Neuroendocrine Tumor in the Common Bile Duct, a Case Report
Introduction
Neuroendocrine tumors (NET) are a rare type of tumor that develops from enterochromaffin and kulchitsky cells, which have endocrine and nervous system characteristics [1]. These tumors can occur anywhere in the body, but the intestine, lungs, and pancreases are the most commonly affected [2]. The incidence of Gastrointestinal NET is 0.2 to 2% [1]. There are numerous types of neuroendocrine tumors, some of which proliferate. Others, on the other hand, grow slowly, which is how they got their name (carcinoid), which means cancer-like [2]. Neuroendocrine tumors are classified by WHO based on their anatomical location or histological grade. Neuroendocrine tumors are classified into three grades based on mitotic index and Ki-67 index, with well-differentiated NET being the highest. Mixed NET, hyperplastic, and pre-neoplastic lesions were added as new categories [3]. They are also classified according to the staging scheme [2]. Furthermore, neuroendocrine tumors are classified as functional or nonfunctional. These functional tumors secrete hormones such as serotonin and other substances that cause signs and symptoms such as flushing, diarrhea, wheezing, and palpitation in patients. Approximately 60% of NETs are nonfunctional and do not release enough substances to cause symptoms, which explains why they are diagnosed later [2]. Various imaging and laboratory tests are used to make the diagnosis [4]. However, treatment varies depending on the type of tumor, grade, and stage, but surgical resection and postoperative chemotherapy are the mainstays of treatment [1, 4]. In this report, we discuss a case of primary hepatic neuroendocrine tumor, a rare type of neuroendocrine tumor found in the common bile duct in a 44-year-old female patient.
Case Presentation
Our patient is a 44-year-old female, medically free, and a known case of liver mass since 2011. The mass was discovered incidentally when the patient presented with right upper quadrant pain. It had a sudden onset, was colicky, and radiated to the back. It was intermittent and decreased by analgesia. An abdominal ultrasound revealed three focal lesions on the left liver lobe measuring about 2*3*3cm and another on the right side, about 2*2.5cm. The gallbladder and common bile duct (CBD) showed no abnormalities. No further investigations were carried out at the time since the patient was a foreign citizen and opted to return to her country. She was admitted as a case of liver mass. A detailed history was taken, which reported hemorrhoids of 1-year duration, and was otherwise insignificant. For 7 years, the patient was off the record before showing up again in 2018. She underwent a diagnostic laparoscopy, and a true cut biopsy was obtained for histopathology. The examined levels were free of malignancy and were initially diagnosed as a case of hamartoma. Hence, the patient was planned for left hepatectomy.
The procedure uncovered a 6*5cm mass at the porta hepatis, involving liver segments 4 and 5, which had mostly arisen from the hepatic duct. As well as a 2*3cm mass at the peripancreatic lymph nodes. There were no other hepatic lesions, and the vessels were intact. Histopathology report revealed a pseudoencapsulated tumor with infiltrative margins composed of sheets and trabecular of large polygonal neoplastic cells with abundant oncocytic to clear cytoplasm, open chromatin, some showing signet ring- like appearance. The tumor cells were distributed in a fibrous stroma. Multiple foci of necrosis were seen-mitosis 1-2/10HPE. The surrounding liver was not cirrhotic. Based on those pathological findings, the mass had features mostly of hepatic cellular carcinoma - fibrolamellar type or metastatic adenocarcinoma from the gastrointestinal tract. The special stains as PAS and Alcian blue, were focal positive. Immunohistochemical stains such as HEP-PAR1, CK7, CK20, CK8/18, and CAM 5.2 were required for final diagnosis but unfortunately were unavailable at our institute, and the patient could not afford having them done in a private lab. The Lymph Node Mass was a Metastatic Tumor Deposit.
In addition, the patient underwent an abdominal and chest CT scan, which revealed the absence of metastatic tumor elsewhere. The patient then underwent an upper and lower GI endoscopy. The upper GI endoscopy displayed an active duodenal clean-based ulcer, while the lower GI endoscopy was clear.
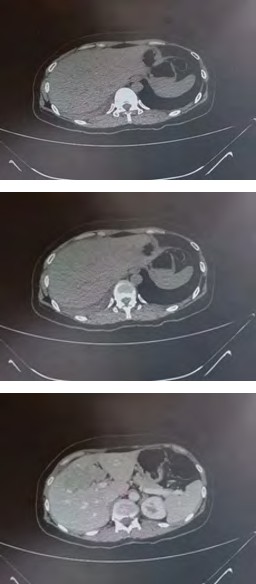
(A) (B)
(C) (D)
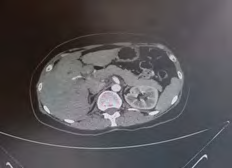
(E) (F) Figure1: This figure is of multiple phases of a contrast enhanced triphasic liver CT scan. Figures A – F show an axial view of different levels of the liver. A contrast enhanced lesion can be seen at the common bile duct.

(A) (B)

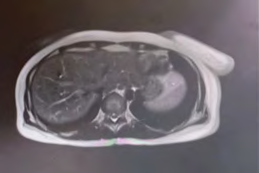
(C) Figure 2: Figure G-I show a stricture in the common bile duct via MRCP.

Discussion
Primary hepatic neuroendocrine neoplasms (PHNENs) are sporadic, accounting for less than 1% of all resected primary neoplasms of the liver [5]. Since Edmondson’s first report of this disease in 1958 [6], 150 neuroendocrine tumor (NETs) cases have been reported in the English literature until 2019, and less than 200 till today [7, 8]. This is since the liver is the organ most commonly affected by neuroendocrine tumor metastases; mostly from gastrointestinal tract (GIT) NETs, as 54% to 90% of NETs cases originate in the GIT, primarily in the appendix, small bowel, and rectum [9]. No consensus has been reached because of their rarity, despite claims that they are caused by either ectopic pancreatic tissue or intrahepatic bile duct progenitor epithelium cells [10]. Our case supports both claims since two masses were found; one at the peripancreatic lymph nodes and the other at the porta hepatis, which is thought to have originated from the hepatic ducts.
There has been no definitive sex prevalence reported Luchini C, et al. [5], although some studies stated that a higher number of males were affected within their sample [11], and the average age at diagnosis is in adulthood (around 50 years), with very few cases under the age of 40 [5]. Our patient was diagnosed with PHNET at 44, although she had an earlier onset of symptoms seven years prior to presentation (i.e.; at the age of 37). To the best of our knowledge, this is the first case of a PHNET published from Jordan with a prolonged latent phase starting from an uncommon starting point going around the average age and other aspects mentioned later.
NETs can be classified as functional or nonfunctional depending on whether they secrete hormones and whether those hormones induce any clinical symptoms. In contrast to other NETs, PHNENs are typically nonfunctional [12]. These tumors have slow growth and low-grade malignancy and only become clinically evident at advanced stages. Nonspecific symptoms such as stomach discomfort, abdominal pain, weight loss, fatigue, and abdominal masses are the most prevalent clinical symptoms. They were followed by no clinical symptoms, which are generally recognized as space- occupying lesions discovered upon performing a physical examination. There have also been reports of Cushing syndrome, carcinoid syndrome, and obstructive jaundice [12, 13]. This patient presented with a known case of liver mass of 7 years duration. At the time of diagnosis, the patient presented with right upper quadrant pain. She did not suffer from any other symptoms, and the hepatic mass was revealed by ultrasound, which supports past literature. The patient, being a foreign citizen, did not stay for further investigations, so her workup was not completed.
She was later found to have a clean-based duodenal ulcer, yet we could not rule out tumor gastrin secretion associated with duodenal ulcer and related to Zollinger- Ellison syndrome mentioned in previous studies Hanzawa S, et al. [14]. Moreover, the tumor’s course was slower than familiar, with a prolonged latent phase (years). After taking a detailed history, the patient revealed she suffered from hemorrhoids in 2017 (6 years after her first presentation). To the best of our knowledge, no previous studies have linked the pathogenesis or prognosis, or worsening of PHNENs with hemorrhoids. Hence we encourage future researchers to explore any possible associations.
In general, imaging techniques, including ultrasonography, CT scans, and MRI play a crucial role in the diagnosis of liver masses. Most PHNENs have an abundant blood supply, but they lack radiological characteristics that set them apart from other liver tumors, and they are frequently misdiagnosed as hepatocellular carcinoma. In addition, while PET/CT cannot be used to diagnose PHNENs directly, it can be used to determine whether the NET originated in the liver. Alpha-fetoprotein (AFP) and carcinoembryonic antigen (CEA), two serum tumor markers, have no practical diagnostic utility in diagnosing PHNENs [10, 15]. In our case, an ultrasound picked up a hepatic mass that showed 3 focal lesions on the left lobe (2*3*3cm) and another on the right side (2*2.5cm). Then diagnostic laparoscopy was conducted. The lesion on the right surface looked soft, with a mildly depressed surface. During this procedure, a true cut biopsy was done, bringing us to the most reliable form of diagnosis, the histopathological investigations [16].
A biopsy can be obtained by a fine needle or post- surgically (true-cut biopsy) after resecting the mass. However, the fine needle biopsy has not proven to be accurate enough. Therefore, true-cut biopsies followed by post-surgical histological and immunohistochemical assessment is the primary procedure for ultimate diagnosis [17].
Hematoxylin and Eosin (HE) staining is helpful in classifying tumors. Special stains, such as Masson’s, can boost the diagnosis rate to 80% or higher. Immunohistochemistry improves accuracy by identifying markers such as synaptophysin, neuron-specific enolase, CD56, chromogranin, and others. It is also helpful in computing the mitotic index and the Ki-67 index [18]. Other immunohistochemistry stains have demonstrated the ability to detect tumor origins, such as CDX2 with gastroenteropancreatic origin, TTF-1 with tumors of thoracic origin, the transcription factor PDX1, which has been reported to have a particular specificity for pancreatic NETs, and others Luchini C, et al. [19]. In regards of our patient, a true cut biopsy was taken post-operatively and stained with Masson’s trichrome and retic special stains (the most reliable biopsy and stain). Further Alcian Blue and PAS stain were used and showed positive focal results. The first 2 Immunohistochemistry tests were negative for any Mets markers (ttf-1,ck20,pax08,cd34, gata-3 ,cdx2 and mucicarmine special stain was negative) and were positive for CK-7, chromogranin , synaptophysin, and the Ki-67 was (15%), also it was important to mention that the 3rd test done 6 month later showed a cdx2 positive which supports the double origin statement and shows the importance of keeping a long-term follow-up with periodic imaging tests due to the need of excluding an eventual primary site of the disease different from that of first presentation, suggesting the accumulation of mutations as a result of the long latent period [20].
The current WHO classification for NETs in 2019 contains three grades (G1, G2, and G3) that are connected to both the mitotic index and the ki-67 index: NET G1 has 2 and 3 percent, respectively, whereas NET G2 has 2-20 and 3-20 percent, and NET G3 has >20 and >20 percent, respectively Yang K, et al. [16]. The current instance had a low cellular proliferation index, as demonstrated by the low Ki-67 (15%) and 1-2 mitotic figures per 10 high power fields, suggesting a favorable prognosis for this case, which was classified as a G2 by the WHO. It is unclear whether the tumor grade is linked to the prognosis; some studies find a positive association, while others find a negative correlation [21].
Surgical methods in treating PHNENs have proven to be more successful than medical methods, with a 74% five- year survival rate and a recurrence rate of approximately 18%. The size and location of the tumor influence resection; Tumors with multiple foci that encompass both liver lobes are treated with different methods, including selective hepatic artery embolization, radiofrequency ablation, and hepatectomy with liver transplant. Transcatheter arterial chemoembolization (TACE), systemic chemotherapy, local ablation, and somatostatin analogs failed to demonstrate a long-term survival advantage. TACE had a positive first reaction only in the short term. It reduces tumor size, which is advantageous prior to surgical excision. Despite various management modalities, reaching an agreement on a treatment strategy remains challenging because of the rarity of the disease [22, 23, 24]. Recent studies assured that surgical treatment is now the best option, with histological and immunohistochemical confirmation and monthly follow-ups [10]. Our patient underwent a left hepatectomy; she was monitored in the wards until she was stable, and then was discharged to recover at home, with scheduled follow-ups.
Conclusion
PHNENs are a rare entity of neuroendocrine neoplasms. Their diagnosis is made difficult because of the lack of distinctive radiologic characteristics. Hence, they are diagnosed by exclusion, and histologic testing is used for confirmation. When feasible, surgical resection is the mainstay of treatment. In other instances, when surgery is not an option, combining TACE and somatostatin analogs administration has good results in palliative care.
Acknowledgments
This research was mentored and supervised by the Mutah Research and Audit Society (MRAS).
References
-
Miri SR, Movaghar ER, Safaei M, Sharifi A (2020) Neuroendocrine tumor of the common bile duct: a case report of extremely rare cause for obstructive jaundice. International Journal of Surgery Case Reports 77: 303- 306.
-
Neuroendocrine tumors: Introduction. Cancer net
-
Lee ST, Kulkarni HR, Singh A, Baum RP (2017) Theranostics of neuroendocrine tumors. Visceral medicine 33(5): 358-366.
-
Neuroendocrine tumors - diagnosis. Cancer Net
-
Luchini C, Pelosi G, Scarpa A, Mattiolo P, Marchiori D, et al. (2021) Neuroendocrine neoplasms of the biliary tree, liver and pancreas: a pathological approach. Pathologica 113(1): 28-38.
-
Pathology HEA of tumor (1958 )Tumors of the liver and intrahepatic bile ducts.
-
Costa AC, Cruz FS, Guimaraes H, Paz AR, Costa EAC, et al. (2020) Primary hepatic neuroendocrine tumor: A case report and literature review. International Journal of Surgery Case Reports 72: 1-4.
-
Xia Y, Zhang L, Wu H, Qiao L, Xia L (2020) Primary hepatic neuroendocrine tumor with multiple liver metastases: A case report with literature review. The Journal of International Medical Research 48(6): 1-8.
-
Camargo ES, Viveiros M de M, Correa Neto IJF, Robles L, Rezende MB (2014) Primary hepatic carcinoid tumor: case report and literature review. Einstein 12(4): 505- 508.
-
Elayan A, Batah H, Badawi M, Saadeh A, Hafez SA (2022) Primary Hepatic Neuroendocrine Tumor: A Case Report and Literature Review. Cureus 14(2): e22370.
-
Brad DK, Kodiatte TA, Rajeeb SM, Goel A, Eapen CE, et al. (2016) Neuroendocrine neoplasms of liver - A 5-year retrospective clinicopathological study applying World Health Organization 2010 classification. World Journal of Gastroenterology 22(40): 8956-8966.
-
Yu WM, Li R, Sun BL, Du JK, Tuo HF (2021) Primary hepatic neuroendocrine tumor with multiple liver metastases: A case report with literature review. International Journal of Surgery Case Reports 89: 106590.
-
Shi C, Zhao Q, Dai B, Xie F, Yang J (2018) Primary hepatic neuroendocrine neoplasm Long-time surgical outcome and prognosis. Medicine 97(31): e11764.
-
Hanzawa S, Sadamori H, Kagura M, Monden K, Hioki M, et al. (2020) Primary hepatic gastrinoma being diagnosed preoperatively: a case report and literature review. Surgical Case Reports 6(1): 290.
-
Hu HX, Yu T (2019) Primary hepatic neuroendocrine tumors: A case report. Medicine 98(50): e18278.
-
Yang K, Cheng YS, Yang JJ, Jiang X, Guo JX (2015) Primary hepatic neuroendocrine tumor with multiple liver metastases: A case report with review of the literature. World Journal of Gastroenterology 21(10): 3132-3138.
-
Quartey B (2011) Primary Hepatic Neuroendocrine Tumor: What Do We Know Now? World Journal of Oncology 2(5): 209-216.
-
Shah D, Mandot A, Cerejo C, Amarapurkar D, Pal A (2019) The Outcome of Primary Hepatic Neuroendocrine Tumors: A Single-Center Experience. Journal of Clinical and Experimental Hepatology 9(6): 710-715.
-
Luchini C, Pelosi G, Scarpa A, Mattiolo P, Marchiori D, et al. (2021) Neuroendocrine neoplasms of the biliary tree, liver and pancreas: a pathological approach. Pathologica 113(1): 28-38.
-
Song JE, Kim BS, Lee CH (2021) Primary hepatic neuroendocrine tumor: A case report and literature review. World Journal of Clinical Cases 4(8): 243.
-
Costa AC, Cruz Fs, Guimaraes H, Paz AR, Costa EAC, et al. (2020) Primary hepatic neuroendocrine tumor: A case report and literature review. International Journal of Surgery Case Reports 72: 1-4.
-
Schwartz G, Covanta A, Gaetz H, Olichney J, Attiyeh F (2008) Primary carcinoid tumors of the liver. World Journal of Surgical Oncology 6: 91.
-
Touloumis Z, Delis SG, Triantopoulou C, Giannakou N, Avgerinos C, et al. (2008) Primary hepatic carcinoid; a diagnostic dilemma: a case report. Cases Journal 1(1): 314.
-
Nikfarjam M, Muralidharan V, Christophi C (2004) Primary hepatic carcinoid tumours. HP 6(1): 13.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty