Assessment of Serum Calcium, Magnesium and Cholecalciferol Status in the Patients of Migraine: A Cross Sectional Analytical Study
Background: Migraine which is a common intense headache occurs usually on one side of head accompained by the symptoms of nausea, vomiting and increased sensitivity to light and sound, photophobia and phonophobia. As the exact mechanisum in the pathogenesis of migraine is not clearly documented but it is thought that the deficiency of some important elements may have role to alleviate headache and migraine. Therefore we have evaluated the role of serum cholecalciferol, magnesium and calcium in the patients with migraine to confirm our results. Objective: The aim of this study is to evaluate the serum cholecalciferol, calcium and magnesium levels in the chronic migrainuers in comparison to normal healthy individuals. Methodology: A cross-sectional analytical study that was conducted at Isra University hospital and Liaquat University of health and medical sciences hospital, Hyderabad. Total sixty subjects were selected and divided into two groups as group-A comprising of 30 normal subjects and group-B consisting of 30 chronic migrainuers cases. The selection of case subjects were carried out through non-probability purposive sampling based on inclusion and exclusion criteria. Whole blood 5cc was taken from each subject and was immediately centrifuged at 3000 rpm for 10-15 minutes to separate out serum which is used for the quantification of cholecalciferol, calcium and magnesium levels in the serum. The data was analyzed on SPSS version 22.0. The continuous and categorical variables were analyzed using Student t-test and Chi square test. Results were described as statistically significant at p-values ≤ 0.05. Results: The data obtained by the present study showed that the mean±SD of age in group A and group B was 38.8±9.64 and 40.2±10.7 years respectively with p-value 0.49 in the normal and migraine patients. However, mean±SD of serum cholecalciferol was found to be 23.94±7.04 and 19.08±6.33ng/dl respectively with p-value 0.007. It has also been noticed that about 90% of the chronic migrainuers showed deficiency or insufficiency of serum cholecalciferol as compared to 73% in the control subjects. The mean±SD of serum calcium in both groups A and was noted as 9.28±0.67 and 8.89±0.83 ng/dl respectively with p-value 0.047. In addition mean±SD of serum magnesium was found to be 1.88±0.24 and 1.75±0.20 ng/dl in both A and B groups respectively with p-value 0.022. Conclusion: It is concluded that serum cholecalciferol, calcium and magnesium was found to be in lower levels in the patients during migraine attack as compared to normal subjects having no complain of headache by the subjects.
Introduction
A migraine is usually called as episodic vascular disorder which is a clinical condition that greatly disturbs the quality of life of the persons, their families and friends. The prevalence of this disease in both men and women is between 25 to 39 years of life period [1, 2]. It has been reported in a study that migraine a primary headache disorder usually called as tension-type of headache continues to be under diagnosed and under-treated. It is characterized by the recurrent attacks lasting to 4-72 hours and this may be accompained by the symptoms of neausea, vomiting, increased sensitivity to light and sound, photophobia or phonophobia [3, 4, 5, 6].
Migraine which is a chronic headache disorder has been classified into two main sub-types migraine with aura and migraine without aura as recognized by the criteria of international Classification of Headache Disorder. Migraine with aura is characterized primarily by the transient neurological symptoms such as depression, repetitive yawning, fatigue and neck stiffness and pain where as migraine without aura is a clinical syndrome characterized by headache along with photophobia or photophonia [7]. It is reported that migraine which is caused either by cortical spreading depression theory is basically a disease related to the brain characterized by the disturbances in the normal functioning of brain or vascular theory which suggests that it is related by the widening of blood vessels that cause migraine pain and aura. It is further reported that serotonin a chemical neurotransmitter play an important role in the development of migraine [8, 9].
Few studies reported that the basic mechanism of migraine pain in the brain is due to the release of some pain-producing inflammatory substances around the nerves and blood vessels in the head. The main characteristic of migraine attack is headache that may take several hours to 2-3 days. This neurological characteristic is often severe pulsating and one-sided [10, 11].
Several studies in the scientific literature in this respect have reported the association of migraine with the serum level vitamin D, calcium and magnesium. In relation to the chemical nature, vitamin D is a fat soluble secosteroid synthesized in the skin from 7-dehydro cholesterol as hormone or ingested with food as vitamin [12]. Deficiency of vitamin D is associated with chronic pain disorder, depression and other neurological disorders [13, 14].
It has been reported in another study that the brain has numerous receptors and vitamin D activating enzyme 1α-hydroxylase found in many cell types and involved in bone and mineral metabolism, inflammation, immune system and in the metabolism of neurotransmitters. In addition vitamin D is also involved in the association of severe headache and thus it is considered as a potential prophylactic agent or adjuvant in the management of migraine [15, 16].
It has been reported in a study that serum cholecalciferol has been associated with migraine by various hypothesis such as decreased synthesis of serotonin, modulation of nitric oxide production, cytokine and calcium channels with in microcirculation [17]. Extensive research has been done on the role of some important minerals. Many studies in this connection have been carried out reported on the role of magnesium and calcium particularly in the pathophysiology of migraine [18]. In addition some mechanisms are concerned to provide the justification of the relationship between calcium level and migraine attacks. In this connection few studies have shown that serum magnesium level in migraine patients compared to healthy control subjects is found slightly lower where as the serum calcium is found in higher level [19]. However, some studies have shown that when calcium is administered along with Vitamin D, it minimizes the frequency of migraine in the considerable number of patients as calcium and magnesium interact with each other [20].
There are no studies conducted so far to measure serum cholecalciferol, serum calcium and serum magnesium together in the patients suffering from chronic migraine. Therefore, the purpose of this study is to determine the level of cholecalciferol, calcium and magnesium in the serum of migraine patients in comparison to the healthy control subjects.
Methodology
Study Design
A cross-sectional analytical study that was carried out to determine the calcium, magnesium and cholecalciferol levels in the serum of chronic migraine patients.
Study Settings
This study was performed at Isra University Hospital Hyderabad and Liaquat University of Medical and Health Sciences Hospital Jamshoro.
Duration of Study
It was a two years study period extending from January 2015 to January 2017.
Study Population, Sample size and Grouping
This cross-sectional analytical study was conducted among migraine patients in comparison to normal healthy individuals. Considering the prevalence of migraine as 2% with 95% confidence interval 0.05 level of significance the sample size was calculated to be 30 [21]. Based on the sample size formula total 60 persons were selected and were divided into Group-A comprising of 30 normal having no complain of regular episodal migraine attacks and Group-B consisting of 30 chronic migraine patients.
Baseline Data and Demographical Assessment
Initially for each subject, baseline data regarding age, sex, bodyweight, height, waist circumference and body mass index were collected. Weight was taken by analogue scale with light clothing and without shoes. Height was taken by measuring without shoes for accuracy. BMI was determined using body weight (in kg) divided by height (in m2). Waist circumference was measured by inelastic tape at narrowest part of body below the ribs.
Biochemical Assessment
For the biochemical assessment, 5.0 ml of whole blood was taken from each patient during the migraine attack and when they were in a normal condition informing no complain of headache at the time of blood sampling. The blood samples were centrifuged at 4000 rpm for the separation of sera from the blood. The sera were then stored at – 20oC till analysis.
The sera obtained from the blood of each individual were used for the determination of serum cholecalciferol [22], serum calcium [23] and serum magnesium [24].
Determination of Serum Cholecalciferol Level (Migraine and Normal Subjects)
The serum 25-hydroxy vitamin D (25-OH-D) concentration is used to assess the vitamin D status. Non- fasting levels of serum 2H (OH) D were measured in human plasma and serum using a chemiluminescent microparticle immunoassay ARCHITECT 1000 reagent kit system for the determination of 25-OH vitamin D. Based on the previous studies and reports of Institute of Medicine (10M) reported the serum levels of 25 (OH) D of < 20, ≥ 20 and <30 and ≥30 ng/ml as deficiency, insufficiency and sufficiency respectively [25]. The normal value is considered as 31-60 ng/ml.
Determination of Serum Calcium (Ca++) Level
The quantitative determination of calcium in human serum was carried out by using Roche 902 automated chemical analyzer.
For the quantitative analysis of calcium level in the serum 6 test tubes were taken and were labeled from A to F. The amount of calcium standard 2ml of 20 mg/dl and diluted assay buffer (5ml diluted with 45ml HPLC graded water) were added into each tube. 10 µl of sample was added in 2 wells of the plate. Working detector reagent was added to all the wells. The plates were then shaken gently for 20-30 sec. The mixture was incubated for 5min at 37oC. The absorbance was read at 570nm and the reading was noted in mol/L.
Normal value of Ca++ in serum: 2.15-2.55mol/L
Determination of Serum Magnesium (Mg++) Level
The quantitative determination of magnesium in human serum was also carried out on Roche automated clinical chemical 902 analyzer.
For the quantitative determination of magnesium level in the serum, 0.5 ml of serum was taken from each person and was then transferred to the konelab 60 chemical analyzer for analysis. 2 µl of serum was taken along with 240 µl of reagent with 2.41 mg/dl of calibrator No.2 (CALS). Mixture was read at 510 nm. The reading was then noted in mmol/L. Normal value: 0.66 – 0.99 mmol/L
Statistical Analysis
The data was collected and reported as mean±standard deviation. One way ANOVA SPSS version 22.0 was used to find out the significant result. Continuous and numerical values were analyzed by student t-test while the categorical values were analyzed by chi square test and results were presented as frequency in percent and at 95% confidence interval. P- value <0.05 were considered as significant difference between the groups.
Results
The present study is concerned to evaluate the demographical and biochemical assessment between the case control chronic migraine patients in comparison to normal subject. The demographic evaluation among the groups were gender, age distribution, body weight and body mass index while the biochemical assessment include determination of cholecalciferol, calcium and magnesium levels in the serum of both groups.
Demographical Assessment
The gender distribution of study subject male and female between controls (group A) and migraine cases were noted as 15 and 15, 10 and 20 respectively with p- value of 0.39 (Table 1).
The age distribution in the study subject showed mean±SD age in the groups A and B was 71.50 ± 11.5 and 79.17 ± 12.46 kg respectively with t-value 0.53 and p- value of 0.138 (Table 1).
The body mass index among group A and B was found to be 28.47 ± 3.81and 29.71 ± 3.58 kg / m2 respectively with p-value 0.196 (Table 1).
| Variables | Control Subjects (Group-A) | Case Subjects(Groups -B) | P-value |
| Sample size (n) | 30 | 30 | - |
| Gender | 15(M)+15(F) | 10(M)+20(F) | 0.39 |
| Age (mean ± SD) | 38.8±9.64 | 40.2±10.7 | 0.49 |
| Body wt (kg) | 74.50±11.5 | 79.17±12.46 | 0.138 |
| BMI (kg/m²) | 28.47±3.81 | 29.71±3.58 | 0.196 |
Table 1: Demographic Variables of Control and Case Subjects.
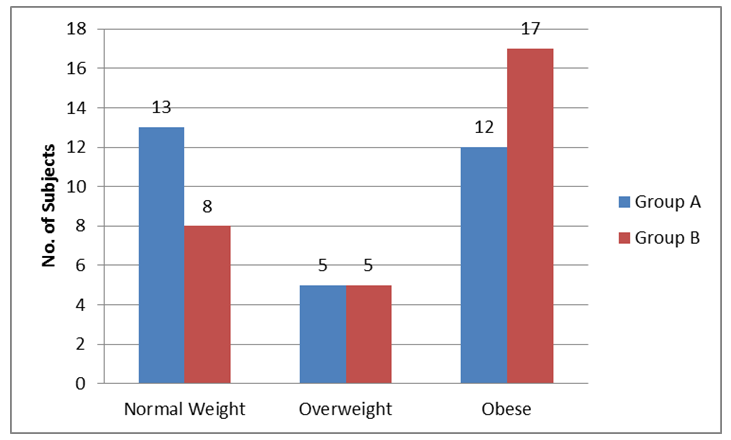
the persons as normal, over weight and obese (Table 2, Figure 1).
| Subjects (n=60) | Normal <25 (kg/m2) | Over Weight 25-29.9 (kg/m2) | Obese ≥30 (kg/m2) | P-value |
|---|---|---|---|---|
| Group -A (n=30) Control | 13 | 5 | 12 | 0.358 |
| Group -B (n=30) Chronic migraine | 8 | 5 | 17 |
Table 2: Categorial Characterization of person with nature of body mass index in the study group.
The mean±SD serum magnesium levels among both group of study subjects was found to be 1.88 ± 0.24 and 1.75 ± 0.20 mg/dl respectively with p-value of 0.022 (Table 3A).
Biochemical Assessment of case and control Subjects
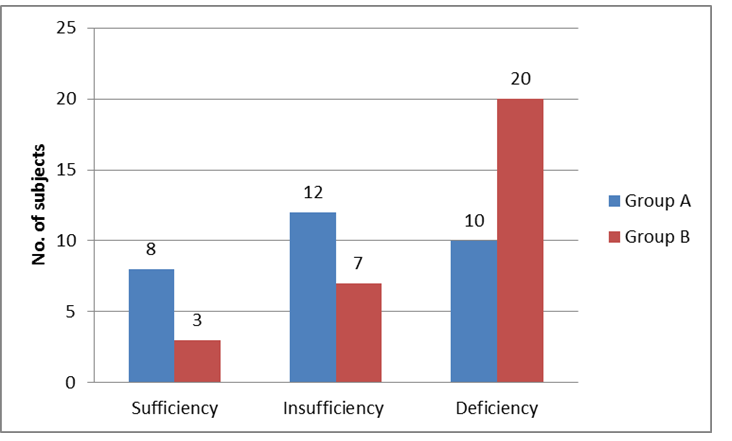
Serum cholecalciferol (ng/ml) : The mean±SD serum cholecalciferol level among groups A and B was noted as 23.94 ± 7.04 and 19.08 ± 6.33 ng / ml respectively with p- value 0.007 (Table 3A) The status of serum cholecalciferol in the serum of both subjects were also noted and classified according to the required quantity 30 ng / ml consider as sufficiency, 20 – 30 ng / ml insufficiency and < 20 ng / ml in the serum signify as deficient (Table 3B; Figure 2).
The mean±SD serum calcium level in both study group A and B was found to be 9.28 ± 0.67 and 8.89 ± 0.83 mg / dl respectively with p- value of 0.047 (Table 3A).
| Total Subjects (n=60) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Biochemical Variable | s | Normal Value | Group-A (n=30) | P-value | ||||||||||
| G | roups –B (n=30) Chronic Migrain | e | ||||||||||||
| Control | ||||||||||||||
| Serum Cholecalciferol | 31-60 ng/ml | 23.94 ± 7.04 | 19.08 ± 6.33 | 0.007 | ||||||||||
| Serum Calcium | 2.15-2.55mol/L | 9.28 ± 0.67 | 8.89 ± 0.83 | 0.047 | ||||||||||
| Serum Magnesium | 0.66 – 0.99 mmol/L | 1.88 ± 0.24 | 1.75 ± 0.20 | 0.022 |
Table 3A: Serum Cholecalciferol, Calcium and Magnesium in the Study Subjects.
| Subjects (n=60) | Sufficiency > 30 ng / ml | Insufficiency 20-30 ng / ml | Deficiency< 20 ng / ml | P | -valu | e | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group –A Control (n=30) | 8 | 12 | 10 | 0.029 | ||||||||||
| Group – B Control (n=30) | 3 | 7 | 20 |
Table 3B: Status of Serum Cholecalciferol in the Study Subjects.
Discussion
In the current study we have analyzed the serum cholecalciferol, calcium and magnesium levels in the patients of chronic migraine which is an episodic headache of vascular origin of unknown etiology and pathogenesis. In association with this unknown etiology present research accepted the alternative hypothesis because serum cholecalciferol, calcium and magnesium showed association with the severity of pain and other symptoms like nausea, vomiting, photophobia or phonophobia in chronic migrainuers. Various hypothesis reported that serum cholecalciferol has been associated with migraine such as decreased serotonin synthesis, modulation of nitric oxide and calcium channels within microcirculation. As exact mechanism in relation to migraine with serum cholecalciferol is still known, however few studies reported that there is a strong association with chronic pain [17, 26].
In the present study we have found many people who were affected with chronic migraine pain in the different age groups noted as 38 ± 9.64 and 40.2 ± 10.7 respectively with p-value 0.49. These findings are consistent with previous studies which also reported similar findings and association in different age group of persons with chronic migrainuers [27, 28].
The mean body weight and mean BMI in the study group of A and B are found consistent with previous studies [29, 30], however certain studies reported different body weight and BMI in chronic migrainuers while the mean BMI in the groups A and B was noted as 28.47 ± 3.81 and 29.71 ± 3.58 kg / m2 respectively with p- value 0.196. The findings are consistent with the previous study which also showed high BMI in chronic ± migrainuers [31, 32]. It has also been reported in few studies regarding the impact of vitamin D deficiency and frequency of headache in migrainuers [33, 34], as many studies reported that the relationship between serum vitamin D level and headache in still controversial [35, 36, 37]. However, present study is therefore taken into consideration to resolve this controversy.
The present study also aimed to evaluate serum cholecalciferol level with the association of pain in the chronic migrainuers. It has been observed that 90% of chronic migrainuers revealed deficiency or insufficiency of serum cholecalciferol compared to control subjects. This low serum cholecalciferol are consistent with Tozzi, et al. [38] which has also reported vitamin D to as low as < 10 ng / ml in migrainuers. Our findings also in tine and found consistent with previous studies [38] where insufficiency and deficiency of serum cholecalciferol were found in 67% of the population respectively.
In our study we investigated and think that vitamin D could be a better treatment option for headache especially for chronic migraine patients and this supposed to decrease the frequency and the severity of pain attack. Their findings thus support the present study as 90% of chronic patients showed deficiency or insufficiency of serum cholecalciferol as compared to 73% in control subjects. This is inconsistent with previous study reported from Pakistan and other countries [39]. In the current study we have also investigated the mean±SD serum magnesium level in both control and case groups and level of Mg++ in the serum was found to be as 1.88 ± 0.24 and 1.75 ± 0.20 ng/dl respectively with p-value 0.022. It has also been reported in this connection that prophylactic use of oral Mg++ or during an episode of headache was a useful approach that reduced the migraine attacks [40, 41]. According to a recent study it has been observed that the serum level of ionized Mg++ an active form of magnesium was not significantly different in migrainuers from those without migraine. This is in contrast to the present as well as previous studies. Low level of magnesium in the serum of chronic migraine patients has been reported by the previous study [42] and this finding also in line with the present study. In case of serum calcium level in both groups A and B was noted as 9.28 ± 0.67 and 8.89 ± 0.83 mg/dl with p-value 0.047. In the current study we have also investigated the role of calcium level in the serum of chronic migrainuers. Few studies in this connection reported that increased serum calcium in migraine is also the cause of migraine headache. This finding in contradistinction to the present and previous studies [43].
Conclusion
In conclusion, based on the results of the present study and other few studies we have agreed that mostly headache is basically related to the deficiency of vitamin D among migrainuers. The impact of vitamin D on the severity of migraine attacks is still not clear while the role of vitamin D in several neurological disorders has been widely investigated. The present study mentioned that the mean serum magnesium and calcium levels in migrainuers are significantly less as compared to normal persons. Few studies in this regard showed the association of vitamin D, calcium and magnesium in migraine patients separately but the present study is concerned with the association and quantification of all the parameters together in migraine patients. Therefore through this study it is recommended that all the parameters should provide beneficial tool in assessing the patients with migraine by the physicians.
References
-
Frediani F, Martelletti P, Bussone G (2004) Measure of negative impact of migraine on daily activities, social relationships and therapeutic approach. Neurol Sci 25(3): 249-250.
-
Martin S (2001) Prevalence of migraine headache in Canada. CMA J 164(10): 1481.
-
WHO (2016) Immunization, Vaccines and Biologicals. World Health Organization, Fact sheet: 1-2.
-
WHO (2006) Neurological disorders: a public health approach. Neurol Disord public Heal challenges pp: 41-176.
-
Gordon Smith K, Forty L, Chan C, Knott S, Jones I, et al. (2015) Rapid cycling as feature of bipolar disorder and comorbid migraine. J Affect Disord 175: 320-324.
-
Taga A, Russa M, Manzoni GC, Torelli P (2016) Cluster headache with accompanying migraine – like features : A possible clinical phenotype. Headache 57(2): 290- 297.
-
IHS (2013) Headache Classification Committee of the International Headache Society. International Classification of Headache Disorder 3rd (Edn.), Cephalagia 33: 629-808.
-
Lauritzen M (1994) Pathophyriology of the migraine aura. The spreading depression theory. Brain 117(1): 199- 210.
-
Weitzel KW, Thomas ML, Small RE, Goode JV (1999) Migraine: a comprehensive review of new treatment options. Pharmacotherapy 19(8): 957-973.
-
WHO (2016) Headache disorders. World Health Organization.
-
Steiner TJ (2007) Lifting the burden: The global campaign to reduce the burden of headache worldwide. J Headache Pain 6(5):373-377.
-
Holick MF (2007) Vitamin D deficiency. N Eng J Med 357(3): 266-281.
-
Milaneschi Y, Hoogendijk W, Lips P, Heijboer AC, Schoevers R, et al. (2014) The association between low vitamin D and depressive disorders. Mol Psychiatry 19(4): 444-451.
-
Holick MF (2017) The vitamin D deficiency pandemic approaches for diagnosis, treatment and prevention. Rev Endoer Metab Disord 18(2): 153-165.
-
Battoult S, Whiting SJ, Peltier SL, Sadrin, Gerber G, et al. (2013) Cholecalciferol metabolism, functions and needs: From Science to health claims. Eur J Nutr 52(2): 429-441.
-
Buettner C, Brustein R (2015) Association of statin use and risk for severe headache or migraine by serum vitamin D status: a cross-sectional population- based study. Cephalagia 35(9): 757-766.
-
Adams JS, Hewison M (2010) Update in Vitamin D. J Clin Endocinol Metb 95(2): 471-478.
-
Reddy KS (2016) Global Burden of Disease Study 2015 provides GPS for global health 2030. Lancet 388(10053): 1448-1449.
-
Ashrafi MR, Najafi Z, Shafiei M, Heidari K, Togha M (2014) Cinnarizine versus Topiramate in the prophylaxis of migraine among children and adolescents : A randomized double blind clinical trial. Iran J Child Neurol 8(4): 18-27.
-
Slavin M, Bourguignon J, Jackson K (2016) Impact of food components on _in vitro_ calcitonin gene related peptide Secretion-A Potential Mechanism for Dietary Influence on Migraine. Nutrients 8(7): 406.
-
Natoli, JL, Marack A, Dean B, Buter Q, Turkel CC, et al. (2010) Global prevalence of chronic migraine: a systematic review. Cephalalgia 30(5): 599-609.
-
Wallace AM, Gibson S, de la Hunty A, Lamberg-Allardt C, Ashwelb M (2010) Measurement of 25-OH vitamin D in the clinical laboratory: Current Procedures, Performance characteristics and limitations. Steroids STE 75(7): 477-488.
-
Gindler EM, King JD (1972) Rapid calorimetric determination of calcium in biological fluids with methylol blue. Am J clin Pathol 58(4): 376-382.
-
Itani O, Tsang RC (2010) Bone disease-clinical chemistry: Theory analysis correlation 5th (Edn.), Mosby Inc pp: 614.
-
Ross AC, Manson JE, Arbams, Aloia JF, Brannon PM, et al. (2011) The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab 96(1): 53- 58.
-
Hewison M (2011) cholecalciferol and innate and adaptive immunity. Vitam Horm 86: 23-62.
-
Power SW, Coffey CS, Chamberlain LA, Ecklund DJ, Klingner EA, et al. (2017) Trial of Amitriptyline, Topiramate and placebo for pediatric migraine. N Eng J Med 376: 11-54.
-
Herekar AD, Herekar AA, Ahmad A, Uqaili UL, Alvi SZ, et al. (2013) The burden of headache disorder in Pakistan: methodology of a population – based nationwide study and questionnaire validation. J Headache Pain 14: 73-76.
-
Rao GN, Kulkarni GB, Guruaj G, Rajesh K, Stovner LJ, et al. (2012) The burden of headache disorders in India: methodology and questionnaire validation for a community – based survey in Karnataka state. J Headache Pain 13(7): 543- 550.
-
Sadaf N, Naureen A, Khalid S, Shahnaz A (2016) Frequency of cranial autonomic symptoms in migraine patients. Pak J Neurol Sci 11(2): 1-7.
-
Fayyazi A, Khajeh A, Ghazavi A, Sangestani M (2016) Omega 3 in childhood migraines: A double blind randomized clinical Trial. Iran J Child Neurol 10(1): 9- 13.
-
Charles A (2013) Migraine: A brain state. Curr Opin Neurol 26(3): 235-239.
-
Song TJ, Chu MK, Sohn JH, Ahn HY, Lee SH, et al. (2018) Effects of vitamin D deficiency on the frequency of headaches in migraine. J Clin Neurol 14(3): 366-373.
-
Gokhan Ozer (2018) The Impact of Serum 25- Hydroxyvitamin D Level on Migraine Headache. J Clin Exp Investig 9(1): 40-44.
-
Lannacchero R, Costa A, Galleli L, Squillace A, De Sarro G (2015) P060. Vitamin D deficiency in episodic migraine, chronic migraine and medication-overuse headache patients. J Headache Pain 16(1): 184.
-
Lippi G, Cervellin G, Mattiuzzi C (2014) NO evidence for an association of vitamin D deficiency and migraine. Biomed Res Int 14: 1-5.
-
Khorvash F, Mottaghi T, Askari G, Maracy MR, Nejad MA, et al. (2013) The association between serum vitamin D levels with general and abdomen obesity among patients with migraine. Int J Prev Med 4(2): 313-317.
-
Tozzi E, Boncristiano A, Antenucci AR, Farello G (2016) vitamin D 25 (OH) D serum level on headache children. J Headache Pain Manag 1: 1-5.
-
Zandifar A, Masjedi SS, Banihashemi M, Asgari F, Ebrahim H, et al. (2014) vitamin D status in migraine patients: A case control study. Biomed Res Int pp: 1-7.
-
Nagata E, Fujii N, Hosomichi K, Mitsunaga S, Suzuki Y, et al. (2014) Possible association between dysfunction of vitamin D binding protein and migraine attacks. Plos One 9(8): 105319.
-
Edlitz-Markus T, Haimi-Cohen Y, Zeharia A (2015) Association of age at onset of migraine with family history of migraine in children attending a pediatric headache clinic: A retrospective cohort study. Cephalalgia 35(8): 722-727.
-
Mauskop A, Varughese J (2012) Why all migraine patients should be treated with magnesium. J Neural Transm 119(5): 575-579.
-
Dhillon KS, Singh J, Lyall JS (2016) Treatment of clinical cases of migraine. J Headache Pain Manag 1: 2-4.
- Acido Labile or Gastro Irritant Apis and Enteric Release in Galenic Practice: An Overview
- A Study on Knowledge, Attitude and Practice of Hand Hygiene among Healthcare Professionals at a Tertiary Care Hospital, India
- Influence of Inoculum Concentration on In Vivo Incubation Period of Emmia lacerata, Pathogenesis and Management of Wilt in Pepper (Capsicum annuum L.)
- Vanilla’s Chemistry
- Marine Anti-Cancer Compounds and Adverse Effects of Global Warming on Oceans: An Overview
- Serological Investigation of Chikungunya Virus Antibody among Malaria-Suspected Febrile Patients in Some Healthcare Facilities in Rivers State