A Case of Multinodular Goiter Treated with Iodum 200 C
Hyperthyroidism is a pathological disorder in which excess thyroid hormones are secreted by the thyroid gland. Hyperthyroidism increases with age and is more frequent in women. Hyperthyroidism develops in most of the cases of Multinodular Goiter after frequent intake of iodine. Multinodular Goiter (MNG) is the most common disorder of the thyroid gland result of the genetic heterogeneity of follicular cells and apparent acquisition of new inheritable cellular qualities. It is most often detected as a simple mass in the neck but sometimes an enlarging gland produces pressure symptoms. This article describes a case of a 39-year-old female patient who presented with swelling in neck associated with pain in left eye and blurred vision since 2 years. The case was diagnosed as Multinodular Goiter and treated in the OPD of our hospital. Thorough case taking was done and the totality of symptoms was constructed. Based on the totality, Iodum 200 C / 5 doses once in 3 days were prescribed for 2 weeks. The case got remarkably improved within a period of 4 months with the thyroid hormones ranging within normal limits. Thus it is evident that Multinodular Goiter with hyperthyroidism can be treated efficiently with well selected specific homoeopathic medicines.
Introduction
Hyperthyroidism is a common thyroid disorder associated with excess thyroid hormone production. Hyperthyroidism can be overt or subclinical. Overt hyperthyroidism is characterized by low serum thyroid- stimulating hormone (TSH) level and raised serum levels of Thyroxine (T4), Triiodothyronine (T3) or both [1]. Subclinical hyperthyroidism is characterized by low serum TSH but normal serum T4 and T3 concentrations [2]. The prevalence of hyperthyroidism varies based on dietary iodine content. The risk factors associated with the hyperthyroidism include smoking, iodine deficiency, iodine excess, selenium deficiency, genetic factors and the use of certain drugs [3]. Hyperthyroidism is most commonly seen in women compared to men [4].
Multinodular goiter (MNG) is the most common disorder of the thyroid gland. It is the result of the genetic heterogeneity of follicular cells and apparent acquisition of new inheritable cellular qualities. It is most often detected as a simple mass in the neck but sometimes an enlarging gland produces pressure symptoms. The risk factors associated with the hyperthyroidism include smoking, iodine deficiency, iodine excess, selenium deficiency, genetic factors and the use of certain drugs. The nodules of MNG may present as growths and fusion of localized colloid-filled follicles or discrete adenomas or cysts. Nodules larger than 1 cm may be detected clinically by palpation. Nodules less than 1 cm in diameter are not clinically detectable unless located on the surface of the gland and are much more frequent. Hyperthyroidism develops in most of the cases of MNG after frequent intake of iodine. Majority of the lesions are not lethal whereas 4 to 17% of MNG cases fulfill the criteria of malignant change. The incidence of goiter depends upon the status of iodine intake of the population. In areas of iodine deficiency, prevalence of goiter is very high and longstanding goiters may develop multinodularity frequently. The etiological factors of MNG include functional heterogeneity of normal follicular cells due to genetic, acquisition of new inheritable qualities by replicating epithelial cells, subsequent functional and structural abnormalities in growing goiters, elevated TSH (induced by iodine deficiency, excessive intake of natural goitrogens, congenital abnormalities of thyroid hormone synthesis), smoking, stress and certain drugs [5].
Materials and Methods
This case was taken using standardized case record format from Unit VII of Sarada Krishna Homoeopathic Medical Collegiate Hospital. Wayne’s index [6] showing the scoring of signs and symptoms for the diagnosis of hyperthyroidism is used. Overall improvement of the case was analyzed by repeated investigations and follow up.
Case Presentation
A 39 years old female patient presented with complains of swelling around the neck since 2 years. The complaint had an insidious onset and gradually progression. She also started experiencing pain over the eyes with blurring of vision. She also suffered from palpitation since 3 months on and off which got aggravated by physical exertion. She had a history of weight loss and hair fall. and weakness of whole body since 1 year. She is taking allopathic medication for these complaints. The complete symptom of the patient is mentioned in Table 1.
| Complaints with Duration | Location & Extension | Sensation / Character &Pathology | Modalities & A/F | Concomitants / Associated Symptoms |
|---|---|---|---|---|
| Swelling in neck since 2 years | Thyroid gland | Swelling | Pain in left eye with blurring of vision since 2 years | |
| Weakness of whole body since 1 year | Whole body | Weakness | < exertion | Hairfall |
| Palpitation since 3 months | Chest | Palpitation | < exertion |
Table 1: Presenting complaints.
Systemic Examination
Examination of Neck (Thyroid Gland):
Inspection: Multiple nodular swellings in the anterior aspect of neck seen, swelling moves on deglutition, swelling does not move on protrusion of tongue, no scars, no dilated veins, no visible pulsation.
Palpation: Multiple nodular swellings of both lobes of thyroid gland, no local warmth, no tenderness, no pulsation felt.
Special tests: Romberton’s test – Negative, Kocher’s test – Negative, Exophthalmos – Present and Other Eye signs – Negative.
WHO Grading of Goiter [6]: According to WHO, goitre is graded into 3 categories. When no goiter presence is found that is, when the thyroid is impalpable and invisible it is included under Grade 0. When neck thickening is present as a result of enlarged thyroid, palpable, however, not visible in normal position of the neck or when the thickened mass moves upwards during swallowing, it is included under Grade 1. Grade 1 includes nodular goiter if thyroid enlargement remains invisible also. When the neck swelling is present and visible when neck is in normal position, corresponding to enlarged thyroid- found in palpation, it is included in Grade 2.
The signs and symptoms of the patient indicate that this patient has Grade 2 Goiter, as per WHO Grading of Goiter.
| Score | Signs | Present | Absent | |
|---|---|---|---|---|
| Dyspnea on effect | - | Palpable thyroid | 3 | |
| Palpitations | 2 | Bruit over thyroid | -2 | |
| Fatigue | 2 | Exophthalmoses | 2 | |
| Preference for heat | -5 | Lid Retraction | - | |
| Preference for cold | - | Lid Lag | - | |
| Excessive sweat | 3 | Hyperkinesia | -2 | |
| Nervousness | - | Hands hot | -2 | |
| Appetite: Increased | - | Hands moist | -1 | |
| Appetite: Decreased | - | Casual pulse rate: | ||
| 80 – 90 beats per minute> 90 beats per minute | < 80 beats per minute | - | ||
| 80 – 90 beats per minute> 90 beats per minute | 3 | |||
| 80 – 90 beats per minute> 90 beats per minute | - | |||
| Weight: Increased | - | Atrial Fibrillation | - | |
| Weight: Decreased | 3 | Atrial Fibrillation | - |
Table 2: Wayne’s index showing the scoring of signs and symptoms for the diagnosis of hyperthyroidism.
Homoeopathic Analysis
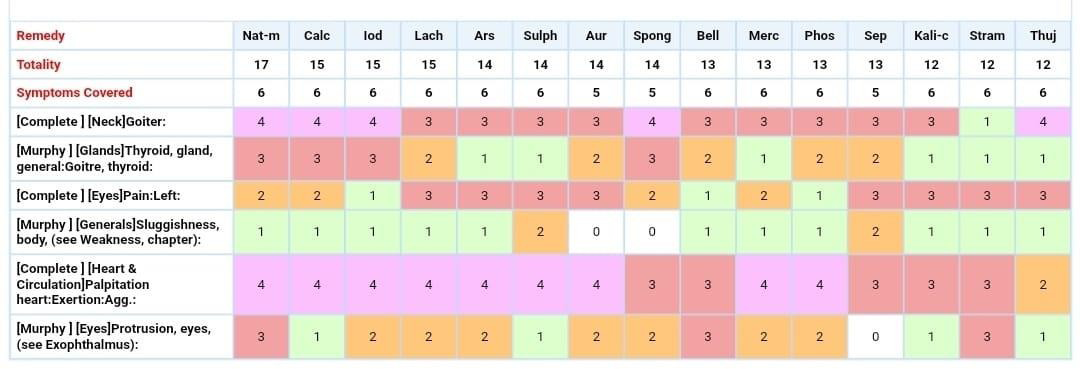
The patient was treated as a whole with the similimum obtained on constructing the totality of symptoms inclusive of mental, physical and particular symptoms as shown in Table 3. The rubrics for the totality of symptoms were selected and repertorization was done as shown in Figure 1 Homoeopathic Intervention:
The patient was treated with similimum and the symptomatic changes in the subsequent follows up were recorded as shown in Table 4. The patient was advised to take Thyroid Function Test (TFT) periodically and the reports were preserved.
| Mental generals | Physical generals | Particular symptoms |
|---|---|---|
| Fear of disease =++ | Appetite: Good (3 times/ day) Thirst: Good (liters/ day) Stool: Regular | Swelling in the neck (Enlarged thyroid gland) |
| Memory loss | Urine: Regular Sleep: Good | Pain in left eye with blurring of vision |
| Weeps easily | Sweat: Increased in axillae Craving: Non vegetarian food Aversion: Milk | Weakness of whole body |
| Thought crowded | Desire: Covering Aversion: Fanning | < exertion |
| Desire: Music | Thermal: Chilly | Weakness of whole body with hairfall Palpitation < exertion |
Table 3: Evaluation and Totality of symptoms.
Result
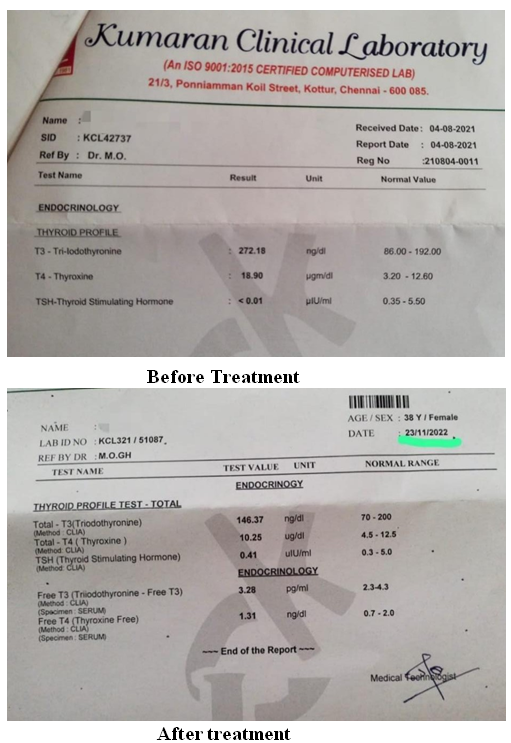
A 39 years old female patient presented with complains of swelling around the neck since 2 years. The complaint had an insidious onset and gradually progression. She also started experiencing pain over the eyes with blurring of vision. She also suffered from palpitation since 3 months on and off which got aggravated by physical exertion. She had a history of weight loss and hair fall. and weakness of whole body since 1 year. She was diagnosed with Multinodular goiter with hyperthyroidism. Based on the Repertorial result and totality of symptoms, Iodum 200 C/ 5 Doses once in 3 days for 2 weeks was prescribed in the first sitting. The same medicine was repeated in regular intervals based the symptomatic changes in the subsequent sittings. The Goiter was graded using the WHO Grading of Goiter and symptoms of hyperthyroidism were evaluated using Wayne’s Index as shown in Table 2. The changes in the levels of thyroid hormones before, during and after treatment were preserved as photographs as shown in Figure 2.
| Date | Follow up | Prescription |
|---|---|---|
| 10/8/2022(First Sitting) | Swelling in neck more on right side (Enlarged thyroid gland)Pain in left eye with blurring of vision Weakness of whole body < exertion Weakness of whole body with hair fall Palpitation < exertion | Rx 1. IODUM 200 C /5 Doses (once in 3 days) 2. B. PILLS 3 × TDS 3. B. DISK 1 × BD |
| × 2 weeks | ||
| 24/08/2022 | Swelling in the neck (Enlarged thyroid gland) [persists]. Weakness of whole body < exertion [persists] Weakness of whole body with hair fall [persists] Palpitation < exertion [persists] Generals: All good and regular | Rx 1. IODUM 200 C /5 Doses (once in 3 days) 2. B. PILLS 3 × TDS 3. B. DISK 1 × BD |
| × 4 weeks | ||
| 1/10/2022 | Swelling in the neck (Enlarged thyroid gland) [persists]. Weakness of whole body < exertion [persists] Weakness of whole body with hair fall [persists] Palpitation < exertion [persists] Generals: All good and regular | Rx 1. IODUM 200 C /5 Doses (once in 3 days) 2. B. PILLS 3 × TDS 3. B. DISK 1 × BD |
| × 4 weeks | ||
| 15/11/2022 | Swelling in the neck (Enlarged thyroid gland) [persists]. Weakness of whole body < exertion [Better] Weakness of whole body [Better] Palpitation < exertion [Better] Generals: All good and regular | Rx 1. IODUM 200 C /5 Doses (once in 3 days) 2. B. PILLS 3 × TDS 3. B. DISK 1 × BD |
| × 4 weeks | ||
| 22/12/2022 | Swelling in the neck (Enlarged thyroid gland) [Better]. Weakness of whole body < exertion [Better] Weakness of whole body with hair fall [Better] Palpitation < exertion [Better] Generals: All good and regular | Rx 1. IODUM 200 C /5 Doses (once in 3 days) 2. B. PILLS 3 × TDS 3. B. DISK 1 × BD |
| × 2 weeks |
Table 4: Symptomatic changes in the follows - up and corresponding prescription.
Discussion
Nodular goiters are experienced in patients commonly seen during clinical practice by Physicians. Multinodular goiter may be asymptomatic with normal TSH levels (Non- toxic MNG) or with systemic thyrotoxic symptoms (Toxic MNG) [7]. In iodine deficient areas, the prevalence of nodular goitre is comprised between 0.4 and 7.2% and about 4% in iodine sufficient countries. Nodular goiters are more common in women along with advancing age and mostly after exposure to external irradiation [8].
A case of 39 years old female diagnosed with hard colloid nodular goiter with a size of about 8.2 × 3.6 mm in the right lobe and 30.3 × 24.5 mm in the left lobe for 2 months which came to the OPD of Sri Sai Nath Post Graduate Institute of Homoeopathy, Allahabad, Uttar Pradesh, India was selected for case study. Detailed case taking was done and totality of symptoms was obtained. Based on the repertorisation done with synthesis repertory, the remedy was selected. On the basis of reportorial analysis, Lycopodium got the highest marks covering most of the rubrics. A single dose of Lycopodium 200 was prescribed followed by placebo for 15 days on the first visit. After 15 days, the second dose of Lycopodium 200 was given on the second visit. Within 4 months, the patient improved and the size of the goiter got significantly reduced [9].
A patient visited the OPD of Father Muller Homoeopathic Medical College Hospital, Deralakatte, Mangalore, Karnataka, India mainly for complaints of pain in the right side of neck which got aggravated while swallowing and moving her neck to sides for the past 4-5 months. After dissatisfying outcome with modern medicine, patient resorted to homoeopathic treatment. A detailed case-taking and repertorisation was done. Phosphorous was given in moderate potency and repetition was based on the response of the medicine upon patient. Within 1 year 4 months of homoeopathic treatment, the patient became free from her complains [10].
In this study, a 39 years old female patient presented with complains of swelling around the neck since 2 years was taken. She also had pain over the eyes with blurring of vision and palpitation since 3 months a history of weight loss, hair fall and weakness of whole body since 1 year. She was diagnosed with Multinodular goiter with hyperthyroidism. Based on the Repertorial result and totality of symptoms, Iodum 200 C/ 5 Doses once in 3 days for 2 weeks was prescribed in the first sitting. The same medicine was repeated in regular intervals based the symptomatic changes in the subsequent sittings.
Conclusion
This case of Multinodular Goiter with Hyperthyroidism was prescribed with IODUM 200 C in regular intervals and the gradual improvement in the symptoms of the patient was witnessed. In addition to this, the levels of thyroid hormones came to normal. In allopathic system of medicine, thyroid supplements are given in case of hyperthyroidism and surgery is insisted in cases of MNG. Long term Hormone therapy gas significant side effects in the humans. On the other hand, the individualistic approach of homoeopathic system of medicine improves the vital force the patient thereby facilitating the normal secretion of hormones. From this study, we could infer that the well selected homoeopathic medicines are efficacious in the treatment of endocrine disorders both in the symptom and hormone levels.
References
-
Ross DS, Burch HB, Cooper DS, Greenlee MC, Laurberg P, et al. (2016) 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid 26(10): 1343-1421.
-
Biondi B, Cooper DS (2018) Subclinical Hyperthyroidism. N Engl J Med 378(25): 2411-2419.
-
Taylor PN, Albrecht D, Scholz A, Gutierrez-Buey G, Lazarus JH, et al. (2018) Global epidemiology of hyperthyroidism and hypothyroidism. Nat Rev Endocrinol 14(5): 301- 316.
-
Madariaga GA, Palacios S, Guillén-Grima F, Galofre JC (2014) The incidence and prevalence of thyroid dysfunction in Europe: a meta-analysis. J Clin Endocrinol Metab 99(3): 923-931.
-
Medeiros Neto G (2016) Multinodular Goiter. In: Feingold KR, Anawalt B, et al., editors. South Dartmouth (MA): MDText.com, Inc 2000.
-
Kalra S, Khandelwal SK, Goyal A (2011) Clinical scoring scales in thyroidology: A compendium. Indian J Endocrinol Metab 15(Suppl 2): S89-94.
-
Hurley DL, Gharib H (1996) Evaluation and management of multinodula goiter. Otolaryngologic Clinics of North America 29(4): 527- 540.
-
Pinchera A, Aghini-Lombardi F, Antonangeli L, Vitti P (1996) Multinodular goiter. Epidemiology and prevention. Annali Italiani di Chirurgia 67(3): 317-325.
-
Shukla V (2021) Homoeopathic treatment of nodular goitre: A Case report. Int J Homoeopath Sci 5(3): 67-70.
-
Britto RC, George F (2022) Homoeopathic management of multinodular goitre: A case report 6(2): 133-136.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty