With NIDDM [NEFRON] 11). Diabetes Care 32(8): 1497-1502.
-
Johnson CA, Levey AS, Coresh J, Levin A, Lau J, et al. (2004) Clinical practice guidelines for chronic kidney disease in adults: part II. Glomerular filtration rate, proteinuria, and other markers. Am Fam Physician 70(6): 1091-1097.
-
Collins AJ, Foley RN, Chavers B, Gilbertson D, Herzog C, et al. (2011) United States Renal Data System 2011 Annual Data Report: Atlas of chronic kidney disease & end-stage renal disease in the United States. Am J Kidney Dis 59(1): 1-420.
-
Rossing P, Hougaard P, Parving HH (2002) Risk factors for development of incipient and overt diabetic nephropathy in type 1 diabetic patients: a 10-year prospective observational study. Diabetes Care 25(5): 859-864.
-
Shen FC, Chen CY, Su SC, Liu RT (2009) The Prevalence And Risk Factors Of Diabetic Nephropathy In Taiwanese Type 2 Diabetes - A Hospital Based Study. Acta Nephrologica 23: 2.
-
John L, Sundar Rao PSS, Kanagasabapathy AS (1991) Prevalence of diabetic nephropathy in non-insulin dependent diabetics. Indian Journal Med Res 94: 24- 29.
-
Ramachandran A, Snehalatha C, Satyavani K, Latha E, Sasikala R, et al. (1999) Prevalence of vascular complications and their risk factors in type 2 diabetes. J Assoc Phys India 47(12): 1152-1156.
-
Samanta A, Burden AC, Jagger CA (1991) Comparison of the clinical features and vascular complications of diabetes between migrant Asian and Caucasians in Leicester, UK. Diabetes Res ClinPract 14(3): 205-213.
-
Burden AC, McNally PG, Feehally J, Walls J (1992) Increased incidence of end-stage renal failure secondary to diabetes mellitus in Asian ethnic groups in United Kingdom. Diabet Med 9(7): 641-645.
-
Unnikrishnan R, Rema M, Pradeepa R, Deepa M (2007) Prevalenceand risk factors of diabetic nephropathy in an urban south Indian population: the Chennai Urban Rural Epidemiology Study (CURES 45). Diabetes Care 30(8): 2019-2024.
-
Mohan V, Meera R, Premalatha G, R Deepa, P Miranda, et al. (2000) Frequency of proteinuria in type 2 diabetes mellitus seen at a diabetes centre in southern India. Postgrad Med J 76(899): 569-573.
-
Vaishnava H, Dixit NS, Soloman SK (1964) Study of diabetes in South India. J Assoc Phys India 12: 255- 276.
-
Varghese A, Deepa R, Rema M, Mohan V (2001) Prevalence of microalbuminuria in type 2 diabetes mellitus at a diabetes centre in southern India. Postgrad Med J 77(908): 399-402.
-
Islam N, Kazmi F, Chusney GD, Mattock MB, Zaini A, et al. (1998) Ethnic differences in correlates of microalbuminuria in NIDDM. The role of the acute- phase response. Diabetes 21(3): 385-388.
-
Schmitz A, Vaeth M. Microalbuminuria: a major risk factor in non-insulin-dependent diabetes. A 10-year follow-up study of 503 patients. Diabet Med 5(2): 126-134.
-
Alrawahi AH, Rizvi SG, Al-Riyami D, Al-Anqoodi Z (2012) Prevalence and Risk Factors of Diabetic Nephropathy in Omani Type 2 Diabetics in Al- Dakhiliyah Region Oman Med J 27(3): 212-216.
-
Ramachandran A, Snehalatha C, Satyavani K (1999) Prevalence of vascular complications and their risk factors in type 2 diabetes. J Assoc Phys India 47: 1152-1156.
-
Deckert T, Yokoyama H, Mathiesen E, Rønn B, Jensen T, et al. (1996) Feldt-Rasmussen B. Cohort study of predictive value of urinary albumin excretion for atherosclerotic vascular disease in patients with insulin dependent diabetes. BMJ 312(7035): 871-874.
-
Trevisan R, Vedovato M, Mazzon C, Coracina A, Iori E, et al. (2002) Concomitance of Diabetic Retinopathy and Proteinuria Accelerates the Rate of Decline of Kidney Function in Type 2 Diabetic Patients. Diabetes Care 25(11): 2026-2031.
-
Fried LF, Orchard TJ, Kasiske BL (2001) Effect of lipid reduction on the progressionof renal disease: A meta- analysis. Kidney Int 59(1): 260-269.
-
Chuahirun T, Simoni J, Hudson C, Seipel T, Khanna A, et al. (2004) Cigarette smoking exacerbatesand its cessation ameliorates renal injury in type 2 diabetes. Am J Med Sci 327(2): 57-67.
-
Bello AK, Hemmelgarn B, Lloyd A, James MT, Manns BJ, et al. (2011) Associations among estimated glomerular filtration rate, proteinuria, and adverse cardiovascular outcomes. Clin J Am Soc Nephrol 6(6): 1418-1426.
-
Tonelli M, Klarenbach SW, Lloyd AM, Matthew TJ, Aminu KB et al. (2011) Higher estimated glomerular filtration rates may be associated with increased risk of adverse outcomes, especially with concomitant proteinuria. Kidney Int 80(12): 1306- 1314.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty