Significance of Chromogranin A and Synaptophysin in Parathyroid Proliferative Lesions: Immunohistochemical Study on Parathyroid Adenoma, Atypical Adenoma, Carcinoma and Hyperplasia
Introduction
Chromogranin A (CgA) and synaptophysin (SPY) are the two most used immunocytochemical markers for neuroendocrine cells and their tumors in pathology laboratory [1, 2, 3, 4, 5, 6]. CgA is the most specific marker for neuroendocrine granules and SPY is the most sensitive marker in well-differentiated neuroendocrine tumors (NETs) [6]. Parathyroid lesions are concurrently immunopositive for parathyroid hormone and CgA but the status for SPY immunostaining in parathyroid gland (PG) has not been yet settled. Primary hyperparathyroidism (P-HPT) became the common endocrine disorder by the introduction of automated serum calcium measurement with Technicon in mid-1974 [7]. The current incidence of P-HPT has been reported as low as 17.7 cases per 1,000,000 persons in the US [8] while another reported incidence was as high as 42 per 100,000 [7]. P-HPT predominates in women with a female to male ratio of 3 - 4: 1 and an average age at diagnosis of 55 years [7, 8, 9] with its prevalence up to 4 per 1,000 in women over age 60 [9]. P-HPT refers to the inappropriate overproduction of parathyroid hormone (PTH), resulting in abnormal calcium homeostasis [7, 8, 9]. The level of PTH is inversely proportional to the serum calcium level, which is tightly controlled between 8.8 and 10.5mg/l [7]. In patients with P-HPT, the elevated serum calcium level is above 1mg/dl of the upper limit and twice as many levels of serum calcium [7, 8, 9, 10]. The negative feedback relationship of P-HPT with serum Ca++ is steeply sigmodal with the steep portion of the curve responsible to the normal range of serum Ca++ where low serum Ca++ stimulates plasma PTH levels and high serum Ca++ levels inhibit plasma PTH levels [7]. Under extreme hypercalcemia in patients with parathyroid carcinoma, un- controllable hyperparathyroidism would emerge [10, 11]. About 90% of patients with P-HPT have elevated plasma PTH levels while the remaining patients have normal plasma PTH levels [9]. The plasma C-terminal PTH levels in adults are between 18 and 65pg/ml [7]. Patients with P-HPT are generally asymptomatic despite the laboratory findings of hypercalcemia, hypophosphatemia, hypercalciuria, increased serum PTH and normal levels of parathyroid -related protein [7]. P-HPT may resort from adenoma/single-gland disease (80-85%), primary parathyroid hyperplasia (PPH) /multi- gland disease (10-15%) or rare carcinoma (< 1%) [7, 8, 9, 10] and parathyroid proliferative lesions may have a clonal origin [4]. CgA immunostaining is widely distributed in adrenal medulla, thyroid C-cells, anterior pituitary cells, intestinal neuroendocrine cells, parathyroid chief cells, pancreatic endocrine cells and others and the strong CgA immunostaining corresponds to aggressive marker in pancreatic NETs and medullary thyroid carcinomas [12, 13]. The majority of CgA immunopositive tumors are also immunopositive for SPY [3, 5, 6]. However, structure-function relationship for SPY in PGs had not been thoroughly scrutinized [2, 12, 13] and this study aimed to explore the roles of CgA and SPY in normal PGs, adenoma, carcinoma and hyperplasia. Histopathology of HPT represents hypercellular PGs with less fibroadipose tissue, which increases with age reaching 50% of the gland at age 50 [8, 9]. Immunohistochemical staining helps to diagnose hyperfunctioning lesions with less staining for PTH while they were 98% positive for CgA and only 11% positive for SPY as reported by Yu Q, et al. [14]. We studied wet weight of PGs and relative immunohistochemical staining intensity for PTH, CgA and SPY.
Materials and Methods
Five cases of normal PGs were collected from the euparathyroid autopsy cases with normal serum calcium and phosphate levels. Four PGs in each case were resected from each case and were weighed in the fresh state as previously reported (Table 1) [15].
| Immunohistochemical Staining | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case No | Age/ Sex | NO of PGs | Total Weight (mg) | Parathyroid Hormone (%) | Chromogranin A (%) | Synaptophysin (%) | ||||||
| 2+ | 1+ | 0 | 2+ | 1+ | 0 | 2+ | 1+ | 0 | ||||
| 1 | 51/F | 4 | 130 | 90 | 10 | 0 | 85 | 15 | 0 | 0 | 0 | 100 |
| 2 | 56/F | 4 | 160 | 76 | 20 | 4 | 78 | 20 | 2 | 0 | 0 | 100 |
| 3 | 66/F | 4 | 220 | 100 | 0 | 0 | 100 | 0 | 0 | 0 | 0 | 100 |
| 4 | 71/M | 4 | 140 | 64 | 27 | 9 | 0 | 90 | 10 | 0 | 0 | 100 |
| 5 | 83/M | 4 | 130 | 100 | 0 | 0 | 100 | 0 | 0 | 0 | 0 | 100 |
| Mean | 65.4 | 4 | 156 | 86 | 11.4 | 2.6 | 72.6 | 25 | 2.4 | 0 | 0 | 100 |
| SE | 5.6 | 0 | 17 | 7 | 5.4 | 1.8 | 18.6 | 1.6 | 1.9 | 0 | 0 | 0 |
Table 1: Normal Parathyroids.
P-HPT cases included 13 parathyroid adenomas, one atypical adenoma, one case each of primary and metastatic parathyroid carcinomas and 8 cases of PPH, all of which were removed by surgery (Tables 2). All the tissues were fixed in 10% buffered formalin and embedded in paraffin. The deparaffinized sections were treated with citrate buffer (0.1 N, pH 6.0) for 10min in Biocare Medical pressure cooker. In the previous study, monoclonal anti-human PTH (1: 100
dilution, Dako Corp, Carpenteria, CA) and monoclonal anti- CgA (both at 1: 100 dilution, BioGenix, Lab, San Ramon, CA) were used. For the current study, the tissue sections were initially incubated with anti-human PTH and monoclonal anti-CgA antibody (both from Dako Corp., at x 1: 100 dilution, clone DAK-A3, Santa Clara, CA) and rabbit anti- synaptophysin (SPY) (1: 200 dilution, Cell Marque, Cat 336-76, Rocklin, CA). Immunohistochemical staining was performed at each batch of 20 tissue sections to obtain comparative staining intensity including normal parathyroid sections. For evaluating immunohistochemically stained sections, 1 to 8 microscopic low-power fields (4x10=x40) were estimated for 0 as negative staining, 1+ and 2+ with the strongest stained area in the normal gland set at 2+ with a 10% incrementally increasing percentage of the microscopic tissue area as previously reported [15] plus newly added two carcinoma cases in this study. Mean and standard error were calculated.
Results
The mean total weight of normal PGs was 156 mg, ranging from 130mg to 220mg (Table 1). The normal gland showed about 13% interstitial fat and consists of over 90% chief cells, which were strongly positive for PTH and CgA in majority of the cells. Oxyphil cells are minor component at 0 to 15% (Figures 1 A-D). The normal parathyroid Case 1, from a 51 years-old woman, measuring 0.5x0.4cm, consisted of uniformly dense chromatin-dense small nucleus and small clear chief cells within about 50% of the adipose tissue (Figure 1A). The cytoplasm was densely and diffusely positive for PTH in nearly 100% (Figure 1B) while CgA immunostaining was diffusely for 85% with 15% of which was weakly positive (Figure 1C), and the entire normal cells were negative for SPY immunostaining (Figure 1D). All adenomas were single-gland tumor, and the mean weight was 2.7g, ranging from 0.4g to 8.0g (Table 2).
| Adenomas | Immunohistochemical Staining | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| S.No. | Age/Sex | Weight (g) | Parathormone (%) | Chromogranin A (%) | Synaptophysin (%) | ||||||
| 2+ | 1+ | 0 | 2+ | 1+ | 0 | 2+ | 1+ | 100 | |||
| 1 | 18/F | 2.5 | 0 | 39 | 61 | 0 | 10 | 90 | 0 | 0 | 100 |
| 2 | 36/M | 6 | 0 | 12 | 88 | 0 | 5 | 95 | 0 | 0 | 100 |
| 3 | 43/F | 8 | 0 | 75 | 25 | 0 | 10 | 90 | 0 | 0 | 100 |
| 4 | 45/F | 1 | 0 | 100 | 0 | 100 | 0 | 55 | 0 | 0 | 100 |
| 5 | 47/F | 5 | 0 | 4 | 96 | 0 | 9 | 91 | 0 | 0 | 100 |
| 6 | 47/F | 1.5 | 44 | 56 | 0 | 0 | 36 | 64 | 0 | 10 | 90 |
| 7 | 48/M | 0.4 | 0 | 90 | 10 | 0 | 80 | 20 | 0 | 0 | 100 |
| 8 | 51/F | 4.8 | 0 | 56 | 44 | 0 | 55 | 45 | 0 | 0 | 100 |
| 9 | 53/M | 1.5 | 32 | 68 | 0 | 65 | 35 | 0 | 0 | 0 | 100 |
| 10 | 67/F | 0.6 | 0 | 78 | 22 | 0 | 100 | 0 | 0 | 0 | 100 |
| 11 | 69/M | 3.5 | 30 | 50 | 20 | 30 | 55 | 15 | 0 | 0 | 100 |
| 12 | 74/F | 1.6 | 0 | 74 | 26 | 70 | 20 | 10 | 0 | 35 | 65 |
| 13 | 77/F | 0.5 | 10 | 70 | 10 | 0 | 5 | 95 | 0 | 0 | 100 |
| Mean | 52.4 | 2.7 | 7.2 | 60.2 | 32.8 | 19.6 | 30.4 | 54.2 | 0 | 16 | 93 |
| 4 | 0.9 | 4.3 | 8.4 | 9.9 | 10 | 9.4 | 11 | 0 | 11 | 8 |
Table 2: Parathyroid Adenomas, Atypical Adenoma and Carcinomas.
Atypical Adenoma (1)
| 1 | 81/M | 5 | 0 | 10 | 90 | 5 | 30 | 65 | 0 | 0 | 100 |
|---|
Table 3: Parathyroid Adenomas, Atypical Adenoma and Carcinomas.
| 1 | 44/Fa | 4 | 90 | 10 | 0 | 0 | 5 | 95 | 0 | 0 | 100 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 55/Fb | 2 | 85 | 15 | 0 | 0 | 80 | 20 | 0 | 0 | 100 |
Table 4: Parathyroid Adenomas, Atypical Adenoma and Carcinomas.
a: Primary carcinoma, b: Metastatic carcinoma Table 2: Parathyroid Adenomas, Atypical Adenoma and Carcinomas.
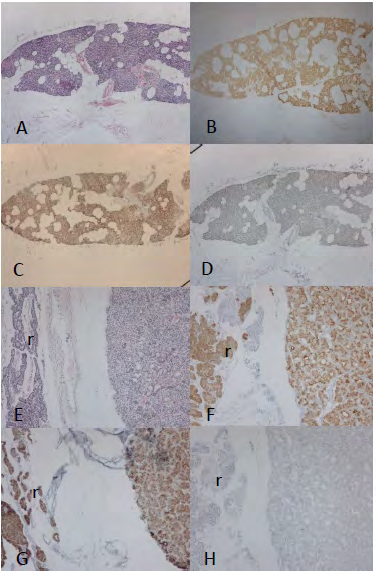
There was little interstitial fat tissue, and the majority was chief cells (Figure 1E) (Table 2). In Case 7 adenoma from a 48 years-old male, weighing 0.4g and measuring 0.8x0.4cm, composed of the densely packed adenomatous chief cells with no interstitial adipose tissue as compared to the rim of the normal parathyroid tissue, which contained about 25% of adipose tissue area (Figure 1E). The packed adenomatous chief cells composed of twice larger clear amphophilic cytoplasm and slightly larger nucleus compared to the rim of the normal tissue (Figure 1E). Thus, this adenoma consisted of larger cytoplasm and nucleus than the adjacent smaller normal rim and was moderately and granular stained for PTH and CgA compared to the densely immunostained normal rim tissue for PTH and CgA while both adenomatous tissue and normal rim tissue were negative for SPY (Figures 1F to H). Case 6 adenoma, weighing 1.5g and measuring 1.5x0.9cm, consisted of adenomatous tissue attached with normal adjacent parathyroid cells, the latter contained about 15% fat with a small fat tissue at the margin of the adenoma (Figure 2A).
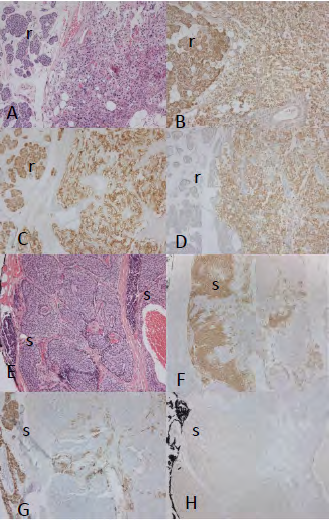
The adenomatous cells composed of more than twice larger clear and amphophilic cytoplasm and slightly larger nucleus (Figure 2A). By PTH immunostaining, adenomatous cells were moderately and granular stained compared to the densely stained normal tissue while CgA granular staining was a bit weaker and SPY staining was moderately and diffusely positive for the adenoma (Figures 2B to D). This case was one of two adenomas positively immunostained for SPY (Figure 2D) (Table 2). The previously reported low- grade parathyroid carcinoma from 81 years-old male, was reclassified as atypical adenoma this time since there was no invasion into the adjacent organs nor recurrences after surgery (Table 2).The tumor consisted of two components: the outer lobules, consisting of 10% of this tumor tissue were moderately positive for PTH and partly positive for CgA and the major inner lobules, consisting of 90% of the tumor tissue were negative for PTH and CgA, and both outer and inner lobules were negative for SPY (Figures 2F to H). Thus, this tumor consisted of inner lobules of moderately PTH and CgA immunostained packed small cells and major mid- portion of the larger, amphophilic tumor cells, which were negatively immunostained for PTH, CgA and SPY (Figures 2E to H). There was no tumor invasion into and beyond the tumor capsule (Figure 2E).
Legend to Figure 1
The normal parathyroid gland consisted of small amphophilic cytoplasm and small dark nucleus within inter- glandular adipose tissue (A). Normal gland was diffusely and strongly positive for PTH (B) and moderately to strongly positive for CgA in 90% of the cells (C) while normal parathyroid cells were completely negative for SPY (D). This Case 7 small adenoma attached with normal rim consisted of twice as large cytoplasm and slightly larger nucleus than the normal rim cells (E). The adenomatous cells were moderately immunostained for PTH (F) and CgA (G) and were completely negative for SPY (H). r: normal rim.
Legend to Figure 2
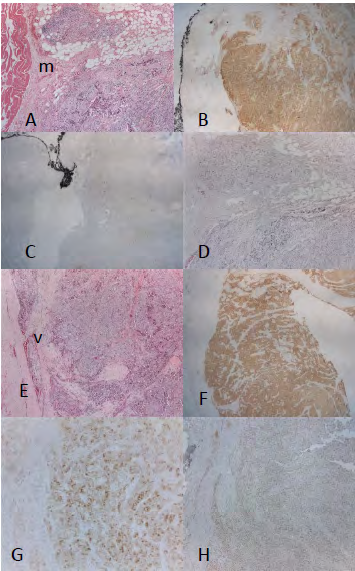
This Case 6 adenoma attached with normal rim consisted of twice larger amphophilic cytoplasm and slightly larger nucleus (A), which was moderately and diffusely immunostained for PTH (B) and CgA (C) while they were moderately positive for SPY (D). This atypical adenoma consisted of nests of amphophilic tumor lobules surrounded by fibrous bands and attached with nests of darkly stained small cell nests at the tumor margin (E), the latter was moderately positive for PTH (F) and moderately and patchy immunostained for CgA (G) while the mid-portion of the tumor cells were negative for PTH and CgA. r: normal rim, s: small cell lobule Case 1 primary carcinoma from 44 years-old female, weighing 4 g and measuring 1.6x1.0cm, invaded into the adjacent neck skeletal muscle and adipose tissue, and consisted of densely solid tumor lobules, composed of larger moderately eosinophilic cytoplasm and slightly larger nucleus (Figure 3A). The tumor lobules were separated by thin to thick fibrous bands with no adipose tissue (Figure 3A). About 90% of the tumor cells were strongly positive for PTH while about 5% of them were weakly and sporadically positive for CgA and were completely negative for SPY (Figures 3B to D). Case 2 from 55 years-old female, weighing 2g and measuring 1.2x1.0cm, was metastatic tumor to the neck lymph node with vascular invasion at the tumor periphery and composed of nodular tumor lobules, packed with eosinophilic tumor cells containing larger nuclei with prominent nucleoli and more than twice larger cytoplasm of the normal cell cytoplasm (Figure 3E). The tumor lobules were separated by thick fibrous bands with no interstitial fat (Figure 3E). The tumor cells were strongly and diffusely positive for PTH and were moderately positive in about 90% of the tumor cells for CgA and were totally negative for SPY (Figures 3F to H). The two carcinomas were diffusely and strongly positive for PTH but unevenly positive for CgA immunostaining in less than PTH immunostaining in the entire tumor tissue (Figures 3B, 3C, 3F, 3J) (Table 2).
Legend to Figure 3
This primary carcinoma Case 1 invaded into the adjacent skeletal muscle and consisted of solid tumor nests surrounded by thin fibrous bands with vascular invasion at the tumor periphery (A). The eosinophilic tumor cells were diffusely and strongly positive for PTH (B) and focally and weakly positive for CgA (C) and completely negative for SPY (D). This metastatic Case 2 carcinoma consisted of solid eosinophilic tumor cell nests separated by thick fibrous bands, containing vascular tumor invasion at the tumor margin (E). The tumor cells were diffusely and strongly positive for PTH (F) and diffusely and mildly positive for CgA (G) and were completely negative for SPY (H). m: skeletal muscle,*: vascular invasion of tumor cells.
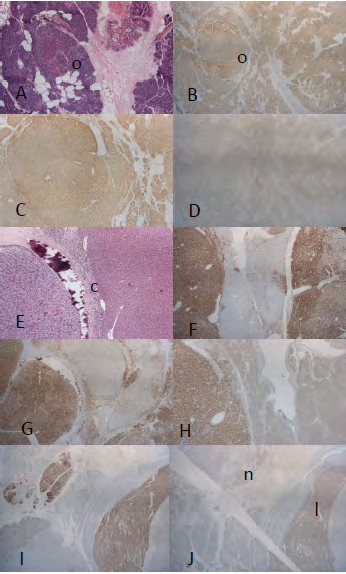
In PPH, the total mean weight of the combined four glands was 5.9g, ranging from 1.3g to 14.1g (Table 3) and consisted of chief cells over 90% of the cells. Among eight cases, there was some but decreased interstitial fat than in the normal PGs. PHT and CgA immunostaining was less than that of the normal parathyroid cells (Table 3). There was no strong staining for PTH and CgA as PTH staining between 1+ and 0 and CgA staining was mostly 1+ at less staining than PTH staining (Table 3). The majority was chief cells and PTH staining was less than that of normal parathyroid cells as the staining was mostly 1+ and CgA staining was 1+ (Table 3). Case 4 PPH from 41 years-old female, weighing 1.3g and measuring 1.0x0.8cm, composed of densely packed chief cells of normal sized nucleus and cytoplasm within 10% adipose tissue stroma (Figure 4A). The hyperplastic cells were weakly and diffusely positive for PTH and CgA immunostaining and was completely negative for SPY (Figures 4B to D). Case 3 PPH from 38 years- old male, weighing 8.1g and measuring 1.5x1.0cm, consisted of larger lobular nests separated by thin fibrous stroma and composed of small clear chief cell nests and small, strongly amphophilic, oxyphilic cell nests (Figure 4E). The chief cell nests were strongly and diffusely positive for PTH while the oxyphilic cells were mostly negative with focal positive for CgA and were moderately positive for SPY in 10% of the cell nests (Figures 4F to H). One more Case 5 of PPH weighed 14.1g and was alternately and moderately positive in tumor lobules for PTH and CgA in 80% and 70%, respectively and 15% weakly positive for SPY (Figures 4I & J).
| Primary Hyperplasia (8) | Immunohistochemical Staining | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case No | Age/ Sex | No of PGs | Total Weight (g) | Parathormone (%) | Chromogranin A (%) | Synaptophysin (%) | ||||||
| 2+ | 1+ | 0 | 2+ | 1+ | 0 | 2+ | 1+ | 0 | ||||
| 1 | 23/M | 4 | 15.4 | 0 | 10 | 90 | 0 | 10 | 90 | 0 | 0 | 100 |
| 2 | 26/F | 4 | 2.7 | 0 | 59 | 41 | 0 | 74 | 26 | 0 | 0 | 100 |
| 3 | 38/M | 4 | 8.1 | 0 | 30 | 70 | 0 | 76 | 24 | 0 | 10 | 90 |
| 4 | 41/F | 4 | 1.3 | 0 | 35 | 65 | 0 | 10 | 90 | 0 | 0 | 100 |
| 5 | 45/F | 4 | 14.1 | 0 | 35 | 65 | 0 | 32 | 68 | 0 | 20 | 80 |
| 6 | 63/M | 4 | 5.4 | 0 | 90 | 10 | 0 | 82 | 18 | 0 | 0 | 100 |
| 7 | 66/M | 4 | 5.3 | 0 | 12 | 88 | 0 | 17 | 83 | 0 | 0 | 100 |
| 8 | 74/F | 4 | 7.5 | 0 | 3 | 97 | 0 | 0 | 100 | 0 | 0 | 100 |
| Mean | 45 | 4 | 5.9 | 0 | 34.3 | 65.8 | 0 | 37.2 | 62.4 | 0 | 3.8 | 96 |
| SE | 4.5 | 0 | 1.7 | 0 | 10.2 | 10.2 | 0 | 12.1 | 12.1 | 0 | 2.6 | 2.6 |
Table 5: Primary Parathyroid Hyperplasia.
Legend to Figure 4
This Case 4 small gland (0.5 x 0.3cm) consisted of lobular nests containing some adipose tissue and a focal oxyphilic nodule (A). The hyperplastic cells were weakly positive for PTH (B) and CgA (C) while they were negative for SPY (D). Case 3 large hyperplastic gland consisted of large hyperplastic nests separated by thick fibrous bands with a partial stromal calcification (E). The hyperplastic nests were moderately positive for PTH (F) and CgA (G). The major hyperplastic cell nests were negative for SPY while there were moderately and partially SPY positive cell nests (H). Another Case 5 large hyperplastic gland composed of two CgA-positive nests (I), among which only one hyperplastic cell nest was weakly positive for SPY (J). c: calcification, l: SPY-positive lobule, n: SPY-negative lobule, o: oxyphilic cells.
Discussion
Almost all normal PG was diffusely and strongly positive for PTH while CgA immunostaining was not all strongly positive using anti-CgA and was completely negative for SPY (Figure 1A to D). Thus, less PTH and CgA immunostaining is a reliable marker for diagnosing hyperfunctioning parathyroid lesions, resulting from less stored PTH in the CgA-containing secretory granules [7, 8, 9]. Immunohistochemical staining in single-gland adenomas and four-gland P-PTH is similar, suggesting that adenomas and PPH cases eventually end up though the similar tumorigenesis while adenomas occur in one gland and PPH occurs in four glands. Proliferative parathyroid lesions were less immunostained for PTH than normal PGs, and this is supported by less tissue extract levels of PTH in adenomas 79±20ng/mg protein (19.1 %) and PPH at 129±20ng/mg (31.2 %) as compared to the normal PGs of 413±106ng/mg [16]. Two carcinoma cases were diffusely and strongly positive for PTH while the tumor cells were sporadically and weakly immunostained for CgA, reflecting abundant stored PTH in the tumor tissues with actively autonomous PTH synthesis associated with much less stored CgA-containing secretory granules in the cancer tissues [7, 8, 9, 10, 11]. We expected markedly decreased PTH and CgA immunostaining in the cancer cases as seen in a case of atypical adenoma (Figures 2F to H). DeLellis reported abundant eosinophilic cytoplasm of parathyroid cancer cells diffusely and moderately positive for PTH immunostained like our two cancer cases [17]. This diffusely strong PTH and weak and partial CgA immunostaining would be characteristic for parathyroid carcinoma being different from atypical adenoma, which were weaker and partially immunostaned for both PTH and CgA. One possible explanation for this is that there are two immunopositive PTHs in the parathyroid cells. One is prepro-PTH with larger amino acids in the ribosome [18], which is CgA-negative and PTH-immunopositive to the current PTH antibody in the ribosome, but not in the CgA-positive secretory granules [12, 18], and the other is CgA-positive PTH inside the CgA- positive secretory granules, the latter in the secretory granule would be secreted immediately to modulate serum calcium homeostasis. There are no available antibodies against prepro-PTH, with which to immunostain prepro-PTH at present. The plasma CgA levels were reportedly elevated in individuals with adenomas at 55±33ng/ml and in PPH at 63±88ng/ml as compared to the normal control levels of 25±8ng/ml [19, 20], which supports increased plasma CgA in individuals with hyperparathyroidism. Atypical parathyroid adenoma and carcinoma are extremely rare, representing < 1% of P-HPT [7, 8, 10, 11] and these tumors secrete autonomous amount of PTH as detected in markedly increased PTH levels in the blood and interstitial fluid [16]. Parathyroidectomy did not decrease CgA blood levels in patients with proliferative lesions, thus the elevated blood CgA level is not a general feature of proliferative lesions since parathyroids are small organs and are not the major source of CgA in the blood [19]. The negative SPY immunostaining in all of the normal PGs and the majority of proliferative lesions was a puzzle to us since the majority of CgA-positive neuroendocrine tumors are all positive for SPY [5, 6, 12, 13], thus parathyroid tissues are exceptional from the other normal neuroendocrine organs and their tumors.
It has been reported that parathyroid adenomas have a monoclonal origin that can be traced back to an oncogenic mutation in a single progenitor cell while PPH has polyclonal expansion and proceeds to monoclonal growth [21, 22]. However, more recent study reported that parathyroid adenomas can arise from monoclonal and polyclonal origin [23]. Thus, clonality on parathyroid proliferating lesions has not settled yet. Adenomas are more diffusely and homogenously less immunostained for PTH and CgA than normal PGs (Figure 2), which may correspond to homogenous, clonal tissue growth while PPH presents mixture of strongly and weakly immunostained nodular nests for PTH and CgA with occasional SPY staining, suggesting heterogenous and polyclonal growth (Figure 4). Secondary parathyroid hyperplasia (SPH) develops following chronic renal disease, responding to an adaptation and in many cases untimely maladaptive process, that develops to declining kidney function with impaired phosphate excretion and failure to bioactive vitamin D [7]. Patients with SPH generally have greater uniformity in parathyroid gland sizes than patients with PPH in further progression the glands often resuming a multinodular configuration [7]. Probably, the earliest phases of surgically resected SPH are polyclonal hyperplasia, followed by monoclonal nodular hyperplasia [21, 22]. Most cancers are of multiclonal origin [24, 25] since cancer is genetic disorder with accumulation of evolution occurring during progression in the model of multistep tumorigenesis [26]. Presuming that monoclonal tumors present more homogenous histopathology and multiclonal tumors present more heterogenous histopathology, it is of great interest that parathyroid adenomas are of monoclonal origin and PPH is of polyclonal expansion and then transforms to monoclonal growth [4] even through the majority of other cancers/tumors are multiclonal origin [24, 25, 26]. The plasma C-terminal PTH levels in adults are between 18 to 65pg/ml [7].The extremely high plasma PTH and serum calcium levels are characteristic for patients harboring parathyroid carcinoma as a result of the loss of negative control of high serum calcium on PTH secretion [6, 7, 8, 9, 16, 27]. This lack of high serum calcium on the inhibitory PTH secretion was demonstrated also in our case of atypical parathyroid adenoma: higher serum calcium: 13.5-13.9mg/dl (normal: 8.3-10.4mg/dl) and lower phosphate: 2.1mg/dl (normal: 3.4-4.5mg/dl), respectively, and serum PTH was 569pg/ml (normal: 10-65pg/ml) at a co- existing hypercalcemia and high PTH in blood before surgery. Thus, these extremely high serum calcium and PTH levels are identical to those with parathyroid carcinoma [27, 28]. Six weeks after tumor resection, serum calcium and PTH were 8.0mg/dl and 86.9pg/ml, respectively [15], with some restoration of normalizing calcium-PTH homeostasis. This atypical adenoma case is undistinguishable from carcinoma regarding to the serum calcium and PTH levels, the latter levels are more than twice the upper limits of normal values [15].
For diagnosing parathyroid carcinoma with serum PTH levels, Duan and Mete proposed serum PTH levels more than three times of upper normal limit (in this case: 65pg/ mlx3=195pg/ml) [29] while Machens et al claim the cut-off point for diagnosing parathyroid carcinoma was 700pg/ml [27], and our case was close to the cut-off point but less than 700pg/ml.
Histopathological diagnosis of parathyroid carcinoma would be made on the basis of vascular invasion or invasion to adjacent structures since it is extremely difficult to differentiate between parathyroid carcinoma and atypical adenoma [9, 10, 30, 31]. The definite criteria for parathyroid carcinoma are:
- Vascular invasion,
- Lymphatic invasion,
- Perineural invasion,
- Local malignant invasion into adjacent anatomic structures and
- Histologically/cytologically documented metastasis [30, 31].
Sandelin et al reported a review of 95 cases of parathyroid carcinoma: a medium time from initial surgery to first recurrence was 33 months (range: 1-228 months), medium survival time from the first recurrence to death was 28 months (range: 0-129 months) and 5- year survival was 9% and 10- year survival was 5% [32]. Among 43 patients with parathyroid carcinoma reported by Wynne et al, two patients presented with neck mass and clinical symptoms included arthralgia (17%), weight loss (10%) and nephrolithiasis (7%) [33]. Cordero et al studied 10 cases of parathyroid carcinoma: the average age was 51 years-old, average serum calcium-14.3mg/dl, palpable mass-55%, bone disease-89%, renal disease-78%, capsular invasion-most common, local recurrence-55%, neck lymph node metastasis-11% and lung metastasis-11% [34]. More recently, eight cases of parathyroid carcinoma were reported: vascular invasion in 7/8 cases (87.5%), metastasis to lungs in 5/8 cases (62.5 %) and 2-year remission after surgery in 2/8 (25%) [30]. With
immunohistochemical staining, 6/8 (75%) was positive for CgA, 8/8 cases (100%) lost p27 and 6/8 cases (75%) lost Rb [30].
We had previously used a monoclonal anti-CgA from BioGenix, showing basically the same immunostaining with that of PTH immunostaining [14]. Yu et al also reported similar CgA immunostaining as our previous study [15] using the same monoclonal CgA antibody from BioGenix. Using the current CgA antibody from Dako System, CgA immunostaining was much less than that of PTH immunostaining with BioGenix ‘s antibody, supporting less CgA -containing secretory granules in the proliferative parathyroid lesions [14, 15]. Parathyroid lesions were not evenly immunostained particularly for CgA and SPY, and Yu et al used small tissue sampling of 0.6cm core tissues compared to our tissues, which measured 1.4x0.7cm in the average proliferative lesions. For SPY immunostaining, Yu et al and we used the same polyclonal antibody from Cell Marque, and Yu et al found less SPY immunostaining at 11% in parathyroid proliferative lesions [14]. We found no positive staining for SPY in normal parathyroid cells and positive immunostaining in 2 out of 13 adenomas and in 2 large cases of 8 hyperplastic glands at a total of 4 cases in 21 benign PHP at 19% (Tables 2 & 3). Two SPY-positive adenomas and two SPY-positive hyperplastic glands were larger than 1g in weight and 1.5x0.9cm in tissue section size, and it appears that only larger adenoma and hyperplasia may be immunostained for SPY.
PTH is packed and stored in the dense CgA-containing secretory granules [35]. To release PTH as a peptide hormone, secretory granules make a contact with plasma membrane (exocytosis) [1]. After co-secreting CgA with PTH (parathyroid secretory protein-1), CgA is recycled to the new cycle of hormone synthesis and secretion since a part of CgA is co-secreted into the blood with PTH, thus CgA modulates PTH secretion [1, 36, 37]. CgA and SPY are located in the different fine structures of the endocrine cells where SPY has been less immunostained than CgA in many neuroendocrine cells and their tumors [1, 15], and normal parathyroid chief cells are not immunopositive for SPY [14]. Synaptic vesicle protein 2 (SV2) was identified in humans, which demonstrated positive immunostaining for human gastrointestinal tract, pancreas, anterior pituitary, thyroid, adrenal medulla and parathyroid, the latter was weakly immunopositive to SV2 [38]. SV2 is a membrane glycoprotein found only in the secretory vesicles of neural and endocrine cells and belongs to the major facilitator superfamily of transport proteins [33]. CgA is located in the basic secretory granules while SPY immunostaining occurs diffusely in the cytoplasm outside the secretory granules, corresponding to the diffuse distribution of synaptic vesicles in the cytoplasm [1, 5, 39, 40]. Using the currently commercially available SPY antibody, all normal and the majority of hyperfunctioning parathyroid lesions are negative and this may suggest lesser significance of SPY in PTH synthesis and secretion in contrast to positive immunostaining in the majority of endocrine glands. Thus, function of SPY in parathyroids is unknown. SPY was the first synaptic protein cloned and is the most abundant synaptic vesicle protein, accounting for about 10% of the total synaptic vesicle protein [40, 41, 42, 43]. Presynaptic nerve terminals release neurotransmitters by synaptic vesicle endocytosis [44, 45, 46]. Yet, the functions of SPY in PTH synthesis and secretion remain unknown despite SPY being a reliable marker for other neuroendocrine tissues and their tumors.
Conclusion
Proliferative parathyroid lesions were less immunostained for PTH and CgA than normal PGs and this lesser CgA immunostaining was more characteristic for super-hyperfunctioning atypical adenoma and carcinoma. In parathyroid carcinoma, there were diffusely immunopositive PTH and less, partial CgA-staining in the eosinophilic cancerous cytoplasm. This diffuse PTH positive immunostaining in the cancerous tissue might distinguishes itself from benign proliferative lesions. Less CgA immunostaining represents less stored and ready to secrete PTH in the CgA secretory granules. Normal and the majority of proliferative PG lesions were not immunopositive for SPY, suggesting that SPY is not directly involved in synthesis and secretion of PTH.
Acknowledgement
A part of Immunohistochemical staining for CgA and SPY was performed in part at the Oregon Health and Science University Histopathology Shared Resources.
Declarations
Ethical Approval
All the autopsy and surgical pathology tissues were collected before the year 2000, and ethical approval was grandfathered before that time and would not be required or strictly enforced for this project. The materials presented in this study consisted of autopsy and surgical pathological tissues, which are not objected to the strict ethical approval at present compared to the clinical information.
Competing Interests
There are no competing interests regarding this work.
Author’s Contribution
I am the sole author of this manuscript and I have done every aspect of the work including cutting sections, immunostaining sections, photographing and writing manuscript.
Funding
This work was funded in part by the Oregon Health and Science University Endowment Fund 5413652F-13652.
Availability of Data and Materials
I was in charge of autopsy and surgical pathological materials used in this study at the University of Kansas Medical Center during my tenure and had access to the all the materials which I handled and signed out.
References
-
Ehrhart M, Gruse D, Bader MF, Aunis D, Gratzl M (1986) Chromogranin A in the pancreatic islets: Cellular and subcellular distribution. J Histochem Cytochem 34(12): 1673-1682.
-
Wiedenmann B, Franke WW, Kuhn C, Moll R, Gould VE (1986) Synaptophysin: a marker for neuroendocrine cells and neoplasms. Proc Natl Acad Sci USA 83(10): 3500-3504.
-
Klimstra DS, Modlin IR, Adsay NV, Chetty R, Deshpande V, et al. (2010) Pathology reporting of neuroendocrine tumors: application of the Delphic consensus process to the development of minimum pathology data set. Am J Surg Pathol 34(3): 300-313.
-
Ikeda K, Bekkers JM (2009) Counting the number of releasable synaptic vesicles in presynaptic terminal. Proc Natl Acad Sci USA 106(8): 2945-2950.
-
Jensen SM, Gadzar AF, Cuittita F, Russell EK, Linnoila RI (1990) A comparison of chromogranin, synaptophysin and L: Dopa Decarboxylase as members for neuroendocrine differentiation in lung cancer cell lines. Cancer Res 50(9): 6068-6074.
-
Duan K, Mete O (2016) Algorithmic approach to neuroendocrine tumors in targeted biopsies: Practical approach to immunohistochemical markers. Cancer Cytopath 124(12): 871-884.
-
Shoback D, Marcus R, Bikle D, Strewler G (2001) Cellular and extracellular calcium metabolism. In: Greenspan FS, et al. (Eds.), Basic & Clinical Endocrinology (Edn.), Graw- Hill NY, pp: 273-278.
-
DeLellis RA (2011) Parathyroid tumors and related disorders. Mod Pathol 24(3): s78-s93.
-
Carlson D (2010) Parathyroid pathology. Hyperparathyroidism and parathyroid tumors. Arch Pathol Lab Med 134(11): 1639-1644.
-
Digonnet A, Carlier A, Willemse E, Quiriny M, Dekeyse C, et al. (2011) Parathyroid carcinoma: A review with illustrative cases. J Cancer 2(10): 532-537.
-
Colin, PR, Fajitova, VT, Mortensen, RM, LeBoff MS, Brown EM (1989) Hysteresis in the relationship between serum ionized calcium and intact parathyroid hormone during recovery from induced hyper- and hypocalcemia in normal humans. J Clin Endocrinol Metab 69(3): 593-599.
-
Tomita T (2020) Significance of chromogranin A and synaptophysin in pancreatic neuroendocrine tumors. Bosn J Basic Med Sci 20(3): 336-346.
-
Tomita T (2021) Significance of chromogranin A and synaptophysin in medullary thyroid carcinomas. Bosn J Basic Med Sci 21(5): 535-541.
-
Yu Q, Hardin H, Chu YH, Rehrauer W, Lloyd RV (2019) Parathyroid neoplasms: Immunohistochemical characterization and long noncoding RNA (IncRNA) expression. Endocr Pathol 30(2): 96-105.
-
Tomita T (1999) Immunocytochemical staining patterns for parathyroid hormone and chromogranin in parathyroid hyperplasia, adenoma and carcinoma. Endocr Pathol 10(2): 145-156.
-
Weber CJ, Russel J, Chryssochos JT, Hagler M, McGarity WC (1996) Parathyroid hormone content distinguishes true normal parathyroid from parathyroid of patients with primary hyperparathyroidism. World J Surgery 20(10): 1010-1015.
-
DeLellis RA (1991) Parathyroid carcinoma. In: DeLellis RA, et al. (Eds.), Tumors of the parathyroid gland (Edn.), Armed Forces Institutes of Pathology, Washington DC, pp 53-63.
-
Habener JF, Stevens JD, Tregear CW, Potts JT (1976) Radioimmunoassay of human preparathyroid hormone: Analysis of hormone content in tissue extracts and in plasma. J Clin Endocrinol Metab 42(3): 520-530.
-
Nanes MS, OConner DT, Marx SJ (1989) Plasma chromogranin A in primary hyperparathyroidism. J Clin Endocrinol Metab 69(5): 950-955.
-
Bernini GP, Moretti A, Ferdeghini M, Ricci S, Letizia C, et al. (2001) A new chromogranin A immunoradiometric assay for the diagnosis of neuroendocrine tumours. Br J Cancer 84(5): 636-642.
-
Hogue J, Dixit D, Koh J, Koh J, Olson JA (2004) Functional and genetic studies of isolated cells from parathyroid neoplasm. Proc Natl Acad USA 111(8): 3092-3097.
-
Sh Y, Azimzadel P, Jamingal S, Wentworth S, Ferlitch J (2018) A polyclonal origin of parathyroid tumors is common and is associated with multiple gland disease in primary hyperparathyroidism. Surgery 163(1): 9-14.
-
Shi Y, Hogue J, Dixit D, Koh J, Olson JA (2004) Functional and genetic studies of isolated cells from parathyroid neoplasia. Proc Nat Acad Sci USA 111(8): 3092-3097.
-
Parsons BL (2008) Many different tumor types have polyclonal tumor origin: evidence and implications. Mutat Rev 659(3): 232-247.
-
Parsons BL (2018) Multiclonal tumor origin: Evidence and implications. Mutat Res Rev 777(1): 1-18.
-
Hahn WC, Weinberg RA (2015) Cancer: a genetic disorder. In: Mendelsohn J, et al. (Eds.), Basis of cancer (Edn.), Elsevier Saunders, Philadelphia, PA, pp: 3-17.
-
Machens A, Lorend K, Dralle H (2017) Parathyroid hormone levels predict long-term outcome after operative management of parathyroid carcinoma. Horm Metab Res 49(7): 485-492.
-
Erovic BM, Harris L, Jamali M, Irish JC, Asa SL, et al. (2012) Biomarkers of parathyroid carcinoma. Endocr Pathol 23(3): 221-231.
-
Duan K, Mete O (2015) Parathyroid carcinoma: Diagnosis and clinical implications. Turk Patholog Derg 31(Sup 1): 80-97.
-
Akirov A, Asa SL, Larouche V, Mete O, Sawka AM, et al. (2019) The clinicopathological spectrum of parathyroid carcinoma. Front Endocrinol 10: 731.
-
Erickson L, Mete O, Johlin CC, Perren A, Gill AJ (2022) Overview of the 2022 WHO classification of parathyroid tumors. Endocr Pathol 33(1): 64-89.
-
Sandlin K, Auer G, Bonderson L, Grimelius L, Farnebo LO (1992) Prognostic factor in parathyroid cancer: a review of 95 cases. World J Surg 16(7): 724-731.
-
Wynne AG, van Herden J, Carney JA, Fitzpatrick LA (1992) Parathyroid carcinoma: clinical and pathologic features in 43 patients. Medicine 71(4): 197-205.
-
Cordeiro AC, Montenero FL, Kulcsar MA (1998) Parathyroid carcinoma. Am J Surg 175(1): 52-55.
-
Harber JF, Rosenblatt M, Potts JT (1984) Parathyroid hormone: Biochemical aspects of biosynthesis, secretion, action and metabolism. Physiol Rev 64(3): 985-1003.
-
Coporale LH, Rosenblatt M (1986) Parathyroid hormone secretion: Molecular events and regulation. Nephrol 50(1): 73-95.
-
Taupenot L, Harper KL, O Conner DT (2003) The chromogranin-secretogranin family. N Eng J Med 348(12): 1134-1149.
-
Gomes GMP, Lukinius A, Grimelius L (2000) Synaptic vesicle protein 2, a new neuroendo-crine cell marker. Am J Pathol 157(4): 1299-1309.
-
Gomes, GMP, Strindsberg M, Johansson H, Grimelius L (1999) Co-localization of synaptophysin with different neuroendocrine hormones in the human gastrointestinal tract. Histochem Cell 11(1): 49-54.
-
Custer KL, Sustin NS, Sullivan JM, Bajjalieh SM (2006) Synaptic vesicle protein 2 enhances release probability at quiescent synapses. J Neurosci 26(4): 1303-1313.
-
Rizzoli SO, Betz WJ (2005) Synaptic vesicle pools. Nat Rev Neurosci 6(1): 57-69.
-
Janz R, Sudhof TC, Hammer RE, Unni V, Siegelbaum SA, et al. (1999) Essential roles in synaptic placidity for synaptophysin 1 and synaptophysin 1. Neuron 24(3): 687-706.
-
Leube RE (1994) Expression of the synaptophysin gene family is not restricted to neuronal and neuroendocrine differentiation in rat and human. Differentiation 56(3): 163-171.
-
Rizzoli SO (2014) Synaptic recycling: Steps and principals. EMBO J 33(8): 788-822.
-
Jahn R, Schlebler W, Ouimet C, Greengard p (1985) A 38,000-dalton membrane protein (p38) present in synaptic vesicles. Proc Natl Acad Sci USA 82(12): 4137- 4141.
-
Kwon SE, Chapman ER (2011) Synaptophysin regulates the kinetics of synaptic vesicles. Neuron 70(5): 847-854.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty