Trans Oral Endoscopic Thyroidectomy Vestibular Approach (TOETVA): A Case Report as a New Procedure in Iraq
<p>Introduction: The transoral endoscopic thyroidectomy vestibular approach; Is a new pioneering procedure, natural orifice surgery, truly scar free and involves minimal dissection, thus resulting in excellent cosmetic results and decreased post-operative complications. Case Report: A 25-year-old female presented with a benign multinodular goiter 2 years duration. She requested a surgery that would leave her with a minimal or no scar. She was scheduled to undergo transoral endoscopic thyroidectomy vestibular approach. Results: The operative time was (150 minutes), the patient was discharged from hospital on the second postoperative day, there were no intratoperative complications or mortality and the only postoperative complication that reported during this study was the mild seroma and swelling in the anterior aspect of the neck which resolved completely within two weeks. Conclusion: The transoral endoscopic thyroidectomy vestibular approach (TOETVA) is a safe, feasible and easy to performed procedure when the patient selected properly and the operating surgeon has a good experience in laparoscopic surgery and in conventional open thyroidectomy. The long operative time of this approach will decrease with experience.</p>
Introduction
Conventional thyroidectomy; remain the gold standard surgical treatment for thyroid diseases, but the incisional scar in the anterior aspect of the neck due to this approach cannot be avoided and may results in a permanent cosmetic defect [1].
Endoscopic neck surgery has been introduced since 1996 to avoid or to minimize the incisional scar in the neck [2]. In general there are two endoscopic thyroidectomy approaches; cervical and extra-cervical approaches, the cervical approach, although it is consider as minimally invasive technique but it still leave significant multiples small scar in the anterior aspect of the neck, the most commonly applied extra-cervical approaches are the trans-axillary and trans-areolar approach, although these approaches were successful in providing patients with minimal scar that could be hidden but they involved maximal dissection due to the absence of natural anatomic planes and the long distance between point of entry and the target organ which increase the duration of surgery and postoperative pain and complications, for that reasons these approaches not widely accepted as minimally invasive procedures [1]. On the other hand, the transoral endoscopic thyroidectomy vestibular approach (TOETVA ); the new pioneering procedure is a natural orifice surgery, truly scar free and involves minimal dissection, thus resulting in excellent cosmetic results and decreased post- operative complications [3]. In this case report, we describe the first Trans Oral Endoscopic Thyroidectomy Vestibular Approach (TOETVA) performed in IRAQ.
Case Report
A 25-year-old female presented with complaints of a swelling over the anterior part of her neck for the past 2 years. She had no complaints of pain or compressive symptoms. Examination revealed a swelling over the anterior part of the neck that moved with deglutition, firm in consistency. Ultrasound neck done revealed a mild to moderate enlargement of both thyroid lobes and isthmus with multiple small cystic nodules. Thyroid function test was normal. FNAC showed features suggestive of a benign colloid goiter. She requested a surgery that would leave her with a minimal or no scar. In view of the patient’s age, good general health and the size of the swelling, she was scheduled to undergo transoral endoscopic thyroidectomy vestibular approach.
Operative Technique
Pre-Operative Preparation
The patient was asked to gargle with Chlorhexidine mouth wash three times / day and receive oral Amoxicillin tab. 500mgthree times / day and Metronidazol tab. 500mg three times / day for 3 days before surgery as prophylactic antibiotic, after that the patient was admitted to the Al-Shiffa general hospital/ Basrah/ Iraq on 6th of August 2017, one day before surgery for routine investigations and preparation for general anesthesia.
Procedure
During induction of general anesthesia with endotracheal intubation through the mouth, the patient was receive injectable IV antibiotic inform of Amoxicillin 1g and Metronidazole 500mg after that the patient was placed in supine position with her neck extended using a sand bag placed between her shoulder, the endoscopic monitor set up behind the patient feet, the surgeon stand behind the patient head, the camera assistant stand near the left shoulder and the nurse on the right side of the patient. The oral cavity was washed with saline and Betadine. After locating the central region of the oral cavity and the vestibular region, a 10-mm transverse incision was performed in midline of the vestibule and extended in depth up to the mandible symphysis (Figure1). Using Veres needle, subplastimalhydro dissection with approximately 20cc of Normal Saline with Adrenaline (500cc Normal Saline + 1cc Adrenaline) was performed in 3 axes (central, right and left) (Figure 2). After that blunt dissection of the subplastimal plane with blunt dilator was performed in the same 3 axes of hydro dissection (Figure 3). A 10mm central trocar for camera was placed through the vestibular incision and insufflations to 5-6 mmHg with CO2 (Figure 4). Two additional 5 mm trocar were placed under direct vision through two 5mm vertical incisions in both most lateral aspect of the vestibule at the level of the inferior molars, in order to prevent injury of the mental nerve (Figure 5).




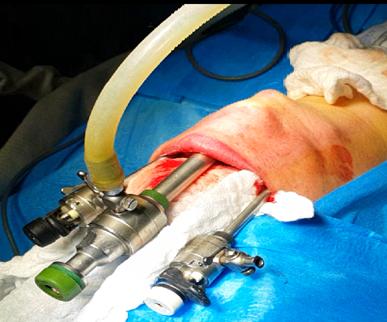
Figure 5: Two additional 5 mm trocar were placed under direct vision through two 5mm vertical incisions in both most lateral aspect of the vestibule at the level of the inferior molars, in order to prevent injury of the mental nerve. The sub-platyssmal plane was entered and dissected with ultrasonic energy device (Sonicbeat Olympus). The deep fascia was opened in the midline and strap muscles retracted with hanging sutures pass through the skin. The isthmus of the thyroid gland was identified and divided. The superior and inferior pedicles on the right side were identified and divided by ultrasonic energy device. Recurrent laryngeal nerve and parathyroid glands were identified and preserved. Subtotal excision of the right thyroid lobe with secured hemostasis was done. The right lobe was brought out through the oral cavity using an endobag. The same procedure was repeated on left thyroid lobe. Redivac drain was inserted through the skin to drain the surgical field. The deep fascia was closed using absorbable sutures and the vestibular port sites were closed in 2 layers using absorbable sutures. The operative time was (150 minutes); recorded from the beginning of vestibular incisions until complete closure of these wounds. No intraoperative complications were reported during this procedure. After recovery from general anesthesia, the patient transmitted to the surgical ward for follow-up. Injectable antibiotic was continued until the patient discharge from hospital. Oral diet was started on first postoperative day. The drain was removed on the first postoperative day containing only few cc of blood stain serous fluid. The patient was discharge from the hospital on the second postoperative day with no complications and given instructions to be continuing on oral antibiotic and mouth wash and to be re-examining at the end of first postoperative week, 2 weeks and 4 weeks.
Discussion
Transoral endoscopic neck surgery was first described as an experimental approach in 2008 by Witzel [4]. In 2012, Nakajo published their results of Trans-Oral Video- Assisted Neck Surgery (TOVANS) performed successfully on live patients [5]. In 2016 Anuwong A, from Thailand, published the first largest cohort of 60 patients had been operated with TransOral Endoscopic Thyroidectomy Vestibular approach (TOETVA), during this study; Dr. Anuwong A, refined the procedure by changing the positions of the two lateral vestibular wounds for working 5mm ports to a positions that more high and lateral in the vestibule near the angle of the mouth to avoid mental nerve injury which is the most specific complication of this approach, finally he concluded that this approach is safe and feasible in selected cases [3]. Recently, in 2017 Anuwong A published the outcome of the 425 patients who underwent TOETVA in comparison to the conventional open thyroidectomy and they concluded that TOETVA can be performed safely while avoiding any skin incision [6]. In addition, TOETVA is associated with longer operating time and less postoperative pain compared with Open Thyroidectomy and has outcome and complication rates similar to those of Open Thyroidectomy. In our case report; we follow the step by step procedure described by Dr. Anuwong A and the only complications that reported was the mild seroma in the lower part of the neck and mild swelling in the chin and submental area that treated conservatively and resolved completely at the end of the second postoperative week. The vestibular wounds completely healed within 1 week and the overall cosmotic results were perfect, Figure 6 shows patient neck before surgery, Figures 7 and 8 shows the patients neck and the vestibule of the mouth in the 2nd postoperative week.



Conclusion
The transoral endoscopic thyroidectomy vestibular approach (TOETVA) is a safe, feasible and easy to performed procedure when the patient selected properly and the operating surgeon has a good experience in laparoscopic surgery and in conventional open thyroidectomy. The long operative time of this approach will decrease with experience.
References
-
Tan CT, Cheah WK, Delbridge L (2008) “Scarless” (in the neck) endoscopic thyroidectomy (SET): an evidence-based review of published techniques. World J Surg 32(7): 1349-1357.
-
Gagner M (1996) Endoscopic subtotal parathyroidectomy in patients with primary hyperparathyroidism. Br J Surg 83(6): 863-875.
-
Anuwong A (2016) Transoral Endoscopic Thyroidectomy Vestibular Approach: A Series of the First 60 Human Cases. World J Surg 40(3): 491-497.
-
Witzel K, von Rahden BH, Kaminski C, Stein HJ (2008) Transoral access for endoscopic thyroid resection. Surg Endosc 22(8): 1871-1875.
-
Nakajo A, Arima H, Hirata M, Mizoguchi T, Kijima Y, et al. (2013) Trans-Oral Video-Assisted Neck Surgery (TOVANS). A new transoral technique of endoscopic thyroidectomy with gasless premandible approach. Surg Endosc 27(4): 1105-1110.
-
Anuwong A, Ketwong K, Jitpratoom P, Sasanakietkul T, Duh QY (2017) Safety and Outcomes of the Transoral Endoscopic Thyroidectomy Vestibular Approach. JAMA Surg.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty