Intra-thyroid Metastasis Revealing Bronchial Cancer
Thyroid metastases are rare. They may exceptionally reveal the primary cancer. Several hypotheses have been proposed to explain the low rate of thyroid metastases. The diagnosis is sometimes difficult to establish because the lesions are most often asymptomatic. Ultrasound and scanner are not specific. Histological examination and immune histochemical analysis is the key to diagnosis. Curative management depends on the histological type and the resect ability of the primary tumor. We report the case of a patient who presented with cervical swelling associated with dysphonia; clinical examination found a thyroid nodule confirmed by cervical ultrasound associated with a forearm mass. The patient underwent a left isthmolobectomy and then a right totalization. Histological examination was in favor of an intra-thyroid metastasis of an adenocarcinoma of pulmonary origin. The extension work-up showed pulmonary nodules and bone metastases. The patient underwent chemotherapy with good progression. Finally, the diagnosis of thyroid metastases must always be evoked in front of a swelling of the thyroid gland especially in the presence of a history of neoplasia.
Introduction
Thyroid metastases are rare. They most often appear during the follow-up of a treated patient but can exceptionally be revealing of the primary cancer. This situation has been rarely reported in the literature.
We report the case of a patient with bronchial cancer revealed by an intra-thyroid metastasis.
Observation
This is an 83-year-old patient, chronic smoker, who presented with left cervical swelling associated with dysphonia. Clinical examination found a hard, well-limited thyroid nodule in the left lobe, associated with a mass in the right forearm that was hard with irregular contours and painful on palpation. The rest of the clinical examination was unremarkable. The biological work-up did not reveal any dysthyroidism. A thyroid ultrasound showed a large left thyroid nodule slightly plunging into the retroclavicular region and classified as EU-TIRADS 4. A left isthmolobectomy was performed. The anatomopathological examination of the surgical specimen was in favour of a moderately differentiated adenocarcinoma, hence the right totalization fifteen days later. The final histological examination showed an intra- thyroid metastasis of an adenocarcinoma of pulmonary origin. The immunohistochemical complement affirmed the pulmonary origin with negative anti-thyroglobulin antibodies, positive anti-CK7 antibodies, negative anti-CK20 antibodies, positive anti-TTF1 antibodies, and positive anti- NAPSIN A antibodies.
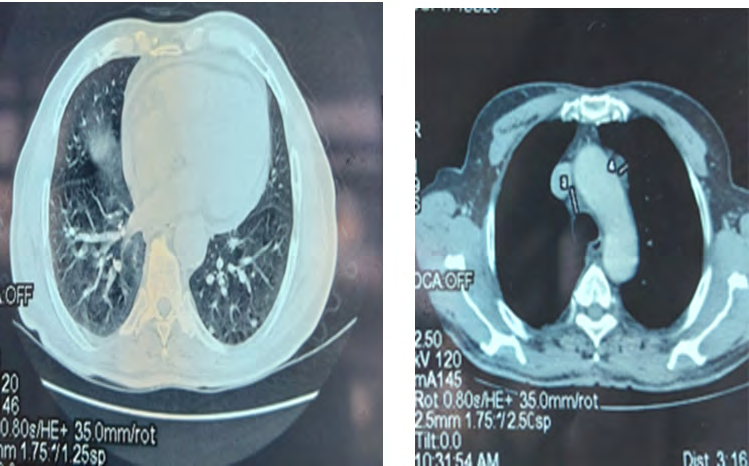
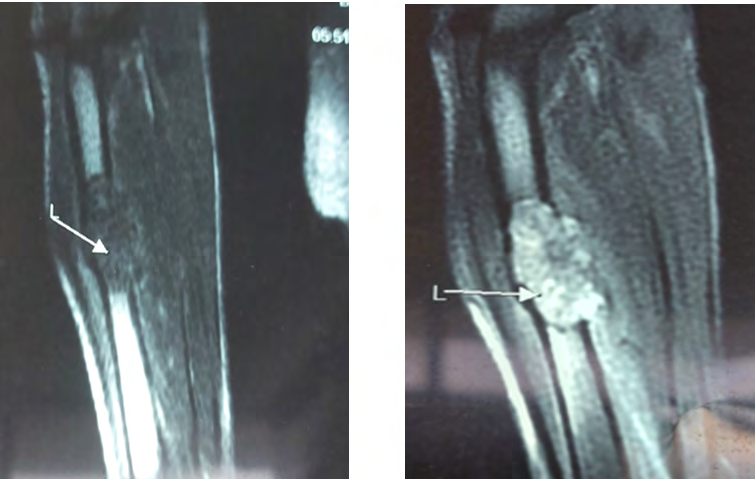
A cervico-thoraco-abdomino-pelvic CT scan found bilateral pulmonary nodules, the largest of which was apical on the left with a long axis of 15mm, associated with mediastinal adenopathy (Figure 1). An MRI of the right forearm showed an aspect in favour of a secondary location (Figure 2). After the various investigations, the diagnosis of metastatic pulmonary adenocarcinoma was retained, hence the indication for adjuvant chemotherapy with a good evolution.
Discussion
Thyroid metastases rare, accounting for 4% of thyroid neoplastic pathology [1]. In a study by Battistella E, et al. which retrospectively analyzed all patients who underwent thyroidectomy, only 9 cases out of more than 5,000 had metastases in the thyroid gland. The most frequent primary tumor was the kidney, followed by the lung and then the breast [2]. In our case, the primary tumor was of pulmonary origin.
Willis proposed two hypotheses to explain the low prevalence of thyroid metastases: the rapid arterial flow through the thyroid did not allow the adhesion of malignant cells and the high oxygen saturation and iodine concentration of the thyroid gland inhibited the growth of malignant cells [3].
A number of studies argue that multi-nodular goitre or other pathological conditions of the thyroid could induce implantation of neoplastic cells from other organs [4, 5]. If Willis’ hypotheses are correct, pathological thyroid glands with reduced blood flow and lower iodine concentrations should be more susceptible to metastasis [3]. In a series by Hefess and al, 42% of patients with thyroid metastases of extrathyroidal origin occur in the setting of thyroiditis or adenomas [6].
Thyroid metastases may be synchronous or metachronous with the primary disease and may in rare cases reveal the primary cancer [7], as was the case for our patient. The diagnosis of thyroid metastases is sometimes difficult to establish because the lesions are usually asymptomatic and may develop in a goitre simulating a primary tumour. In the literature, most patients presented with clinical symptoms such as a thyroid nodule, signs of compression with dysphagia, dysphonia, hoarseness and cough [8]. In our patient, the clinical symptomatology was dominated by a thyroid nodule associated with signs of compression.
Ultrasound is not specific. It may show localized hypoechoic lesions, sometimes calcified, more or less suspicious, or a hyperechoic appearance related to inflammatory or necrotic changes. The CT scan can visualize hypodense lesions, often heterogeneous, with moderate enhancement after injection of the contrast product. PET scans are not a preferred examination for exploring thyroid lesions, but may be useful in the search for the primary tumor and in the assessment of extension [9]. Histological examination and immunohistochemical analysis of the biopsy or surgical specimen are necessary and can strongly point to the primary tumor [10].
In our case, the diagnosis of thyroid metastasis from lung adenocarcinoma was made on the basis of pathological examination with immunohistochemical complement. Curative management is based on the histological type and respectability of the primary tumor [1]. Medical treatment with chemotherapy is proposed in addition to or in the absence of surgical possibilities, taking into account the histological type of the primary tumor and the general condition of the patient.
Conclusion
The thyroid gland can be a rare site of metastasis for many tumors, especially in an abnormal thyroid gland. This diagnosis should always be considered in the presence of swelling of the gland, especially in the presence of a history of cancer. In the case of such a clinical picture, investigations should be completed by a cytopunction and an appropriate extension work-up. If other metastases are found and the thyroid is not the only organ affected, and the patient has a short life expectancy, the only reason to perform surgery is to obtain tracheal decompression and thus give the patient a better quality of life.
References
-
Rodier JF, Tuech JJ, Wilt M, Lindas P, Rodier CB (2008) A locally advanced intrathyroid metastasis of bronchial cancer. Ann Otolaryngol Chir Cervicofac 125(4): 198- 203.
-
Battistella E, Pomba L, Mattara G, Franzato B, Toniato A (2020) Metastases to thyroid gland: review of incidence, clinical presentation, diagnostic problems and surgery, our experience. J Endocrinol Invest 43(11): 1555-1560.
-
Willis RA (1931) Metastatic tumours in the thyroid gland. Am J Pathol 7(3): 187-208.
-
Zivaljevic V, Jovanovic M, Perunicic V, Paunovic I (2018) Surgical treatment of metastasis to the thyroid gland: a single centre experience and literature review. Hippokratia 22(3): 137-140.
-
Chung AY, Tran TB, Brumund KT, Weisman RA, Bouvet M (2012) Metastases to the thyroid: a review of the literature from the last decade. Thyroid 22(3): 258-268.
-
Chung AY, Tran TB, Brumund KT, Weisman RA, Bouvet M (2012) Metastases to the thyroid: a review of the literature from the last decade. Thyroid 22(3): 258-268.
-
Heffess CS, Wenig BM, Thompson LD (2002) Metastatic renal cell carcinoma to the thyroid gland: a clinicopathologic study of 36 cases. Cancer 95(9): 1869- 1878.
-
Dhouib H, Ben Hmida A, Daoud J, Frikha M, Charfeddine I, et al. (2009) A case of thyroid metastasis of an unusual cancer. Cancer Radiothe 13(3): 213-215.
-
Russell JO, Yan K, Burkey B, Scharpf J (2016) Non thyroid metastasis to the thyroid gland: case series and review with observations by primary pathology. Otolaryngol Head Neck Surg 155(6): 961-968.
-
Wirtz G, Quoix E, Grunenberger F, Massard G, Mennecier B (2009) Thyroid metastasis of lung cancer and abnormal thyroid function-a case report. Rev Pneumol Clin 65(1): 27-31.
-
Valo I, Verriele V, Giraud P, Lorimier G, Guyetant S, et al. (2004) Thyroid metastases of an adrenocortical carcinoma 41 years after the diagnosis of the primary tumor. Ann Pathol 24(3): 264-267.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty