Therapeutic Clinical Implications of Crosstalk amongst Gut Microbiota, Bone Health and Vascular Calcification in Chronic Kidney Disease: A Narrative Review
Introduction
The gut microbiome in the human microbiome comprises of trillions of microorganisms inclusive of bacterial, viral, fungi as well as archae that are existent in a symbiotic association with the host at the time of a healthy status [1, 2]. The function amongst others is conferring protection against pathogens possessing the capacity of modulating the immune system along with control of endogenous metabolism of nutrients in association with life style factors [1]. With the escalating microbial DNA sequencing strategies variable microbial communities profiling in the gut has been made possible. This validates that despite intersubject variability, a parameter regarding its constitution is common exists [3]. The human gut microbiota (GM) comprises of greater than 1000 variable microbial species possessing specific properties [3]. Currently the phyla usually visualized are Firmicutes, Bacteroides, Actinobacterium Proteobacteria, Fusobacteria, Verrucobacteria. The initial 2 comprise 90% of GM [2]. Despite the GM constituents are believed to be stable at smaller periods, variability might take place at short as well as long duration exposure to factors like diet, medicines, ageing along with pathological situations [2, 3].
Escalating validation has illustrated that changes in GM (alias gut dysbiosis) might possess a central part in the pathogenesis of numerous diseases inclusive of Chronic Kidney Disease (CKD) [4]. CKD has assumed a considerable global public health problem with enhancing prevalence impacting greater than 850 million subjects globally [5]. General etiology of CKD are inclusive of type2 Diabetes mellitus, hypertension, glomerulopathies, tubulointerstitialnephritis subsequent to infections or exposure to nephrotoxic substances, besides others [5]. With the reduction in Kidney function in CKD manifestation of metabolic complications inclusive of anaemia, metabolic acidosis along with aberrations of bone as well as mineral metabolism take place [6, 7]. Aberrations of bone as well as mineral metabolism besides resulting in fractures [8] have further been correlated with an escalated risk of vascular calcification, cardiovascular complications along with mortality [9]. Uremia further facilitates the generation of imbalance amongst human intestinal microbiota causing an enhanced generation of toxic along with inimical actions like vascular along with renal disease propagation [10]. Despite the vascular calcification along with bone conditions in case of patients with CKD are usually believed to be possessing a common mode, just recently realization has dawned regarding GM might be a 3rd constituent impacting both vasculature as well as bone. Here the objective is to detail the growing proof regarding the association amongst cardiovascular system, gut, bone along with their inter correlation labelled as gut-bone- vascular axis in propagating CKD (Figure 1) [11] .
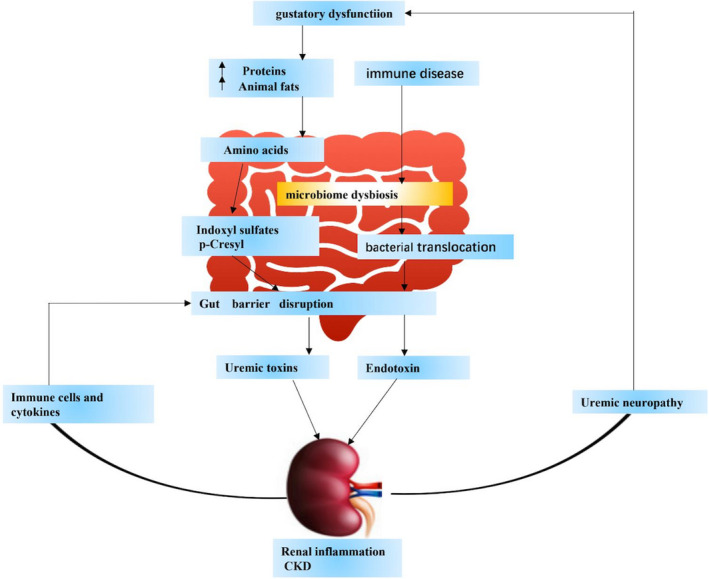
Figure 1 (courtesy ref no-11): The kidney plays an important role in nutritional homeostasis. Base on Chronic kidney disease causes kidney damage, Increased susceptibility to malnutrition injury. In CKD, a reduction in renal filtering capacity results in the deposition and accumulation of waste products in the blood, which eventually develops into uremia. In addition, complications of uremia include uremic neuropathy, which can contribute to gustatory dysfunction leads to an imbalanced diet. Dysbiosis caused by an imbalanced diet (for example, a diet high in protein and animal fat) leads to excessive production and accumulation of p‐cresol and indoxyl sulfate in the gut. This accumulation destroys the intestinal barrier, thereby increasing the permeability of the intestine. Therefore, it can cause kidney damage (like inflammation of the kidneys). Metabolite causes activation of immune cells and factors, and continuous destruction of the intestinal barrier.
Having reviewed earlier the role of epigenetic modifications in Diabetic Kidney Disease (DKD), role of various other etiologies of CKD besides Vitamin K &D in CKD, role of gut microbiota (GM) in obesity, type2 Diabetesmellitus (T2DM), non-alcoholic fatty liver disease(NAFLD)and utilization of probiotics for their treatment, normalphysiology of bone [12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24] we decided to conduct a narrative review regarding correlation of GM in CKD besides the association with bone health and mineral metabolism.
Methods
Here we conducted a narrative review utilizing search engine pubmed, google scholar; web of science embase; Cochrane review library utilizing the MeSH terms like CKD; GM: vascular calcification (VC); mineral along with bone disorders(MBD); VitaminK; TMAO; vascular smooth muscle cells(VSMC) Probiotics; Prebiotics; uremic toxins short chain fatty acids(SCFAs) from 1990’s till 2022 till date.
Results
We found a total of 800 articles out of which we selected 140 articles for this review. No meta-analysis was done.
Vascular Along with Mineral Bone Aberrations in CKD
Vascular Calcification
Besides the reduction in glomerular filtration rate (GFR), a systemic alteration takes place in mineral metabolism in case of patients with propagating CKD. Together these alterations are labelled as Chronic Kidney Disease- mineral along with bone disorders (CKD-MBD). CKD-MBD process the properties of one or greater aberrations in circulating minerals or their controlling hormones (like calcium, phosphate, PTH, VitaminD), bone aberrations along with vascular calcification [25].
CKD is correlated with escalated cardiovascular mortality that might be in part explained by vascular calcification in relation to CKD-MBD. Escalated dyscontrolling might be seen in extremely young dialysis patients which aid in inimical outcomes [26]. Vascular calcification represents an active considerably controlled cellular event with the calcium along with phosphate crystals getting deposited within the intima as well as media layer of vasculature along with/or heart valves [27]. Apart from well acknowledged canonical risk factors for vascular calcification(VC)like age, male sex, diabetes, dyslipidemia, hypertension, smoking along with inflammation, VC in CKD patients (from early states till subsequent to replacement treatment)gets stimulated by decontrolling of mineral metabolism [28], along with phenotypic alterations in vascular smooth muscle cells (VSMC) that reflects the first step in the pathological event labelled as osteochondrogenic differentiation along with apoptosis in VSMC [29]. Different facets of close modes in CKD stimulated vascular calcification further attribute towards the instability along with release of matrix extra cellular vesicles (ECV) possessing calcium along with phosphate from bone as well as VSMC besides elastin(protein with maximum enrichment of media wall) breakdown, facilitating calcium getting deposited [30]. Furthermore, an imbalanced milieu occurring secondary to mineral decontrolling results in dysfunctional actions of VC hampering agents(like pyrophosphates, adenosine, matrix Gla protein (MGP), osteopontin, fetuin, osteoprotegrin Klotho, Bone morphogenetic protein7 (BMP7), (magnesium), whereas escalating the actions of promoters(like proinflammatory cytokines, Oxidative stress (OS), osteocalcin, osteonectin, BMP2, Runx2, secondary calciproteins particles) [30, 31]. Decontrolling of numerous factors have been isolated along with associated with VC besides inimical clinical outcomes [32]. A recently conducted study in CKD patients with variations in degree of renal function have illustrated an aggravated expression of alkaline phosphatase along with Runx2 in VSMC of CKD patients that points to osteogenic differentiation [33]. The part of Wnt hampering agents like sclerostin along with DKK (dickopff) continues to be contradictory [34]. Intriguingly numerous of above detailed factors besides being implicated in vascular calcification, further control bone metabolism along with are responsible for bone aberrations in CKD (Figure 2 & 3).
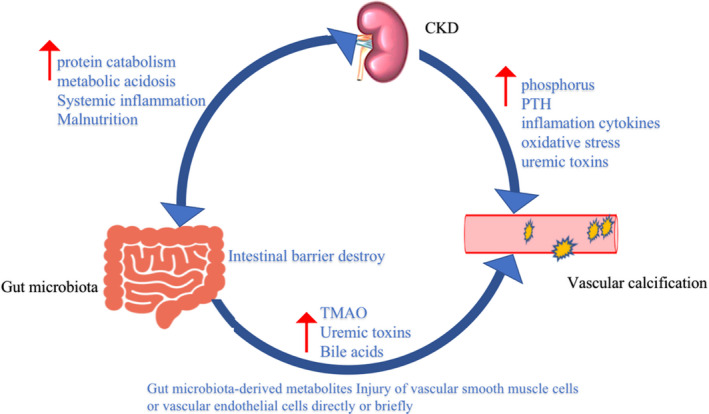
Figure 2 (courtesy ref no-11): In chronic kidney disease (CKD) patients, decreased renal function leads to decreased glomerular filtration rate (GFR), increased proteinuria and uremic toxins, and damage to glomeruli and tubulointerstitial. Also cause metabolic acidosis, accelerated protein catabolism, resulting in malnourished patients. Malnutrition also leads to an imbalance of intestinal homeostasis, which is characterized by increased mucosal inflammation, increased intestinal permeability and abnormally increased gut microbiota‐ derived metabolites like (p‐cresol, indoxyl sulfate and Trimethylamine N‐oxide (TMAO). It can directly or indirectly affect vascular smooth muscle cells or vascular endothelial cells and induce vascular calcification. And high phosphorus caused by chronic kidney disease, parathyroid hormone (PTH), inflammatory cytokines, oxidative stress and uremic toxins can induce vascular calcification.
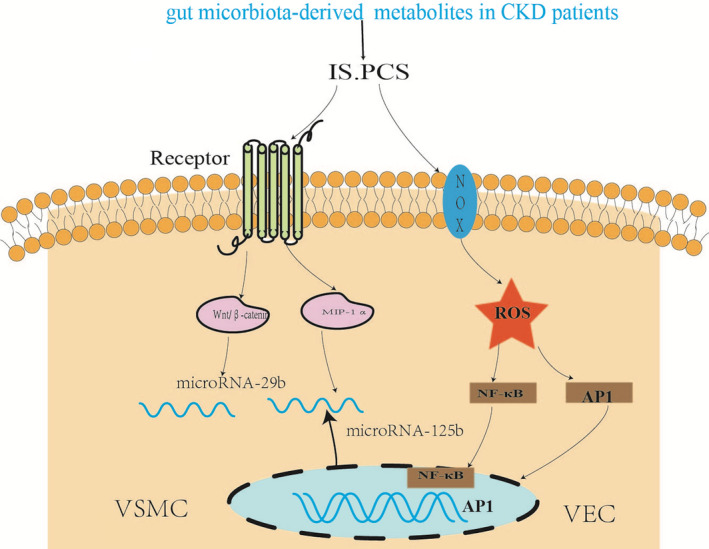
Figure 3 (courtesy ref no-11): Gut Microbial-Derived Metabolites in CKD Patients.
Bone Aberrations in CKD
CKD possesses a robust properties of escalated risk of fractures in CKD patients on dialysis displaying a risk from 1.5 - 8times in contrast to general population [35]. Over the span of 1992-2009, risk of fractures has escalated by 50.9% regarding hip along with vertebral fractures, as well as40.6% in arms and leg fracture which needed to be hospitalized as far as haemodialysis patients in United States are concerned [36]. An epidemiological study conducted further recently revealed that there was an inverse association amongst the estimated glomerular filtration rate (eGFR) along with risk of fractures incidence with an hazard ratio of 1.25(95%CI 1.05- 1.49) for eGFR <60ml/min/1.73m2, as well as 1.65(95%CI 1.14-2.37) for eGFR <45ml/min/1.73m2 [36]. Moreover, the action of reduction of eGFR on fractures incidence was more obvious in case of younger along with male patients [37]. Furthermore, haemodialysis patients who presented with a fracture possessed greater unadjusted ratios of mortality (3.7 times) along with mortality(/rehospitalized (4.0 times) in contrast to dialysis patients without a fracture [35]. The escalated risk of fractures has been observed amongst CKD patients subsequent to Kidney transplantation [38, 39]. In the initial 3 yrs post transplantation, the risk of hip fractures is 34% greater in contrast to dialysis patients along with25% will develop a fracture at a time span of 5yrs [39]. A meta- analysis which was conducted recently revealed that the total incidence rate of fractures was 8.95/1000person years amongst dialysis patients with Kidney transplant recipients (KTR) [38].
Vascular Calcification Along with Bone Disease in CKD-Is the Aetiology Common?
Shared formation of VC along with Bone disease in case of patients with CKD being common factors which stimulate these decontrolling pointed that there is a common aetiology. Escalated proof has revealed the copresence of both VC along with bone disease in CKD patients [40]. However, the modes associating aberrations in bone along with VC remains with no clarity. In view of bone matrix is possessing abundance of controlling factors which are further active in the vasculature as well like osteopontin along with MGP they might be liberated in the circulation at the time of bone getting resorped [41]. In the vascular tissues, cells possessing both osteoblastic along with osteoclastic capacity have been detailed as well as bone associated proteins have been isolated in calcified arterial damage [42]. There might be alternate factors implicated in vascular calcification along with bone depletion in CKD that is validated by the various risk factors shared by both conditions inclusive of Vitamin K along with D aberrations, chronic inflammation, dyslipidemia, hyperparathyroidism, hyperhomocystenemia, estrogen deficiency along with Oxidative stress (OS) [41]. The way detailed in the Kidney Disease Improving Global Outcomes (KDIGO) 2006 Guidelines these words CKD-MBD were referred not to just detail the syndrome regarding the bone along with biochemical aberrations seen in CKD but further be inclusive of extra skeletal calcification that takes place in these patients due to the disturbance in the complicated systems biology that is inclusive of Kidney, skeletal along with cardiovascularsystem [43].
Despite, no etiological association has been made definitively, CKD-MBD as well as specifically hyperphosphatemia, reflects one of the main stimulators of vascular calcification [30]. Hyperphosphatemia causes stimulation of both PTH along with Fibroblast growth factor23 (FGF23) generation which is followed by phosphaturia induction via an action on type2 renal Sodium dependentphosphate transporters [29, 30]. Nevertheless, aberrant quantities of PTH along with FGF23 might be correlated with vascular calcification even prior to the generation of hyperphosphatemia. escalted quantities of PTH along with FGF23 in CKD facilitate bone resorption, that might further escalate serum calcium– phosphate products in a vicious cycle [44]. VSMC‘s on exposure to a milieu rich in calcium as well as phosphate they go through osteogenic differentiation, along with transform to bone generating cells known as Osteoblast Chondrocytes like cells [29]. The injury contractile characteristic are depleted however they form a collagen matrix along with generate abundance of calcium – along with phosphate matrix vesicles, that in turn might start the mineralization of the wall of the vessels [29].
Simultaneously,a bone disease, dynamic in nature possessing the properties of considerable reduction in bone generation rate along with lesser quantities of PTH( lesser bone remodeling) might further be correlated with ectopic calcification of the vessels valves as well as heart [45]. Apparently osteochondrogenic differentiation of the VSMC is based on greater expression of type III Sodium dependent phosphate transporters (Pit 1 as well as Pit 2) thus aiding in vascular calcification in CKD-MBD. It is experimentally validated that anti-aging protein Klotho, a co-receptor that is applicable for classical FGF23 signaling, imparts anti calcification actions by induction of phosphaturia that preserves GFR along with a direct action as well on soft tissue inclusive of vascular smooth muscle [31]. Hence decontrolling of bone along with mineral metabolism might stimulate bone disease as well as vascular calcification in CKD. Simultaneously, extra factors like inflammation that is shared with CKD, along with elimination of Klotho [46] might have inimical actions on bone as well as vasculature (Figure 4) [47].
Figure 4 (courtesy ref no-47): IS enhances the CpG hypermethylation of Klotho and epigenetic modification of klotho to promote the process of VC in CKD and induced methyltransferase‐like (METTL14) ‐dependent N6‐methyladenosine (m6A) regulated vascular calcification in VSMC.TMAO activates endothelial cell mitogen‐activated protein kinase (MAPK) and vascular smooth muscle cell (VSMC) through nuclear factor‐κB (NF‐κB) pathway, leading to inflammatory gene expression and augmenting Ca2+ release from intracellular stores.
Inflammation: Stimulating Bone Disease Along with Calcification
In case of CKD, the existence of what is labelled as Uremic vascular microinflammation is, believed to be the hallmark of pathophysiological component which possesses a significant part in vascular calcification along with bone disease [48].
Already enough proof has been revealed that biomarkers of inflammation like IL-1β, IL-6 along with TNF-α possessed an inverse association with eGFR along with cystatin-C besides positively with albuminuria [49], as per a big cohort study, that pointed to a part of inflammation in the generation of CKD as well as propagation .The modes that associate inflammation with vascular calcification implicates numerous factors as well as are complicated .Multiple inflammatory modulators like C Reactive Protein(CRP) , Oxidative stress( OS), carbonyl stress along with cytokines might directly initiate vascular calcification. Furthermore, inflammation results in reduction of the calcification hampering agent like fetuin [50]. Significantly, the proinflammatory cytokines, TNF-α, receptor activator of nuclear kappa B ligand (RANKL) as well as IL-1 along with IL-17 further possess inimical actions on bone [51]. TNF-α impacts Osteoclastogenesis via direct actions on osteoclast precursors cells, whereas IL-6 possesses the capacity of upregulation of RANKL, hence indirect validate the generation of osteoclasts through crosstalk with mesenchymal cells [46]. In case of a histomorphometric study conducted by Viane, et al. [52], in end stage renal Disease(ESRD) patients illustrated that inflammatory markers like IL-6 as well as TNF-α possessed an independent correlation respectively with aortic calcification along with lesser bone area, highlighting the part of microinflammation in the bone-vascular axis in CKD .No clarification is present regarding the area of origin of chronic inflammation in case of numerous CKD patients, with numerous factors being implicated. Collecting proof pointed to the part of Gastrointestinal Tract (GIT) in the form of a main etiological factor regarding inflammation in CKD [53].
Role of Gut Microbiota in Chronic Kidney Disease
Both experimental in addition to Clinical proof pointed to a unique intestinal microbiota comprising the GM in CKD. A well acknowledged fact is the presence of a healthy, balanced colonic microbiota is basically made up of saccharolytic bacteria (alias bacteria that ferment carbohydrates) [3]. Regarding reduction of GFR, there is exposure of theintestines to uremia. Continuous exposure to escalated quantities of urea result in the overgrowth of urease possessing bacterial families [54], that are implicated in escalated ammonia formation, further enhancing intestinal pH . Furthermore in case of ESRD escalated quantities of uric acid along with oxalates liberation in the GIT in view of colon assuming the main excretion mode [4], which is responsible for enrichment of urease generating microbes [54]. These escalated proliferation of (uricase along with urease possessing species) result in gut dysbiosis generation. In a recently conducted systematic review it was illustrated that patients from any stage of CKD, varying from early GFR reduction to ESRD possessed a considerable variation in GM profile in contrast to normal healthy subjects [55]. Nevertheless, certain variation in GM profile amongst CKD populations can be observed. At the time of early CKD, certain spp of advantage like Ruminococcacea along with Lacnospiraacea, that are of abundancein the general population, possessing the capacity of breakdown of polysaccharides were seen [55]. With advancement of CKD the families correlated with the generation of uremic toxins are, believed to be greater, whereas there is reduction in families correlated with the generation of short chain fatty acids (SCFAs) [55]. These observations pointed that the microbiota in early CKD might be more intricate with that of healthy subjects in contrast to ones with advancement of CKD where gut dysbiosis is more prevalent.
The gut dysbiosis facilitated by the uremic microenvironment is implicated in the elimination of gut - barrier-intactness that in turn aids in translocation of live bacteria, endotoxin molecules (lipopolysaccharides) as well as gut obtained uremic toxins in the circulation [56]. The escalated exposure of the host to these constituents might cause activation of innate immunity along with systemic inflammation, ratio of enhanced intestinal CD4+T helper cells (Th17cells) than Foxp3+regulatory T (Treg) cells ends in a vicious cycle [57]. Furthermore, the proteolytic spp of abundance in CKD generate uremic toxins produced via protein fermentation in the intestine [58], inclusive of p-cresyl sulphate (P-CS), indoxyl sulfate (IS) along with trimethylamine-N-oxide (TMAO) [54], all possessing proinflammatory actions [58].Changes in the microbiota constitutionare inclusive of the microbial spp. that don’t possess the capacity of generating anti-inflammatory characteristics in addition to cytoprotective molecules like SCFA [54].
Besides uremia other factors aiding in the alterations in gut microbiota (GM) organization in case of CKD patients are diet along with medicines [59]. The major aspect of renal diet is protein restriction, whose objective besides preservation of renal function as well as reduction in the uremic toxins generation [59]. Furthermore, for the avoidance of hyperkalaemia as well as oxalates overload dietary Guidelines, advocated are inclusive of restriction of fruits along with vegetables ingestion, food grps possessing abundance of fibers, thus disturbance of symbiotic association in the GIT [60]. Rather than Concentrating on particular nutrients, certain authors conducted assessment of probable part of healthy dietary paradigms, like vegetarian as well as Mediterranean diet on GM arrangement in CKD [61, 62]. A crossectional study revealed that vegetarian haemodialysis patients possessed lesser quantities of P-CS as well as IS in contrast to omnivorous patients [61]. The greater fibers along with decreased quantities of animal proteins of a vegetarian diet might be implicated in the advantageous actions. Mediterranean diet possesses the characteristics of an attractive ratio of protein: carbohydrate consumption for GM, in view of it possessing whole grains, nuts, fruits along with vegetables with modest ingestion of fish along with dairy products as well as lesser consumption of redmeat. Despite, this dietary paradigms was unable to decrease the generation of uremic toxins in CKD- patients [62], it possess the capacity of escalating healthy GM components along with generation of SCFA in healthy individuals [59]. Chronic Intestinal constipation is another usual issue in CKD which impacts Intestinal microbiota [63].
CKD along with its usual correlated comorbidities result in polypharmacy (alias utilization of 5 or≥ medicationsdaily) in 80% of CKD patients [64]. Numerous agents have been implicated in alterations in GM arrangement [65, 66, 67, 68, 69, 70]. Like phosphate binders possess the capacity of influencing GM by resulting in dysfunctional Vitamin K as well as phosphate absorption [65]. Apart from influencing GM calcium dependent phosphate binders might escalate the risk of extra skeletal calcification via induction of escalation of serum calcium by decreased intestinal absorption of Vitamin K2. In a recent review inimical actions of Oral iron supplementation has been documented on GM, gut microbiome as well as intestinal health that might result in escalated formation of uremic toxins in CKD [67] the usual utilization of antibiotics by CKD patients, besides impacting the target pathogen, it influences commensal gut microbiota(GM) [66]. Proton pump hampering agents(PPIs)another kind of medicines utilized usually by CKD patients have been significantly correlated with alterations in gut microbiome in view of long timedecrease in gastric acid liberation besides hypochorhydria [68]. Lastly immunosuppression treatment subsequent to Kidney transplantation can result in considerable changes in GM organization [68, 69].
Intriguingly, decontrolling of GM might aid in vascular along with bone disease in case of CKD patients((the gut- vascular -bone-axis) amongst others via a metabolic switch from the mainly saccharolytic to a proteolytic fermentation paradigms, changed intestinal barrier function as well as dysfunctional Vitamin K status [70].
Gut- Vascular -Bone-Axis in CKD
Numerous factors aiding in gut aberrations connect vascular calcification along with bone disease are inclusive of) uremic (toxinsii) (TMAOiii) (Vitamin Kiv) SCFA.
Uremic Toxins
Uremic toxins p-cresyl sulfate(P-CS) as well as indoxyl sulfate (IS)get generated from the Intestinal microbial metabolism of tyrosine /phenyl alanine along with tryptophan respectively [10]. Subsequent to absorption from the colonicmucosa, they get conjugated with sulfate in the liver to P-CS as well as IS, that are either bound to albumin or circulating freely [10, 68]. In case of CKD the exacerbated microbial generation along with escalated intestinal permeability, both aid in the continued accrual of serum uremic toxins [68].
Canonical haemodialysis does not possesses the capacity of effective elimination of IS in view of greater binding capacity of albumin in plasma [71]. Greater quantities of P-CS as well as IS are correlated with exaggerated CKD propagation besides cardiovascular disease [72, 73]. At the time of CKD, plasma IS quantities are over 100 times of healthy subjects [74]. This aggravated quantities of plasma uremic toxins facilitates the generation of free radicals in renal cells along with VSMC via Oxidative stress( OS) as well as inflammation, resulting in tissue damage [11]. IS stimulates the expression of Osteoblast specific protein along with aortic wall calcification as well as thickening in Dahl-salt sensitive Hypertensive rats [75]. In agreement IS has been illustrated to facilitate a phenotypic shift of VSMC from contractile to Osteogenic phenotype [76]. IS quantities equivalent to those found in ESRD) patients possesses the capacity of causing proliferation of VSMC in rats was illustrated in an experimental Study [77]. In vitro P-CS might work in the form of a pro- osteogenic or pro- calcific toxins [78]. Significant escalation of aortic calcification along with calcification of peripheral arteries of rat was illustrated in a morerecent in vivo studywhere greater continued exposure to P-CS as well as IS took place [79]. Jing, et al. [80], illustrated that serum P-CS stimulated monocyte endothelial crosstalk in vitro via escalated generation of Reactive oxygen species (ROS). Furthermore, in vivo escalated P-CS quantities facilitated atherogenesis in 5/6 nephrectomized apoEL/L mice in contrast to controls [80]. Additionally, the activation of inflammation in addition to coagulation signaling pathways in aorta prior to calcification implied the involvement of these signaling pathways in toxins stimulatedarterial calcification [79].
Limited clinical studies have conducted an evaluation of correlation amongst uremic toxins along with vascular calcification in CKD. Baretto, et al. [73], revealed that a positive correlation existed amongst serum IS quantities as well as pulse wave velocity along with aortic calcification in variable stages of CKD, with IS wall acting as an anticipator of total in addition to cardiovascular mortality. Following that their group illustrated a correlation amongst P-CS as well as vascular calcification in CKD patients that pointed to P-CS quantities in the form of an anticipator of total along with cardiovascular mortality [72]. Rossi, et al. [81], observed a propagating escalated quantities of total in addition to free serum P-CS as well as IS in greater advancement of CKD stages [81]. Moreover total in addition to free serum P-CS as well as IS, possessed an independent correlation with structural as well as functional markers of cardiovascular disease like carotid intima -media-thickness (cIMT) as well as endothelial function [82]. Regarding haemodialysis (HD) patients P-CS quantities were correlated with higher carotid-femoral pulse wave velocity (PMW) which were apparently anticipator of greater arterial stiffness in patients of ESRD [82]. In agreement, study conducted a HD patients illustrated escalated quantities of P-CS in patients with carotid atherosclerotic plaque (CAP), revealed a positive association with greater total plaque area [80]. Lastly a huge cohort study of children with CKD further observed a Significant correlation existed amongst greater IS quantities with greater cIMT) as well as propagation of PMW, which was independent of other risk factors [83]. Significantly all these outcomes have been obtained from observational studies hence need further validation from human prospective studies.
Despite, limited knowledge existed regarding actions of uremic toxins on bone health in CKD the accumulated proof pointed towards IS might hamper osteoclast differentiation along with PTH signalling [84]. Moreover numerous In vitro studies have pointed that IS causes disturbance in the differentiation of mesenchymal stem cells(MSC’s) into osteoblasts, hampers proliferation of osteoblasts, bone mineralde position, alkaline phosphatase action as well as expression of bone associated genes [85]. Hirata, et al. [86], in a study conducted on parathyroid ectomized young adult rats, revealed that low bone turnover occurred secondary to IS [86], which might be a result of modes not associated with skeletal resistance to parathyroid hormone [87]. Treatment of MSC’s with escalated quantities of uremic toxins like P-CS or IS at the time of osteogenic differentiation facilitated down regulation of type 1 collagen, decreased alkaline phosphatase action as well as dysfunctional MSC’s mineral deposition [87]. These outcomes obtained emphasized that uremic toxins impacted osteogenesis negatively. It is well acknowledged that resistance to parathyroid hormone actions take place in the setting of CKD, despite the mode has not been worked out. NiiKono, et al. [88] illustrated that escalated quantities of serum IS facilitated PTH resistance in osteoblasts. In case of an experimental model of CKD IS along with other uremic toxins altered bone arrangement [89]. An inverse correlation existed in haemodialysis patients with alkaline phosphatase as well as with bone particular alkaline phosphatase disregarding intactness of PTH that pointed the involvement of IS in skeletal resistance [90]. Moreover, escalated quantities of IS facilitated 24 hydroxylase (CYP24A1) action that result in 25 hydroxy VitaminD as well as active VitaminD breakdown, decreasing, calcitriol(1, 25 di hydroxy cholecalciferol) quantities [91].
These observations pointed that patients with CKD might generate low bone turnover disease by direct actions of IS on osteoblast along with osteoclast precursors regarding suppression of bone generation along with bone resorption. Nevertheless, greater studies are required regarding unearthing the modes of uremic toxins in propagation of bone disease in case of uremia.
Role of Trimethylamine-N-Oxide (TMAO)
Trimethylamine-N-oxide(TMAO) gets obtained from trimethylamine (TMA ) possessing substrates like l-carnitine, choline along with betaine generated by intestinal microbiota [92]. These substances are present in different kinds of food & its products inclusive of those of animal initiation like red meat, egg, milk, fish, poultry besides those of plant origin like green vegetables, whole grains, spinach as well as beets [92]. TMA which gets generated by bacteria is absorbed effectively into the circulation along with is converted by hepatic enzymes like flavin mono oxygenase to TMAO [92].
In prior larger Clinical study, greater quantities of serum TMAO had been correlated with CVD [93] apart from facilitating atherosclerosis in case of rodents [94]. It is well acknowledged that patients with CKD possessing variable degrees of renal function have escalated generation of serum TMAO in view of changes in GM along with decreased renal function [93, 95]. A well fashioned study conducted recently implicating haemodialysis patients illustrated that greater quantities of serum TMAO were present in aortic calcification, in contrast to those without aortic calcification as well as positive correlation among serum TMAO quantities as well as aortic calcification scores [96]. In case of cultured VSMCs TMAO facilitated calcium -phosphate stimulated calcification along with in an animal CKD model TMAO facilitated vascular calcification [96]. Moreover, Zhang, et al. [96], further illustrated that TMAO facilitated vascular calcification besides osteogenic differentiation by activation ofNLRP3(nucleotide-binding domain, leucine-rich-repeat containing family, pyrin domain-containing 3inflammasome along with NF-Κb ( nuclear factor-kappaB) signaling pathways [96].
TMAO ‘s part regarding bone health was evaluated recently in addition to in age associated osteoporosis [97], along with type2 diabetes mellitus (T2DM) [98], however outcomes obtained from the patients with CKD were missing at present. Intriguingly in vitro treatment with TMAO facilitated adipogenic differentiation along with hampered osteogenic differentiation of bone marrow mesenchymal stem cells (BMMSCs) by up regulation of NF-κB signaling pathway [99]. This emphasized the significance of assessment of part of GM in CKD patients on quantities of serum TMAO along with if it affects vascular calcification as well as bone health. Furthermore Yin, et al. [11] illustrated that TMAO activated endothelial cell mitogen activated protein kinase (MAPK) along with VSMC via NFκB pathway that resulted in inflammatory gene expression as well as escalated Ca2+ liberation from intracellular stores (Figure 5).
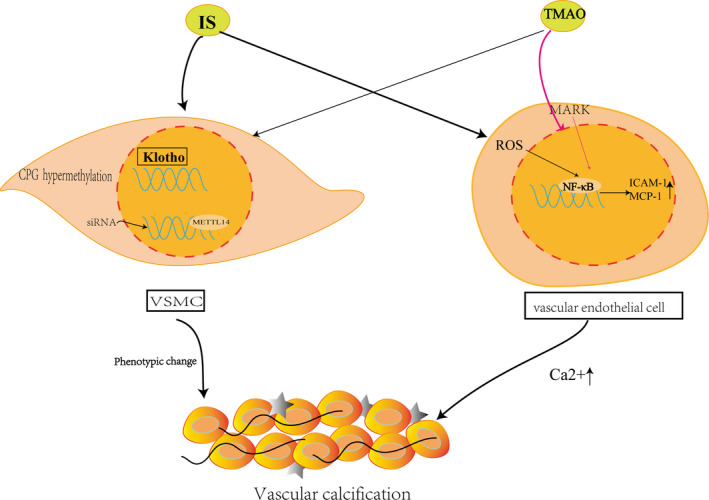
Figure 5 (courtesy ref no-11): IS enhances the CpG hypermethylation of Klotho and epigenetic modification of klotho to promote the process of VC in CKD and induced methyl transferase‐like (METTL14) ‐dependent N6‐methyladenosine (m6A) regulated vascular calcification in VSMC.TMAO activates endothelial cell mitogen‐activated protein kinase (MAPK) and vascular smooth muscle cell (VSMC) through nuclear factor‐κB (NF‐κB) pathway, leading to inflammatory gene expression and augmenting Ca2+ release from intracellular stores.
Role of Vitamin K
Vitamin K represents a fat soluble Vitamin which possesses a part in bone metabolism along with vascular calcification with its deficit is usually present in CKD patients [100]. Furthermore, subclinical Vitamin K deficiency is seen in patients with CKD [101], which corroborated the significance of escalated risk of vascular calcification as well as bone demineralization [102]. It is present in 2 isoforms namely VK 1 or phylloquinine (PK), Vitamin K2 (VK2) or generally known as menaquinone (MK). PK is usually generated by plant as well as seen in green leafy vegetables whereas MK gets formed by bacteria generally in present in yogurt besides other fermented food products as well as generated by bacteria [103]. The bacterial MK existing in the colon are basically MK10 as well as MK11 generated by Bacteroides, MK 8 by Enterobacteri_a_ MK 7 by Veillonell_a_ along with MK 6 by Eubacterium lentum [104]. Despite, the dietary PK in vegatables represents the major sources of the VK 2 consumption (80-90%), only 5-10% gets absorbed, while 10-25% is obtained from MK [105]. Still certain Authors belief is that considerably lesser quantities of VK 2 obtained from intestinal microbiota might significantly impact health [106].
Diets possessing lesser quantities of potassium (like reduced green leafy vegetables that has abundance of VK 1) along with lesser quantities of phosphate (like reduced dairy products that has abundance of VK 2) advocated in patients with CKD, hence reflect probable etiology of Vitamin K deficiency [60]. Other than dietary factors along with utilization of medicines like Vitamin K antagonists as well as phosphate binders [107], GM changed organization in case of CKD patients might further be implicated in being inimical regarding Vitamin K deficiency in thispopulation. A recently conducted study case of with Crohn’s disease revealed that there is decreased gut bacterial organization in Vitamin K deficient patients [106]. A well fashioned study conducted recently has illustrated that mice with interference in microbiota demonstrated, moderate enrichment of microbialgene implicated in Vitamin K formation [108]. Additionally, interference with gut microbiome was correlated with reduced crystallinity along with reduction in bone strength [108]. The probability of GM organization in correlation with Vitamin K status in CKD setting needs greater assessment.
VK dependent proteins (VKDPs) inclusive of osteocalcin (OC), along with matrix Gla protein [MGP] are significant controllers of bone mineralization [109]. Osteoblasts are the only generators of OC, whose binding takes place with calcium ions as well as hydroxyapatite crystals that has a controlling impact on bone mineral metabolism [110]. MGP is generated by VSMCs as well as chondrocytes for avoidance of ectopic calcification [100, 101, 102, 103, 104, 105, 106, 107, 108, 109]. Decreased serum quantities of carboxylated MGP is apparently implicated in the generation along with propagation of vascular calcification [110]. Moreover, on stimulation of the xenobiotic receptor on osteoblasts, Vitamin K possesses the capacity of changing bone mineral events [111] with the knowledge that Vitamin K is necessary regarding functionalization of a cascade of proteins inclusive of OC’s the non-collagen protein in bone matrix having maximum enrichment [111], the absence of bone OC escalates its fragility in addition to proneness to fractures [111]. Decreased consumption of Vitamin K along with functional Vitamin K deficiency as estimated by circulating markers like plasma dephosphorylated uncarboxylated matrix Gla protein(dp-ucMGP) or undercarboxylated OC(unOC)are correlated with lesser Bone mineral density (BMD) along with escalated fractures risk in general population [112] in addition to patients with CKD [113]. In an observational study where assessment of influence of Vitamin K in haemodialysis patients on vascular calcification as well as bone health was done revealed that Vitamin K1 deficiency was the maximum robust anticipator of vertebral fractures, while MK -4 deficiency of aortic calcification, along with MK -7 deficiency of iliac calcification [113].
Various studies observed a positive correlation amongst vascular calcification as well as Vitamin K deficiency [102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114]. In a recently conducted cohort study on ESRD patients, it was illustrated that dp-uc MGP possessed a robust correlation with coronary artery calcium (CAC) as well as aortic valve calcium; nevertheless in a stepwise regression assessmentit was demonstrated that dp-uc MGP was not an independent anticipator of vascular calcification. Simultaneously, a randomized controlled trial illustrated that supplementing 12mths of Vitamin K2 did not enhance vascular calcification in non-dialysis patients [115]. These observations pointed that a complicated, unresolved crosstalk amongst Vitamin K deficiency, bone disease along with vascular calcification exists in CKD. Six randomized controlled trials are ongoing for assessment of actions of Vitamin K supplementation in haemodialysis patients [116].
Role of Short Chain Fatty Acids (SCFA)
In the colon certain bacterial spp possess the capacity of fermenting lot of nutrientslike indigestible carbohydrates inclusive of dietary fibers along with resistant starches like polysaccharides to form short chain fatty acids (SCFA) [117]. SCFA are implicated in the 2-10% of the full energy utilization in humans that work in the form of provision of energy to colonic epithelial cells along with microbiota) [117]. SCFA which have maximum enrichment are inclusive of acetate, propionate as well as butyrate, whose generation takes place maximum via Firmicutes as well as Bacteroides that have fast absorption taking place from the intestinal epithelial cells via particular transporters or diffusion [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117]. The advantages of SCFA are not restricted tointestine, the site of their formation [118]. SCFA, apparently aid in the enhancement of vascular phenotype [11]. Certain studies have illustrated immunomodulatory ability of SCFA.Inflammatory cells like neutrophils macrophages, dendritic cells, as well as Tcells possesses the capacity of response to SCFA treatment, in agreement with their anti-inflammatory actions in broad variety of along with decrease vascular calcification [119], despite restricted studies on this issue.
Accumulating proof corroborated the advantageous actions of SCFA on bone health [129, 30]. Mice receiving treatment with SCFAx8wks illustrated significant enhancement of bone mass along with conferred protection from pathological bone depletion [129]. Lucas, et al. [120], further evaluated diet with greater quantities of fibers that escalated SCFA quantities in caecum along with serum on bone health. They observed this diet aided in enhanced bone mass. Zhou, et al. [121], have revealed a direct correlation amongst dietary fiber ingestion along with BMD basically in men in addition to those enroled possessing lesser genetically estimated GM- obtained SCFA propionate [121].
GM- in case of CKD patients possesses the properties of greater enrichment of spp possessing proteases in contrast to spp possessing enzyme implicated in the breakdown of fibers for production of SCFA, apart from lesser dietary fiber ingestion in view of renal diet advocated [56]. Serum butyrate quantities were 3 times lesser in Chinese CKD patients in contrast to healthy controls [122]. Furthermore, an inverse correlation was observed amongst butyrate as well as renal function [122]. Nevertheless, Terpstra, et al. [123] did not observe decreased quantities of butyrate generating spp nor in butyrate generating ability in a study of Dutch CKD patients sample, however they did not estimate full SCFA quantities. Hence, despite SCFA might be another correlate in Gut- vascular - bone-axis, its significance in CKD requires future evaluation. Moreover Rysz, et al. [47], emphasized how we find beneficial actions of Sodium – glucose co-transporter 2(SGLT2) cangliflozin treatment in CKD patients by reduction of quantities of uremic toxins (by hampering SGLT2 but probably SGLT1 as well) to change intestinal metabolites in an animal model. Furthermore this finding might be correlated with escalated quantities of SCFA as well as changed GM organization [47] (see figure 6).
Role of Epigenetic Modifications & miRNAs
Yin, et al. [11], further illustrated that IS escalated the CpG hypermethylation of Klotho in addition to epigenetic modification of klotho to facilitate the event of VC in CKD along with stimulated methyltransferase‐like (METTL14) ‐ dependent N6‐methyladenosine (m6A) controlled vascular calcification in VSMC. They further highlighted the part of miRNAs in these events (see figure 5).
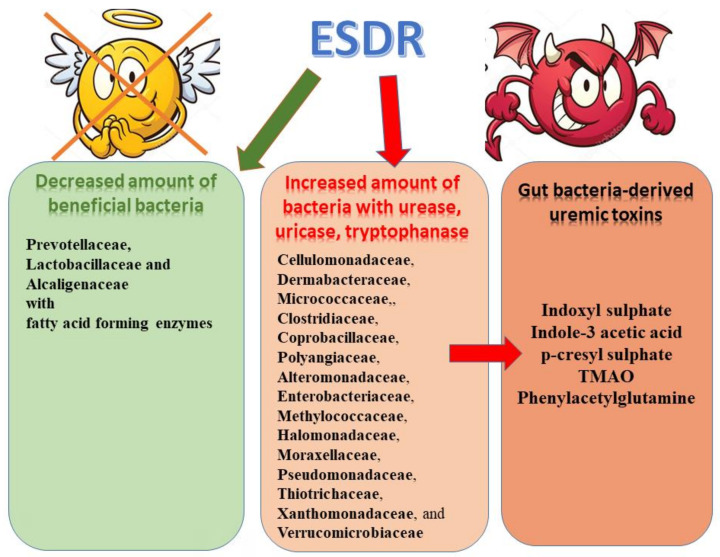
Figure 6 (courtesy ref no-47): Microbiome alterations observed in ESRD patients and uremic toxins.
Treatment Options
Personalized strategies with the aim of regeneration of a symbiotic association of GM with the host in case of CKD patients might be of advantages in Gut- vascular - bone-axis in CKD, thus aiding in amelioratation of vascular calcification as well as Bone mineral disease. For achieving this dietary manipulation. basicaly by escalating dietary fiber ingestion, Probiotics, Prebiotics as well as symbiotic delivery, Vitamin K supplementation where essential. The definition recognized by Food and Agricultural Organization of the United Nations (FAO) and world health organization (WHO) working group experts is that probiotics are live strains of strictly selected microorganisms, which once administered in adequate amounts, give a health benefit to the host [124]. Currently there is no availability of studies evaluating Probiotic, Prebiotics as well as symbiotic delivery, on vascular calcification as well as bone health in CKD patients. Nevertheless, a randomized controlled trial conducted recently illustrated that 3months of fructoligosacharides (FOS) supplementation had no impact on arterial stiffness, however decreased quantities of IL-6, besides preservation of endothelial function in case of patients possessing endothelial injury [125].
Moreover, certain studies pointed that decrease in uremic toxins generation took place in reaction to Probiotics in experimental along with clinical CKD studies attenuated biomarkers of inflammation along with OS [126]. Conversely, Borges, et al. [127], in a double blind, randomized placebo controlled trial where was done observed escalated quantities of IS subsequent to 3mths of Probiotic supplementation, that might be in view of escalated gut barrier permeability .These observations emphasized the need for greater assessment of use of Probiotics treatment in CKD patients that has to be done judiciously currently. Prebiotics, indigestible carbohydrates which work by impacting growth as well as action of advantageous bacteria with decrease in uremic toxins along with inflammatory biomarkers [128]. Conversely, in non- dialysis CKD patients, FOS supplementation did not impact uremic toxins quantities [129]. Similarly symbiotics, which by definition is a combination of Probiotics as well as Prebiotics, resulted in reduction in serum P-CS quantities in CKD patients [126].
Intriguingly, AST 120 an orally delivered spherical adsorbent that has received approval for utilization in CKD patients in Japan along with Asia possesses the capacity of hampering the hepatic generation of indoxyl sulfate by hampering the GIT absorption of indol as illustrated in an experimental study Armani RG, et al. [130]. Furthermore, significant reduction in serum P-CS quantities occurred in an animal model by AST 120 [131]. Moreover, in mice with adenine stimulated Kidney injury on receipt of AST 120 did not possess fecal p-cresol amounts. Additionally, AST 120 decreased the enrichment of Erysipelotrichcacea uncultured Clostridium sensustricto implicated in generation of p-cresol [132]. These preclinical human studies have laid the foundation for clinical studies in humans. A study to start with revealed that AST 120 reduced serum indoxyl sulfate quantities in a dose based fashion in patients with moderate to severe CKD [133]. Subsequently a study conducted more recently, a huge multinational randomized controlled trial to our misfortune did not illustrate any advantageous action of AST 120 on propagation of CKD [134]. A study still continuing has the objective of assessment of Probiotics in addition to oral adsorbents on vascular function in CKD patients [135]. In to certain studies have illustrated advantageous actions of attempting facilitation of gut health regarding intermediate endpoints, whereas other studies have illustrated nil actions or safety aspects as well. This emphasizes the need for greater studies for discovering efficacious therapies, besides identification of particular target (sub-) populations in addition to illustrate actions clinically significant (cardiovascular along with bone) results.
Conclusions Along With Future Directions
Thus CKD along with gut dysbiosis possess similar aberrations of factors which facilitate. Despite, a crosstalkis present amongst gut microbiota (GM), bone health, along with VC (Figure 7), maximum studies have concentrated on correlation amongst 2 of these factors however have not evaluated them together. Thus lot of insight regarding these pathways that associate GM, bone health, along with VC. Hence greater well fashioned cohort studies are required to be conducted for assessment of microbiome arrangement in relation to both bone disease along with VC in case of CKD setting.
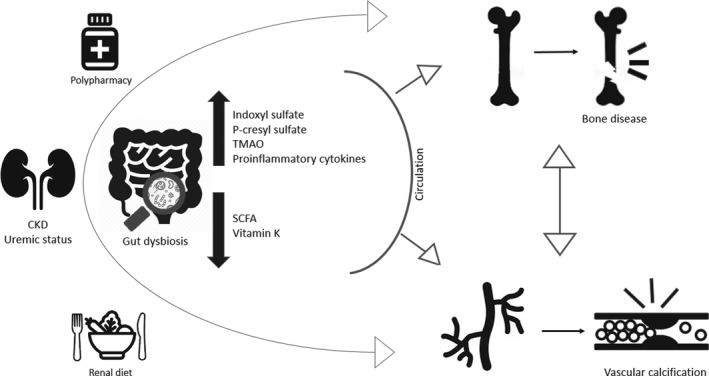
Figure 7: The uraemic milieu is one of the main contributors for gut dysbiosis in CKD. As renal function declines, the colon replaces the kidney as the primary site of excretion of urea and uric acid, which become alternative substrates for the gut bacteria, instead of indigestible foods, example fruits and vegetables) and polypharmacy (ie; phosphate binders, antibiotics, iron supplementation, PPI, immunosuppressants) may account for altered gut dysbiosis in CKD setting. The hypothesis upon gut-vascular-boneaxis in CKD revolves around the augmented exposure of the referred tissues to uremic toxins, such as indoxyl sulphate (IS) and p-cresylsulphate (P-CS), TMAO (Trimethylamine-N-oxide) and pro-inflammatory cytokines given the presence of a disrupted intestinal barrier. In addition, the reduced production of SCFA (short-chain fatty acids) and the deficiency of vitamin K might also exacerbate this mechanism.
Furthermore, a query arises if attempt is made to rectify this GM, does bone health along with VC do these factors get corrected in CKD. The absence of probable, practical approaches for assessment of alterations in gut microbiome at a time duration at the time of a Clinical trial. Whereas significance of assessment of dietary along with Probiotics/ Prebiotics supplementation therapy regarding manipulation of gut microbiota in case of CKD patients with the objective of assessment of their influence over gut metabolites (like of uremic toxins, TMAO, SCFA) it would be further of significance to concentrate on biomarkers of bone disease/ vascular disease such as fractures risk along with risk of CAC. For that Silva, et al. [136], have generated a fast high performance liquid chromatography (HPLC) for determination of protein bound uremic toxins, basically p-cresyl sulphate (p-CS), Indoxyl sulphate (3-INDS) indole-3-acetic acid (3- IAA) along with p-cresol (p-C) & phenol (Pol) [136] that is sustainable. Furthermore, present outcomes apparently point towards heterogenous effectiveness of any intervening treatments which aim towards improvement of gut health with regards to intermediate results like uremic toxins identification of subgroups of patients having proneness to positive treatment reaction would be of utmost importance Recently Ebrahim, et al. [137], conducted a randomized controlled trial β-Glucan Prebiotic supplementation with the observation of significant reduction in plasma free3- INDS quantities at varying time durations like at 8wks free3- INDS(p=0.03), as well as 14wks(p<0.001)free p-CS(p=0.006) at14wks along with total as well as free p cresyl glucuronide (PCG) (p<0.001,p<0.001, respectively along with at14wks. No variations in comparative enrichment of genera amongst groups was observed on entero typing of the populations just 2 of the four enterotypes namely Bacteroides 2 as well as Prevotella were observed. On redundancy assessment just occasional factors impacted gut microbiome, which were inclusive of triglyceride quantities(p<0.001), body mass index( BMI) (p=0.002).Thus concluding that β-Glucan Prebiotic significantly changed quantities of uremic toxins along with facilitated formation of advantageous gut microbiome. Shamloo, et al. [138], have further planned A randomized double blind, cross over trial to study the effects of resistant starch prebiotic in Chronic Kidney Disease (Re SPECKD) trial where 36 patients will be enrolled for a26week regimen with ingestion of 2sachets daily possessing 15 g of resistant potato starch(MS Prebiotic RPS) treatment or 15g corn starch (Amioca TF, digestible controls). Assessment of alterations in uremic toxins would be the primary outcomes .secondary outcomes would comprise of RPS ingestion on symptoms, quality of life (QOL) along with enrichment of, variations in addition to working capacity of gut microbiom [138].
References
-
Eckburg PB, Bik EM, Bernstein CN, Purdom E, Dethlefsen L (2005) Diversity of the human intestinal microbial flora. Science 308(5728): 1635-1638.
-
Rinninella E, RaoulP, Cintoni M, Franceschi F, Gasbarrini A (2019) What is the healthy gut microbiota composition? A changing ecosystem across age**,** environment, diet and diseases. Microorganisms 7(1): 14.
-
Jandhyala RM, Talukdar R, Subramaniam C, Vuyyuru H, Sasikala M, et al. (2015) Role of the normal gut microbiota. World J Gastroenterol 21(29): 8787-8803.
-
Vaziri ND, WongJ, Pahl M, Piceno YM, Yuan J (2013) Chronic Kidney Disease alters intestinal microbial flora. Kidney Int 83(2): 308-315.
-
Jager KJ, Kovesdy C, Langham A, Rosenberg M, Jha CV et al. (2019) A Single number for advocacy and communication. Nephrol Dial Transplant 34(11): 1803- 1805.
-
Chen TK, Knicely DH, Grams MF (2019) Chronic Kidney Disease diagnosis and management: A review. JAMA 322(12): 1294-1304.
-
Levey AS, Coresh J (2012) Chronic Kidney Disease. Lancet 379(8811): 165-180.
-
Graciolli FG, Neves KR, Barreto F, Barreto DV, Canziani ME (2017) The complexity of Chronic Kidney Disease: mineral and bone disorders across stages of Chronic Kidney Disease. Kidney Int 91(6): 1436-1446.
-
Bangalore S, MaronD, O’Brien SM, Fleg JL, Briguori C (2020) Management of coronary disease in advanced Kidney Disease. N Engl J Med 382(17): 1608-1618.
-
Vanholder R, Schepers E, Pietinck A, NaglerEV, Glorieux G (2014) The Uremic toxicity of indoxyl sulfate and p-cresyl sulfate:a systematic review. J Am Soc Nephrol 25(9): 1897-1907.
-
Yin L, Li XX, Ghosh S, Xie C, Chen J, et al. (2021) Role of gut microbiota derived metabolites on vascular calcification in CKD. J Cell Mol Med 25(3): 1332-1341.
-
Kaur KK, Allahbadia GN, Singh M (2021) Potential role of Epigenetic Modulation in prevention or therapy for Diabetic Kidney Disease-still a dream or a reality –A Systematic Review’’. J Diab Nephro Diab Mgmt 1(1-26).
-
Kaur KK, Allahbadia GN, Singh M (2022) An Update on the Approaches of Avoidance of Propagation of Chronic Kidney Disease resulting in Reversal or Prevention of Kidney transplantation-A Systematic Review. J Clini Nephrol 6: 40-57.
-
Kaur KK, Allahbadia GN, Singh M (2022) An update on Etiology of Chronic Kidney Disease with Role of Associated Vitamin K deficiency in Prevention of Vascular Calcification & Cardiovascular Risks & Avoid Mortality: A minireview. Acta Scientific Nutritional Health 6(5): 1-10.
-
Kaur KK, Allahbadia GN, Singh M (2021) Can Vitamin D Supplementation Prevent / Delay/ Halt the Progression of Diabetic Nephropathy; A Systematic Review on Mechanism of Vitamin D Crosstalk with Vitamin D Receptor, with others like Megalin-Cubilin and Amnioless Complex Along with FGF23-Klotho Complex. Published in J Clin Diabetes Obes.
-
Kaur KK, Allahbadia GN, Singh M (2019) Have Probiotics and Synbiotics passed the test of time to be Implemented in Management of Obesity and Related Metabolic Disorders-a Comprehensive Review. Adv Obes Weight Manag Control 9(1): 21-28.
-
Kaur KK, Allahbadia GN, Singh M (2020) Will Probiotics Provide the Answer for Therapy of Non-alcoholic Fatty Liver Disease (NAFLD)? A Systematic Review. Biochem Physiol 9(1): 257.
-
Kaur KK, Allahbadia GN, Singh M (2018) Weight Loss Associated with High Protein Diet Intake in Obesity: Interactions of Gut Microbiota in Protein Sources Influencing this Positive Effect. Acta Scientific Nutritional Health 2(7): 80-89.
-
Kaur KK (2020) Advantages and Limitations of Utilizing Clostridium Species as Probiotics-A Sytematic Review. Transcriptomics S2: 3.
-
Kaur KK, Allahbadia GN, Singh M (2020) The Association of Dietary Fatty Acids and Gut Microbiota Alterations in the Development of Neuropsychiatric Diseases: A systematic Review. Obesity Research Open Journal 7(1): 19-45.
-
Kaur KK, Allahbadia GN, Singh M (2020) Intestinal Immune System in the Regulation of Obesity and Metabolic Syndrome-Therapeutic Implications-A Systematic Review. EC Clinical and Experimental Anatomy 3(7): 07-22.
-
Kaur KK, Allahbadia GN, Singh M (2022) An Update on the Association of Gut-Liver Axis with Gut Microbiome Dysbiosis Correlated NAFLD along with NAFLD-HCC with Potential Therapeutic Approaches: A systematic Review. J Hepatol Gatroenterol.
-
Kaur KK, Allahbadia GN, Singh M (2020) Normal Anatomy of the Human Skeleton with Factors Modifying its Development as Well as Regeneration. EC Clinical and Experimental Anatomy 3(11).
-
Kaur KK, Allahbadia GN, Singh M (2020) The association of dietary fatty acids and gut microbiota alterations in the development of neuropsychiatric diseases: A systematic review. Obes Res Open J 7(1): 19-45.
-
Bover J, Urena-Torres P, Mateu S (2020) Evidence in Chronic Kidney Disease - Mineral and Bone Disorders Guidelines: is it time to Treat or Time to Wait? Clin Kidney J 13(4): 513-521.
-
Henaut L, Chillon JM, Kamel S, Massy Z (2018) Updates on the Mechanism and the Care of Cardiovascular Calcification in Chronic Kidney Disease. Seminal Nephrol 38(3): 233-250.
-
Evenepoel P, Opdebeck B, David K, Hasse PC (2019) Bone-Vascular Axis in Chronic Kidney Disease. Adv Chronic Kidney Dis 26(6): 472-483.
-
Sotomayer CG, te VelderKayzer CA, De Borst NH, Navis GJ, Bakker SH (2020) Lifestyle, Inflammation and Vascular Calcificationin Kidney Transplant Recipients: Perspectives on Long-Term Outcomes. J Clin Med 9(6): 1911.
-
Paloian NJ, Giachelli CM (2014) A Current Understanding of Vascular Calcification in CKD. Am J Physiol Renal Physiol 307(8): F891-F900.
-
Yamada S, Giachelli CM (2017) Vascular Calcification in CKD-MBD: Roles for Phosphates, FGF23 and Klotho. Bone 100: 87-93.
-
Hu MC, Shi M, Zhang J, Quinones H, Griffith C, et al. (2011) Klotho Deficiency Causes Vascular Calcification in Chronic Kidney Disease**.** J Am Soc Nephrol 22(1): 124- 136.
-
Chen J, Budoff MJ, Reilly MP, Yang W, Rosas SE, et al. (2017) Coronary Artery Calcification and Risk of Cardiovascular Disease and Death Amongst Patients with Chronic Kidney Disease. JAMA Cardiol 2(6): 635-643.
-
Chang JF, Liu SH, Lu KC, Ka SM, Hsieh CY, et al. (2020) Uremic Vascular Calcification is Correlated with Oxidative Elastic Lamina Injury, Contractile Smooth Muscle Cell Loss, Osteogensis and Apoptosis: The Human Pathobiological Evidence. Front Med 7: 78.
-
Klingenschmid G, Tschiderer L, Himmler G, Rungger G, Brugger S, et al. (2020) Associations of Serum Dickopff-1 and Sclerostin with Cardiovascular Events: Results from the Prospective Brunek Study. J Am Heart Assoc 9(6): e014816.
-
Tentori F, Mc Collough K, Kilpatrick RD, Bradbury BD, Robinson BM, et al. (2014) High Grade Rates of Death and Hospitalization follow Bone Fractures Among Haemodialysis Patients. Kidney Int 85(1): 166-173.
-
Wagner J, Jhaveri KD, Rosen L, Sunday S, Mathew AT, et al. (2020) Increased Bone Fractures Among Elderly United States Haemodialysis Patients. Nephrol Dial Transplant 29(1): 146-151.
-
Dsbiens LC, Goupil R, Madore F, Mac-Way F (2014) Incidence of Fractures in Middle-Aged Individuals with Early Chronic Kidney Disease: A Population**-**Based Analysis of CARTaGENE. Nephrol Dial Transplant 35(10): 1712-1721.
-
Tan J, Li Y, Wu Z, Zhao J (2018) Risk of Hip Fractures in Patients on Dialysis or Kidney Transplant: A Meta- Analysis of 14 Cohort Studies. Ther Clin Risk Manag 14: 1747-1755.
-
Bali AM, Gillen DL, Weiss NS, Emerson SS, Seliger SL, et al. (2002) Risk of Hip Fracture Among Dialysis or Renal Transplant Recipients. J Am Med Assoc 288(23): 3014- 3018.
-
Sotomayer CG, Benjamens S, Gomes-Neto AW, Pol RA, Groothelof D, et al. (2021) Bonemineral density and Aortic Calcification: Evidence for Bone-Vascular Axis After Kidney Transplantation. Transplantation 105(1): 231-239.
-
Demer LL, Tintut Y (2008) Vascular Calcification**:** Pathobiology of a Multifaceted Disease. Circulation 117(22): 2938-2948.
-
Bostrom K, Watson KK, Horn S, Wortham C, Herman JM, et al. (1993) Bone Morphogenetic Protein Expression in Human Atherosclerotic Lesions. J Clin Investig 91(4): 1800-1809.
-
Kidney Disease Improving Global Outcomes (KDIGO) CKD-MBD Work Group (2009) KDIGO Clinical Practice Guide lines for the Diagnosis, Evaluation, Prevention and Treatment of Chronic Kidney Disease- Mineral and Bone Disorders (CKD-MBD). Kidney Int Suppl 113: S1-S130.
-
Cozzolino M, Dusso AS, Slatopolski E (2001) Role of Calcium-Phosphate Product and Bone Associated Proteins on Vascular Calcification in Renal Failure. J Am Soc Nephrol 12(11): 2511-2516.
-
Martola L, Barany P, Stenvinkel P (2005) Why Do Dialysis Patients Development a Heart of Stone and Bone of China? Blood Purif 23(3): 203-210.
-
Hejao Agudelo J, Baia L, Orimanji M, Santos ARP, Machado JR, et al. (2018) Fish Oil Supplementation Reduces Inflammation But Does Not Restore Renal Function and Klotho Expression in an Adenine Induced CKD Model. Nutrients 10(9): 1283.
-
Rysz J, Franczyk B, Lawinski J, Olszewski R, Calkowska- Rysz A, et al. (2021) The Impact of CKD on Uremic Toxins and Gut Microbiota. Toxins(Basel) 13(4): 252.
-
Viegas C, Araujo N, Marreiros C, Simon D (2019) The Interplay between Mineral Metabolism, Vascular Calcification and Inflammation in Chronic Kidney disease(CKD): Challenging Old Concepts with New Facts. Aging (Albany NY) 11(12): 4274-4299.
-
Gupta J, Mitra N, Kanetsky PA (2012) Association between Albuminuria, Kidney Function and Inflammatory Biomarker Profile in CKD in CRICC. Clin J Am Soc Nephrol 7(12): 1938-1946.
-
Moc SM, Chen NX (2005) Inflammation and Vascular Calcification. Blood Purif 23(1): 64-71.
-
Schett G (2011) Effects of Inflammatory and Anti- Inflammatory Cytokines on the Bone. Eur J Clin Investig 41(12): 1361-1366.
-
Viane L, Behets GJ, Heye S, Claes K, Monbaliu D, et al. (2016) Inflammation and the Bone-Vascular Axis in End Stage Renal Disease. Osteoporosis Int 27(2): 489-497.
-
Lau WL, Kalantar Zadeh K, Vaziri ND (2015) The Gut as a Source for Inflammation in Chronic Kidney Disease. Nephron 30(2): 92-98.
-
Wong J, Piceno YM, DeSantis TZ, Pahl M, Andersen GL, et al. (2014) Expansion of Urease and Uricase Containing Indole- and P-Cresol Forming and Contraction of Short Chain Fatty Acids Producing Intestinal Microbiota in ESRD. Am J Nephrol 39(3): 230-237.
-
Chung SY, Barnes JL, Astroth KS (2019) Gastrointestinal Microbiota in Patients with Chronic Kidney Disease: A Systematic Review. Adv Nutr 10(5): 888-901.
-
Magnusson M, Magnusson KF, Sundqvist T, Denneberg T (1991) Impaired Intestinal Barrier Function Measured By Differently Sized Polyethylene Glycol in Patients with Chronic Renal Failure. Gut 32(7): 754-759.
-
Onal EM, Afsar B, Covic A, Vaziri ND, Kambay M (2019) Gut Microbiota and Inflammation in Chronic Kidney Disease and their Roles in the Development of Cardiovascular Disease. Hypertens Res 42(2): 123-140.
-
Evenepoel P, Meijers BKI, Bammens BRM, Verbek K (2009) Uremic Toxins Originating from Colonic Microbial Metabolism. Kidney Int Suppl 76: S12-S19.
-
Mafra D, Borges N, Alvarenga L, Esgalhado M, Cardozo L, et al. (2019) Dietary Components That May Influencethe the Disturbed Gut Microbiota in Chronic Kidney Disease. Nutrients 11(3): 1-23.
-
Cupisti A, D’Alessandrio C, Gesualdo L, Cosola C, Gallieni M, et al. (2017) Non-Traditional Aspects of Renal Diets: Focus on Fibers, Alkali and Vitamin K1 Intake. Nutrients 9(5): 444.
-
Kandouz S, Mohamed AS, Zheng Y, Sandeman S, Davenport A (2016) Reduced Protein Bound Uremic Toxins in Vegetarian Kidney Failure Patients Treated by Haemofiltration. Haemodialys Int 20(4): 610-617.
-
Pignanelli M, Just C, Begiasti C, Dinculescu V, Gloor GB, et al. (2018) Mediterranean Diet Score: Associations with Metabolic Products of the Intestinal Microbiome, Plaque Burden and Renal Function. Nutrients 10(6): 779.
-
Sumida K, Yamagata K, Kovesdy CP (2020) Constipation in CKD. Kidney Int Rep 5(2): S121-134.
-
Schmidt JM, Hubner S, Nadal J, Titze S, Schmid M, et al. (2019) Patterns of Medication Use and the Burden of Polypharmacy in Patients with Chronic Kidney Disease: The German Chronic Kidney Disease Study. Clin Kidney J 12(5): 663-672.
-
Rabbar Saadat Y, Niknals B, Hosseniyan Khatebi SM, Ardalan M, Majdi H, et al. (2020) Gut Microbiota: An Overlooked Effect of Phosphate Binders. Eur J Pharmacol 868: 172892.
-
Jernberg C, Lofmark S, Edlund C, Jansson JK (2010) Long Term Impact of Antibiotic Exposure on the Human Intestinal Microbiota. Microbiology 156(11): 3216- 3223.
-
Kortman GAM, Reijnder D, Swinkels DW (2017) Oral Iron Supplementation: Potential Implications for the Gut Microbiome and Metabolism in Patients with CKD. Haemodial Int 21: S28-S36.
-
Swarte JC, Douwes RW, Hu S, Vich Vila A, Eisenga MF, et al. (2020) Characteristics and Dysbiosis in the Gut Microbiome in Renal Transplant Recipients. J Clin Med 9(2): 386.
-
Lee JR, Muthukumar T, Dadhania D, Taur Y, Jenq RR, et al. (2015) Gut Microbiota and Tacrolimus Dosing in Kidney Transplantation. PLoS ONE 10(3): e0122399.
-
Evenepoel P, Dejongh S, Verbek K, Meijers B (2020) The Role of Gut Dysbiosis in the Bone-Vascular Axis in Chronic Kidney Disease. Toxins (Basel) 12(5): 285.
-
Meijers BKI, Deloor H, Bammens BRM, Verbek K, Vanrenterghem Y, et al. (2009) p-Cresyl Sulfate and Indoxyl Sulfate in Haemodialysis Patients. Clin J Am Soc Nephrol 4(12): 1932-1938.
-
Liabeuf S, Baretto DV, Baretto FC, Meert N, Glorieux G, et al. (2010) Free p-Cresyl Sulfate is a Predictor of Mortality in Patients at Different Stages of Chronic Kidney Disease. Nephrol Dial Transplant 25(4): 1183-1191.
-
Baretto FC, Baretto DV, Liabeuf S, Meert N, Glorieux G, et al. (2009) Serum Indoxyl Sulfate is Associated with Vascular Disease and Mortality in Chronic Kidney Disease Patients. Clin J Am Soc Nephrol 4(10): 1551-1558.
-
Lano G, Burtey S, Sallee M (2020) Indoxyl Sulfate: A Uremic Endotheliotoxin. Toxins (Basel) 12(4): 229.
-
Adijiang A, Goto S, Uramoto S, Nishijima J, Niwa T (2008) Indoxyl sulfate promotes aortic calcification with expression of Osteoblast specific proteins inhypertensive rats. Nephrol Dial Transplant 23(6): 1892-1901.
-
Mutellielu G, Enomoto A, Jiang A, Takahashi M, Niwa T (2009) Indoxyl sulfate induces Oxidative stress expression of Osteoblast specific proteins in vascular smooth muscle cells. Nephrol Dial Transplant 24(7): 2051-2058.
-
Yamamoto H, Tsuruoka S, Ioka T, Ando H, Ito C, et al. (2006) Indoxyl sulfate stimulates proliferation of rat vascular smooth muscle cells. Kidney Int 69(10): 1780- 1785.
-
Chang JF, Hsuieh CY, Liou JC, Liu SH, Hung CF, et al. (2020) Scavenging intracellular ROS attenuates p-cresyl sulfate triggered osteogenesis through MAPK signaling pathway and NF-κB activation. Toxins (Basel) 12(8): 472.
-
Opdebeek B, Maudsley S, Azmi A, Maré AD, Leger WD, et al. (2019) Indoxyl sulfate and p-cresyl sulfate promote vascular calcification and associate with glucose intolerance. J Am Soc Nephrol 30(5): 751-766.
-
Jing YJ, Ni JW, Ding FH, Fang YH, Wang XQ, et al. (2016) P-cresyl sulfate is associated withcarotid arteriosclerosis in haemodialysis patients inhibits and promotes atherogenesis in apoE-/- mice. Kidney Int 89(2): 439- 449.
-
Rossi M, Campbell K, Johnson D, Stanton T, Pascoe E, et al. (2014) Uremic toxins and cardiovascular disease across the Chronic Kidney Disease spectrum: an observational study. Nutr Metab Cardiovasc Dis 24(9): 1035-1042.
-
Lai YH, Wang CH, Kuo CH, Lin YL, Tsai JP, et al. (2020) Serum p-cresyl sulfate is a predictor of central arterial stiffness in patients on haemodialysis. Toxins (Basel) 12(1): 10.
-
Holle J, Querfeld U, Kirchner M, Anninos A, Okun J, et al. (2019) Indoxyl sulfate associates with cardiovascular phenotype in children with Chronic Kidney Disease. Paediatr Nephrol 34(12): 2571-2582.
-
Yamamoto S, Fukagawa M (2017) Uremic toxins and bone in CKD. J Nephrol 30(5): 623-627.
-
Watanabe K, Tominari T, Hirata M, Matsumoto C, Hirata J, et al. (2017) Indoxyl sulfate, a Uremic toxinin Chronic Kidney Disease suppresses both bone formation and bone resorption. FEBS Open Bio 7(8): 1178-1185.
-
Hirata J, Hirai K, Asai H, Matsumoto C, Inada M, et al. (2015) Indoxyl sulfate exacerbates low bone turnover in parathyroidectomy in young adult rats. Bone 79: 252- 258.
-
Kamprom W, Tawanswatruk T, Mas Oodi SM, Anansilp K, Rattanasompattikul M, et al. (2021) P-cresyl and Indoxyl sulfate impair Osteogenic differentiation by triggering mesenchymal stem cells Senescence. Int J Mol Sci 18(3): 744-755.
-
Nii Kono T, Iwasaki Y, Uchida M, Fujieda A, Hosokawa A, et al. (2007) Indoxyl sulfate induces skeletal resistance to parathyroid hormone in cultured Osteoblastic cells. Kidney Int 71(8): 738-743.
-
Iwasaki Y, Kazama JJ, Yamato H, Shimoda H, Fukagawa M (2013) Accumulated uremic toxins attenuates bone mechanical properties in rats with Chronic Kidney Diseases. Bone 57(2): 477-481.
-
Goto S, Fujii H, Hamada Y, Yoshiya K, Fukagawa M (2010) Association between Indoxyl sulfate and skeletal resistance in haemodialysis patients. Ther Apher Dial 14(4): 417-423.
-
Liu WC, Wu CC, Hung YM, Liao MT, Shyu JF, et al. (2016) Pleiotropic effects of VitaminD in Chronic Kidney Disease. Clin Chim Acta 453: 1-12.
-
Moraes C, Fouque D, Amarai ACF, Mafra D (2015) Trimethylamine-N-oxide from gut microbiota in Chronic Kidney Disease patients: focus on diet. JRen Nutr 25(6): 459-465.
-
Strubbs JR, House JA, Ocque AJ, Zhang S, Johnson C, et al. (2016) Serum Trimethylamine-N-oxide is elevated in CKD and correlate with coronary atherosclerosis burden. J Am Soc Nephrol 27(1): 305-313.
-
Keith RA, Wang Z, Levison BS, Buffa JA, Org E, et al. (2013) Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat promotes atherosclerosis. NatMed 19(5): 576-85.
-
Pelletier CC, Croyle M, Ene L, Aguesse A, Billon Crossouard S, et al. (2019) Elevation of Trimethylamine-N-oxide in Chronic Kidney Disease: contribution of decreased glomerular filtration rate. Toxins (Basel) 11(11): 635.
-
Zhang X, Li Y, Yang P, Liu X, Lu L, et al. (2020) Trimethylamine-N-oxide promotes vascular calcification through Zhang activation ofNLRP3(nucleotide-binding domain, leucine-rich-repeat containing family, pyrin domain-containing 3inflammasome and NF-κB (nuclear factor-kappaB). Arterioscler Thromb Vasc Biol 40(3): 751-765.
-
Li L, Chen B, Zhu R, Li R, Tian Y, et al. (2019) FructusLigustri Lucidi promotes vascular calcification through the regulation of gut microbiota diversity, Oxidative stress, TMAO and Sirt6 levels in aging mice. Aging (Albany NY) 11(21): 9348-9368.
-
Zhou T, Heianza Y, Chen Y, Li X, Sun D, et al. (2019) Circulating gut microbiota metabolite role of Trimethylamine-N-oxide (TMAO) and changes in bone density in response to weight loss diets: The pounds lost trial. Diabetes Care 42(8): 1365-1371.
-
Lin H, Liu T, Li X, Gao X, Wu T, et al. (2020) The role of gut microbiota metabolite Trimethylamine-N-oxide in functional impairment of bone marrow mesenchymal stem cells in osteoporosis disease. Ann Transl Med 8(16): 1009.
-
Cozzolino M, Fusaro M, Ciceri P, Gasperoni L, Cianciolo G (2019) The role of Vitamin K in vascular calcification. Adv Chronic Kidney Dis 26(6): 437-444.
-
Mansour AG, Hariri E, Daaboui Y, Korjian S, El Alam A, et al. (2017) Vitamin K2 supplementation and arterial stiffness among renal transplant recipients a Single-arm, Single-center Clinical trial. J Am Soc Hypertens 11(9): 589-589.
-
Schurgers LJ, Baretto DV, Baretto FC, Liabeuf S, Renard C, et al. (2010) The Circulating inactive form of matrix Gla protein is a surrogate marker for vascular calcification in Chronic Kidney Disease: a preliminary report. Clin J Am Soc Nephrol 5(4): 568-575.
-
Walther B, Philip Kurt J, Booth SL, Bovaval P (2013) Menaquinones, bacteria and the food supply: the relevance of dairy and s fermented food products to Vitamin K requirements. Adv Nutr 4(4): 463-473.
-
Booth SL, Dallal G, Shea MK, Gundberg C, Peterson JW, et al. (2008) Effects of Vitamin K supplementation on bone loss in elderly men and women. J Clin Endocrinol Metab 93(4): 1217-1223.
-
Shearer M, Newman P (2008) Metabolism and cell biology of Vitamin K. Thromb Haemostat 100(4): 530- 547.
-
Walther B, Philip KJ, Booth SL, Bovaval P (2013) Menaquinones, bacteria and the food supply: the relevance of dairy and s fermented food products to Vitamin K requirements. Adv Nutr 4(4): 463-473.
-
Booth SL, Dallal G, Shea MK, Gundberg C, Peterson JW, et al. (2008) Effects of Vitamin K supplementation on bone loss in elderly men and women. J Clin Endocrinol Metab 93(4): 1217-1223.
-
Shearer M, Newman P (2008) Metabolism and cell biology of Vitamin K. Thromb Haemostat 100(4): 530- 547.
-
Wagatsuma K, Yamada S, Ao M, Matsuura M, Tsuji H, et al. (2019) Diversity of gut microbiotaaffecting serum level of undercarboxylated osteocalcin in patients with crohn’s disease. Nutrients 11(7): 1541.
-
Jansz TT, Neradova A, van Ballegooijen AJ, Verhaar MC, Vervloet MG, et al. (2018) The role of Kidney transplantation and phosphate binder state in Vitamin K status. PLoS One 13(8): e0203157.
-
Guss JD, Taylor E, Rouse Z, Roubert S, Higgins CH, et al. (2019) The microbial metagenome and bone tissue composition in mice with reduction in bone strength. Bone 127: 146-154.
-
Akbari S, Rasouri GAA (2018) Vitamin K and bone metabolism:a review of the latest preclinical studies. Biomed Res Int 2018: 4629383.
-
Kurnatowska I, Grzelak P, Masajtis ZA, Kaczmarska M, Stefanczyk L, et al. (2015) Effect of Vitamin K2 on progression of atherosclerosis and vascular calcification in nondialyzed patients with Chronic Kidney Disease stages3-5. Pol Arch Med Wewn 125(9): 631-640.
-
Atkins GJ, Welldon KJ, Wijenayaka AR, Bonewald LF, Findlay DM (2009) Vitamin K promotes mineralization, osteoblasts to osteoclasts transition, and an anti- catabolic phenotype by Carboxylation dependent and independent mechanisms. Am J Physiol Cell Physiol 25: 1358-1367.
-
Cockayne S, Adamson J, Lanham NS, Shearer MJ, Gilbody S, et al. (2006) Vitamin K and the prevention of fractures. Arch Intern Med 155(12): 1256-1261.
-
Fusaro M, Noale M, Viola V, Galli F, Tripepi G, et al. (2012) Vitamin K, vertebral fractures, vascular calcification and mortality: Vitamin K Italian (VIKI) dialysis study. J Bone Miner Res 27(11): 2271-2278.
-
Thamratnopkoon S, Susantitaphong P, Tumkosit M, Katavetin P, Tiranathanagul K, et al. (2017) Correlation of plasma dephosphorylated uncarboxylated matrix Gla protein with vascular calcification and vascular stiffness in Chronic Kidney Disease. Nephron 135(3): 167-172.
-
Witham MD, Lees JS, White M, Band M, Bell S, et al. (2020) Vitamin K supplementation to improve vascular stiffness in CKD: the K4 Kidney randomized controlled trial. J Am Soc Nephrol 31(10): 2434-2445.
-
Lees JS, Mark PB, Witham MD (2021) Vitamin K and vascular stiffness. Clin J Am Soc Nephrol 30(4): 430-436.
-
Lucas S, Omata Y, Hofmann J, Bottcher M, Iljazovic A, et al. (2018) Short chain fatty acids regulate systemic bone mass and protect from pathological bone loss. Nat Commun 9(1): 1-10.
-
Caluwe R, Verbek F, De Vries AS (2020) Evaluation of Vitamin K status and rationale for Vitamin K supplementation in dialysis patients. Nephrol Dial Transplant 35: 25-33.
-
Den Besten G, Van Eunen K, Groen AK, Venena K, Reijngoud DJ, et al. (2013) The role of short chain fatty acids in the interplay between diet, gut microbiota and host energy metabolism. J Lipid Res 54(9): 2325-4230.
-
Felizardo R, Watanabe IK, Dardi P, Rossoni LV, Camana N (2019) The interplay among gut microbiota, hypertension and Kidney disease : The role of short chain fatty acids. Pharmacol Res 141: 366-377.
-
Vinolo MA, Rodriques HG, Nachbar RT, Curi R (2018) Regulation of inflammation by short chain fatty acids. Nutrients 3(10): 858-876.
-
Caluwe R, Verbek F, De Vries AS (2020) Evaluation of Vitamin K status and rationale for Vitamin K supplementation in dialysis patients. Nephrol Dial Transplant 35: 25-33.
-
Zhou T, Wang M, Ma H, Li X, Heianza Y, et al. (2021) Dietary fiber, genetic variations of gut microbiota derived short chain fatty acids. J Clin Endocrinol Metab 106(1): 201-210.
-
Borges NA, Carmo FL, Pinto MBS, de Brito JS, Dolenga CJ et al. (2018) Probiotic supplementation in Chronic Kidney Disease: a double blind, randomized placebo controlled trial. J Ren Nutr 28(1): 28-36.
-
Binda S, Hill C, Johansen E, Obis D, Pot B, et al. (2020) Criteria to qualify microorganisms as Probiotic’’ in food and Diet supplement. Front Microbial 11: 1662.
-
Armani RG, Carvalho AB, Ramos CI, Hong V, Bortolotto LA, et al. (2021) Effects of fructoligosacchharides on endothelial function in CKD patients: a randomized controlled trial. Nephrol Dial Transplant 37(1): 85-91.
-
Armani RG, Ramezzani A, Yasir A, Sharama S, Canziani MEF, et al. (2017) Gut microbiome in Chronic Kidney Disease. Curr Hypertens Rep 19(4): 29.
-
Hill E, Sapa H, Negrea L, Bame K, Hostetter T, et al. (2020) Effect of oat b-glucan supplementation in Chronic Kidney Disease:a feasibility study. J Ren Nutr 30(3): 208- 215.
-
Ramos CI, Armani RG, Canziani MEF, Dalboni MA, Dolenga CJR, et al. (2019) Effects of Prebiotic(fructoligos acchharides) on uremic toxins of Chronic Kidney Disease patients: A randomized controlled trial. Nephrol Dial Transplant 34(11): 1876-1884.
-
Niwa T, Yazawa T, Ise M, Sugano M, Kodama T, et al. (1991) Inhibitory effect of oral sorbent on accumulation of albumin bound indoxyl sulfate in serum of experimental uremic rats. Nephron 57(1): 84-88.
-
Sato E, Saigusa D, Mishima E, Uchida T, Miura D, et al. (2018) Impact of the oral adsorbent AST 120 on organ specific accumulation of uremic toxins: LC-MS/MS and MS imaging techniques. Toxins(Basel) 10(1): 19.
-
Sato E, Hosomi K, Sekimoto A, Mishima E, Oe Y, et al. (2020) Effects of oral adsorbent Kidney damage AST 120 on fecal p-cresol and indol levels and on the gut microbiota composition. Biochim Biophys Res Commun 525(3): 773-779.
-
National Library of Medicine U (2021). Oral absorbent and Probiotics in CKD patients with PAD on gut microbiota, lncRNA, Metabolome and vascular function. Clinical trials Gov Identifier.
-
Rodriques FG, Ormanji MS, Heilberg JP, Bakker SJL, De Borst MH (2021) Interplay between gut microbiota, bone health and vascular calcification in Chronic Kidney Disease.Eur J Clin Investig. 51(9): 13588.
-
Marques SS, Barreiros L, Sampaio Maio B, Segundo MA, Fernandes SR (2022) Rapid and sustainable HPLCmethod for the determinationof uremic toxins in human plasma samples .Anal Bioanal Chem ahead of print dec 5.
-
Ebrahim Z, Proost S, Tito RY, Raes J, Glorieux G, et al. (2022) The effect of β-Glucan Prebiotic on Kidney function, uremic toxins and gut microbiome in stage 3 to 5 Chronic Kidney Disease(CKD) in pre dialysis participants: a randomized controlled trial. Nutrients 14(4): 805.
-
Shamloo M, Mollard R, Wang H, Kingra K, Tangri N, et al. (2022) A randomized double blind cross over trial to study the effects of resistant starch prebiotic in Chronic Kidney Disease(ReSPECKD). Trials 23(1): 72.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty