Lymphadenopathy in Autoimmune Thyroiditis: Paratracheal Lymph Nodes are Indeed Crucial
<p>Cervical lymphadenopathy is common in patients with autoimmune thyroiditis and supposed to be pathognomic for the disease if found in the paratracheal compartment (Robbins level VI). The aim of this prospective study is the extensive characterization of all cervical lymph node compartments in order to determine the significance of sonographic visible cervical lymphnodes in autoimmune thyroiditis. The study comprises 32 consecutive autoimmune thyroiditis patients and 32 controls without any thyroid pathologies. All patients underwent high resolution ultrasound and all visible lymph nodes were evaluated in all cervical levels by size, volume, S/L-ratio, appearance, vascularity and structural changes. In total, 84 lymph nodes in Robbins level VI were detected in the group of patients with autoimmune thyroiditis whereas the control group showed 2 positive lymph nodes. Lymph nodes in Robbins level VI were significantly smaller compared to lymph nodes in other cervical compartments with 54% of lymph nodes</p>
Introduction
An involvement of cervical lymph nodes in autoimmune thyroiditis (AIT) has been detected by some studies so far [1, 2, 3, 4, 5]. However, the involvement of paratracheal lymph nodes (Robbins level VI) is controversial. Studies of Brancato et al. and Jones et al. gave a systematic description of the sonographic pattern of cervical lymph nodes in AIT. They detected an increased number of hyperplastic lymph nodes in AIT- patients in Robbins level I-IV [1, 2, 3, 4, 5]. Those findings are diametrical to previous studies, including a pilot study of our own group [3] and prompted us to critical review the results of Brancato et al. Therefore, we collected new, unbiased data of the prevalence of all visible LN in AIT- patients compared with healthy controls in a prospective setting. Aim of this study was the evaluation of every visible LN in all cervical levels (Robbins level I-VI) of the neck without an arbitrary definition of a ‘hyperplastic’ LN. Study populations were evaluated prospectively, after a careful estimation of the sample size, excluding patients with infection and tumors that are known to be associated with cervical LN involvement.
Material and Methods
We analyzed a total of 64 patients. Two groups were prospectively defined as follows: Group one included 32 patients with autoimmune thyroiditis (AIT). AIT was defined as typical ultrasound findings (hypoechoic thyroid, septation, lobulation) plus elevated TSH, already proven substituted hypothyroidism or elevated thyroid antibodies. The second group included patients without any thyroidal pathology confirmed by ultrasound. Sample size was determined with the help of the department of medical statistics of the Georg-August University Gottingen based on our earlier study [3]. Excluded were all patients with other diseases that involve or influence cervical LN like influenza, diseases that required radioiodine treatment in the past, radiation of the head/neck area, malignant thyroid or otolaryngeal tumors, infectious dental diseases, current surgery of the head/neck area, lymphomas, toxoplasmosis, HIV or current herpes simplex. All patients underwent ultrasound of the neck with a high resolution Siemens ACUSON Antares Ultrasound Scanner using a 5-13MHz transducer (Siemens, Erlangen, Germany). Sonographic pattern of the thyroid was examined and all cervical LN compartments (RLI-VI) were ascertained. Visible LN were extensively assessed by size, volume, short-axis/long-axis ratio, shape (oval or rounded), vascularity and presence of a hilum or structural changes like calcification or cystic degeneration. Cervical LN were divided into four compartments adapted from Robbins, et al. [6]. Due to the difficulty separating RL II, III and VI from each other in ultrasound, these compartments were examined together. For further analyses the appearance of thyroid tissue in ultrasound was rated as follows: 1= slightly hypoechoic and/or micro-nodular pattern; 2= hypoechoic septated thyroid and/or micro-nodularity; 3= deeply hypoechoic, lobulated thyroid. Blood levels of TSH, TSH-receptor antibodies (TRAB), anti-TPO-antibodies (TPOAb) and anti-Thyroglobulin- antibodies (TgAb) were analyzed using chemiluminescence immunometric assays (Immulite, Siemens Medical Solutions, Los Angeles, CA; USA) using the following reference values: TSH= 0.27-4.2 µIU/ml, TPOAb= 0-35 IU/ml, TgAb= 0-40 IU/ml, TRAB= 0-1,75 IU/ml. As the sonographic pattern is decisive in the evaluation of thyroid diseases and patients with normal ultrasound show a normal serology in more than 90% of cases [7, 8], no blood work was performed in the control group. Mean values and standard deviation were calculated for all variables. Differences between groups were analyzed by the Kruskal-Walis, t-test or Mann-Whitney test. A p-value <0.05 was considered significant. Linear regression and the coefficient of determination (r²) were used in order to correlate TPO Ab-values with the amount of paratracheal LN and ultrasound findings. Graph Pad Prism 6 and Microsoft Excel were used for statistical analysis.
Results
We examined a total of 64 patients (48 females and 16 males aged 21 to 78 (mean 36) in a prospective setting. Patients were divided into two groups as follows: 32 controls without any thyroid pathologies and 32 patients with AIT. Thyroids of all individuals of the control group showed regular echogenicity, size and perfusion. Thyroid nodules were not present in any of these patients. Thyroid volume ranged between 3,8 and 17,9 ml with a median of 8,7 ml. All patients of the AIT group showed a hypoechoic thyroid in ultrasound. Thyroid volume ranged between 3,2 and 14,2 ml (mean 8 ml). 12 patients showed a micronodular hypoechoic sonographic pattern. 6 patients had thyroid nodules >1 cm (a total of 13 nodules). All nodules showed a benign appearance. 20 of 32 patients had positive TPOAb, 2 patients showed positive TgAb and one patient had elevated TRAB. TSH was elevated in 7 patients and 13 patients with known hypothyroidism were already substituted with levothyroxine. Only a slight correlation between TPOAb values and thyroid ultrasound findings could be observed (r²=0.22). Table 1 shows the number of positive LN in all cervical compartments for each group. There were no significant differences in the amount of cervical LN between patients with and patients without AIT in RL I-IV. The amount of LN in RLV was significantly higher in the control group (p=0.0002) AIT patients showed a significantly higher amount of visible LN in RLVI compared to the healthy control group (p=0.0183). LN were significantly smaller in RLVI compared to RLI-V (p=0.0135) and in 54% of LN in RLVI the longitudinal diameter was below 5 mm.
| Control Total number of LN (mean + standard aviation) | AIT Total number of LN (mean + standard aviation) | Kruska-Wallis | |
| Total | 894 (27.9±8.95) | 732 (22.88±12.44) | ns |
| RL I | 41 (2.05±1.12) | 35 (2.19±1.47) | ns |
| RL II-IV | 254 (7.94±4.59) | 232 (7.25±5.05) | ns |
| RL V | 596 (18.63±6.98) | 368 (11.5±7.06) | 0.0002 |
| RL VI | 2 (1±0) | 83 (3.074±2.43) | 0.0183 |
Table 1: Number of LN in all cervical levels in AIT-patients compared to the control group.
AIT-patients showed a significantly higher amount of visible LN in RLVI compared to all other cervical compartments. LN= lymph nodes. Characteristics of cervical LN are shown in Table 2. Long-axis and short-axis diameter did not show significant differences between both groups in RL III-VI whereas short-axis diameter was higher in RLI of AIT patients. Calcification or intranodal cystic degeneration was not observed in any LN.
There was no correlation between anti-TPO values and the amount of visible LN (r²=0.018).
| Control | AIT | Kruska-Wallis | ||||||
| RL I | ||||||||
| Long | 7.03 ± 2.61 | 7,6 ± 2,67 | ns | |||||
| Short | 3.55 ±1.21 | 4,28 ± 1,87 | 0,0366 | |||||
| S/L | 2.33 ± 1.86 | 0,6 ± 0,25 | 0,001 | |||||
| RL II-IV | ||||||||
| Long | 6.7 ± 3.25 | 7.06 ± 2.95 | ns | |||||
| Short | 2.97 ± 1.33 | 3.24 ±1.53 | ns | |||||
| S/L | 0.48 ± 0.2 | 0.48 ± 0.21 | ns | |||||
| RL V | ||||||||
| Long | 5.55 ± 1.95 | 6.19 ± 2.34 | ns | |||||
| Short | 2.19 ± 1.01 | 2.41 ± 1.09 | ns | |||||
| S/L | 1.71 ± 0.41 | 0.42 ± 0.21 | ns | |||||
| RL VI | ||||||||
| Long | 4.65 ± 1.35 | 4.96 ± 1.63 | ns | |||||
| Short | 2.1 ± 0.49 | 2.93 ± 1.31 | ns | |||||
| S/L | 0.54 ± 0.29 | 0.64 ± 0.38 | ns |
Table 2: Sonographic characterization of visible LN.
Discussion
AIT is one of the most common autoimmune diseases and the most common cause of hypothyroidism [9, 10]. T- cell mediated diffuse lymphocyte infiltration leads to destruction and functional impairment of thyroid tissue [9]. Ultrasound and serology of elevated antibodies against thyroid peroxidase and/or thyroglobulin are the diagnostic basis whereas ultrasound typically displays a diffuse hypoechoic pattern of the thyroid parenchyma [9]. It is presumed that cervical lymphadenopathy (LAP) is related to the autoimmune process in AIT. An increased prevalence of enlarged cervical LN was described in earlier studies [1, 2, 3, 4, 5] and LAP in Robbins Level VI seems to be predictive for AIT in an early stage [2, 11, 12]. However, there is no prospective randomized study regarding the prevalence of cervical LAP in AIT compared to healthy subjects. The aim of our prospective study was the extensive evaluation of LN in all cervical levels in order to determine the prevalence and predictive value of LAP, especially in RLVI. We analyzed all visible cervical LN and compared AIT patients with healthy controls in each Robbins level. This is the first study analyzing LN in a prospective setting in all cervical compartments without using arbitrary cut-offs offs in order to minimize any bias in our data. Our results showed a significantly higher number of LN in RLVI of AIT patients. Only 2 LN in RLVI were detected in controls without thyroid diseases confirming visible LN in RLVI are a rare finding in healthy individuals. However, AIT patients showed 84 LN in RLVI (mean 3,1/patient) indicating an essential involvement of these paratracheal LN in AIT. Therefore, we propose to include the sonographic examination of paratracheal LN in the clinical workup of patients with suggested AIT. Especially in doubtful cases or early stages of AIT the additional information can help to differentiate patients with AIT from patients without thyroid disorder in order to minimize false negative results. Furthermore, positive LN in RLVI are known to be smaller compared to other cervical LN compartments. Our results confirm those findings as mean long–axis diameter of RLVI LN were <5mm.
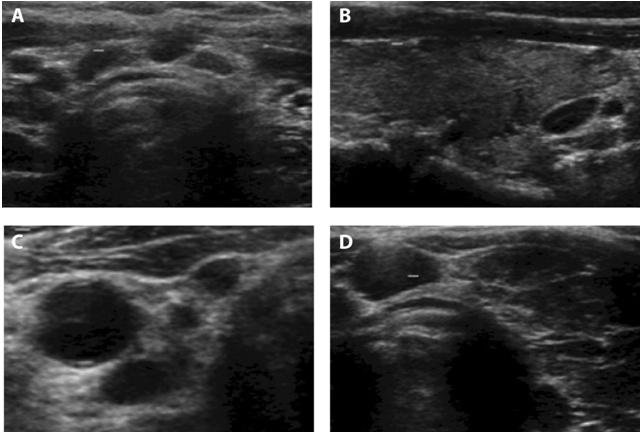
Serres-Créixams et al. first described an involvement of paratracheal LN in AIT and suggested a connection to the inflammatory process. The study enclosed 309 consecutive patients in two groups (AIT and controls without thyroid disease) reviewed by one radiologist in a retrospective setting. Presence of any detectable LN in RLVI in ultrasound was documented. Data showed a significantly higher number and size of LN in RLVI in the AIT group. Results were confirmed by a study of Sahlmann et al. that included prospective data of 98 patients evaluating all cervical LN compartments. Cut-off values were used in order to determine compartment positivity. An overall cut-off of 5mm in the transverse diameter was used and RL I-III and V were considered positive if more than five LN were present whereas RL VI was considered positive if at least one LN was detectable. Next to a higher number of LN in RL VI, AIT patients also showed a significant higher amount of LN in RL II-IV in that study. Several other studies selectively focused on changes in paratracheal LN of AIT patients. Akbaba et al. examined LN in RLVI in 165 AIT patients compared to 32 healthy subjects retrospectively and presented a significantly higher ratio and volume of RL VI-LN as well as a positive correlation between the number of LN and TPO levels. Furthermore, the group showed remaining LAP in the AIT group in a five-year follow up. Another study of Kosiak, et al. evaluated RLVI-LN in 98 children with Hashimoto’s thyroiditis (HT) prospectively. In 98% of the patients in the HT group at least two enlarged LN were present in RLVI. A recent prospective study of Ormeci et al. compared characteristics of a Delphian LN (a small compartment of RL VI; figure 1A- 1D) between 126 AIT patients in different stages of the diseases as well as controls and confirmed previous findings. Both, number and size of Delphian LN were highly correlated with the progress of AIT. Authors suggested including the evaluation of cervical LN in the diagnostic process in order to prevent missing a AIT- diagnosis.
In contrast to our present results and results of the above described studies, the work of Brancato et al. did not show any differences of LN in RLVI between AIT patients and healthy controls in a retrospective setting. Differences were only detected in RL II, III and IV. That study used an arbitrary cut-off of the long-axis diameter of 10mm, which might explain why LN in RLVI was missed [1]. Another study that did not detect LN in RLVI was presented by Jones, et al. [5]. The group detected a larger amount of LN in RLI and III in patients with HT compared to patients with non-toxic goiter. LN-sizes were similar between both groups in all cervical levels. That study only detected 0,03 (HT) and 0,02 (control) mean LN in RLVI which implicates either an arbitrary cut-off in LN diameters or a possible bias due to the retrospective setting as RLVI might not have been evaluated routinely and can easily be missed in clinical routine. As LN in RLVI often show certain sonographic malignancy criteria as rounded shapes and facet formation a possible malignancy of those LN has to be discussed. In an earlier study we therefore performed an extensive workup of patients with AIT and distinct LAP in RLVI including clonal analysis of those paratracheal LN. Results invariably showed benign etiology pointing out that enlarged LN in RLVI are possibly related to the autoimmune process [13]. Anyhow, lymphomatous LN may show a similar sonographic pattern. An earlier case report of our group addressed this issue presenting one patient with AIT and extensive LAP that exceeded from RL
II-VI to the retroclavicular compartment. Further diagnostics revealed a follicular B-cell Non-Hodgkin lymphoma [14]. Therefore, in cases with extensive LAP exceeding to the retroclavicular or mediastinal compartments it is suspicious for malignancy and further diagnostics are crucial.
Conclusion
LAP in RLVI is indeed pathognomic for AIT and can be used as a predictor for AIT in early stages.
References
-
Brancato D, Citarrella R, Richiusa P, Amato MC, Vetro C, et al. (2013) Neck lymph nodes in chronic autoimmune thyroiditis: the sonographic pattern. Thyroid 23(2): 173-177.
-
GA (2014) Changes in the Charactersitics of Paratracheal Lymph Nodes in Patients with Chronic Autoimmune Thyroiditis for Five Years Follow-up. Endocrine Society’s 96thAnnual Meeting and Expo. Chicago, USA.
-
Sahlmann CO, Meller J, Siggelkow H, Bouter C, Meller B, et al. (2012) Patients with autoimmune thyroiditis. Prevalence of benign lymphadenopathy. Nuklearmedizin 51(6): 223-227.
-
Serres Creixams X, Castells Fuste I, Pruna Comella X, Yetano Laguna V, Garriga Farriol V, et al. (2008) Paratracheal lymph nodes: a new sonographic finding in autoimmune thyroiditis. J Clin Ultrasound 36(7): 418-421.
-
Jones MR, Mohamed H, Catlin J, April D, Al Qurayshi Z, et al. (2015) The presentation of lymph nodes in Hashimoto's thyroiditis on ultrasound. Gland Surg 4(4): 301-306.
-
Robbins KT, Clayman G, Levine PA (2002) Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Arch Otolaryngol Head Neck Surg 128(7): 751-758.
-
Tam AA, Kaya C, Ucler R, Dirikoc A, Ersoy R, et al. (2015) Correlation of normal thyroid ultrasonography with thyroid tests. Quant Imaging Med Surg 5(4): 569-574.
-
Trimboli P, Rossi F, Thorel F (2012) One in five subjects with normal thyroid ultrasonography has altered thyroid tests. Endocr J 59(2): 137-143.
-
Chistiakov DA (2005) Immunogenetics of Hashimoto's thyroiditis. J Autoimmune Dis 2(1): 1.
-
Pearce EN, Farwell AP, Braverman LE (2003) Thyroiditis. N Engl J Med 348(26): 2646-2655.
-
Kosiak W, Piskunowicz M, Swieton D, Batko T, Kaszubowski M, et al. (2015) An additional ultrasonographic sign of Hashimoto's lymphocytic thyroiditis in children. J Ultrason 15(63): 349-357.
-
Ormeci T, Colakogullari M, Orhan I (2016) Importance of Delphian Lymph Node Evaluation in Autoimmune Thyroiditis: Fact or Fiction? Pol J Radiol 81: 72-79.
-
CB (2016) Clonal analysis of marked paratracheal lymphadenopathy in autoimmune thyroiditis invariably shows benign etiology. Deutsche Gesellschaft Nuklearmedizin, Dresden, Germany.
-
Bouter CMB, Meller J, Sahlmann CO (2015) What makes Lymphadenopathy in Patients with Autoimmune Thyroiditis Suspicious for Malignancy? Exp Clin Endocrinol Diabetes Rep.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty