Epilepsy and Quinazolinones: The Renewable Relationship
Epilepsy is a global public health issue requiring a global response. Epilepsy is present everywhere and affects people of various ages, genders, ethnicities, and social backgrounds, regardless of geographical locations. Excess discharge from the cortical neurons in the cortical section of brain is generally responsible for epileptic state. Understanding the classification of epileptic seizures is the first step toward the correct diagnosis, treatment and prognostication of the condition. Specific seizure types or syndromes often respond better to specific medications or surgical approaches. Multidrug resistant syndrome and refractory epilepsy are the biggest challenge in treatment of epilepsy, they lead to defect access of Anti-Epileptic Drugs AEDs to their target in CNS. Moreover, the marketed drugs carry severe side effects such as drowsiness, hepatotoxicity, anemia, and teratogenicity. Therefore, there is pivotal need to discover more safe and effective drugs. Quinazolinones analogues represent molecules which are capable of binding at multiple sites with high affinity and facilitate more rapid discovery of useful medicinally active compounds. Series of new quinazolinone derivatives were synthesized by many sceintists around the world, screened virtually and evaluated for the anticonvulsant activity against different types of seizures. They are to be a vital part of the solution of epilepsy in the future.
Introduction
Prevalence and Incidence of Epilepsy
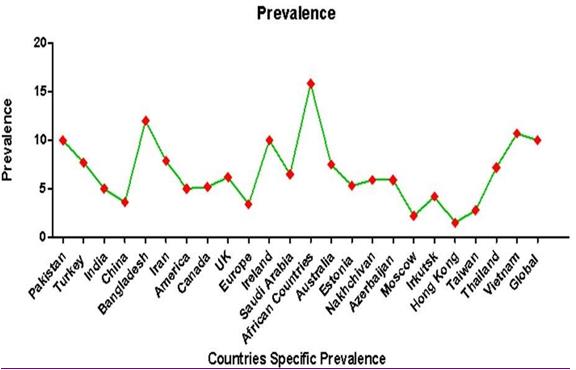
Epilepsy is a global public health issue requiring a global response. Epilepsy is present everywhere and affects people of various ages, genders, ethnicities, and social backgrounds, regardless of geographical locations [1]. It is the most common chronic serious neurological disease as it affected 50 million people worldwide and nearly 80% of them are found in developing regions2. Globally, an estimated 5 million people are diagnosed with epilepsy each year. In high-income countries, annual new cases are around 49 per 100,000 people in the general population. In low-income and middle-income countries, this figure can be up to 2 times higher as 139 per 100,000 [2, 3, 4]. This is likely due to the increased risk of endemic conditions, such as malaria or neurocysticercosis (NCC), the higher incidence of road traffic injuries and birth-related injuries in addition to that most people in developing countries with epilepsy receive no medical attention at all [5]. Consequently, although diagnostic and therapeutic innovations remain important goals, the greatest challenge for world health lies in appropriately identifying epileptic patients with providing the best available treatment [4, 6]. The prevalence of epilepsy in developed countries ranges from 4 to 10 cases per 1000, while in the developing and tropical countries studies have reported higher prevalence rates of epilepsy, ranging from 14 to 57 cases per 1000 persons [7, 9]. In Saudi Arabia the prevalence of epilepsy is 6.5 per 1000 and it is probably 2 times higher in children and young adult compared to other groups and with a lower rate in middle age people. The prevalence rate of epilepsy in Saudi Arabia is within the range reported in most other communities [10, 11, 12]. The prevalence of epilepsy of some countries is summarized in (Figure 1)[13].
The prevalence of active epilepsy is 6.4 per 1,000 and the lifetime prevalence is 7.6 per 1,000. The prevalence tends to increase with age, with peaks in the oldest age groups and in socially deprived individuals. The incidence of epilepsy is 61.4 per 100,000 person-years. Epilepsy has a bimodal distribution according to age with peaks in the youngest individuals and in the elderly. The increased incidence of seizures and epilepsy in the elderly can be attributed to the increase of age-related and aging-related epileptogenic conditions [14].
Causes of Epilepsy
Excess discharge from the cortical neurons in the cortical section of brain is generally responsible for epileptic state. Transition from normal behavior to seizure behavior may be caused by a number of factors including greater spread and neuronal recruitment secondary to a combination of enhanced connectivity, enhanced excitatory transmission, a failure of inhibitory mechanisms, and changes in intrinsic neuronal properties [18, 19].
Previously, the causes of epilepsy were classified as idiopathic, symptomatic, or cryptogenic [20]. The International League Against Epilepsy ILAE in 2010 proposed that to replace the old classification by the following categories: genetically, in which genetic factors have a major role in the causation of the epilepsy and in which the causative or susceptibility genes are inherited or result from de-novo mutations that might or might not be further inherited, structural or metabolic, in which there is a clear genetically or non- genetically determined cause that is structural or metabolic (e.g, stroke, trauma, brain tumor, aminoacidopathies), and unknown. The structural or metabolic categories are under discussion for further clarifying to extend and include immune and infectious causes [21].
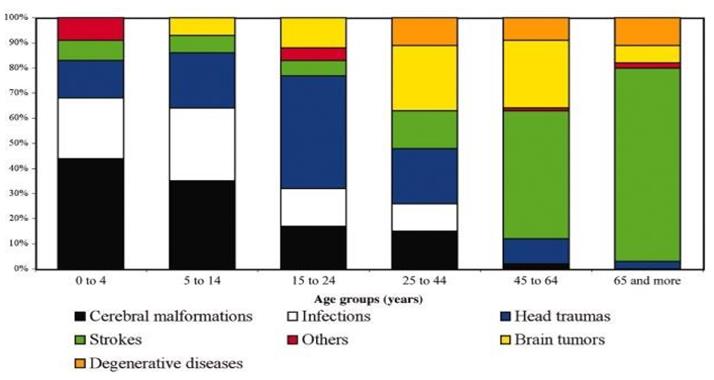
The likely underlying cause of epilepsy varies with age as shown in (Figure 2) [22]. Congenital factors (including genetic conditions) are predominating in infancy and perinatal stage. Idiopathic (genetic) epilepsies remain common in later childhood and adolescence but are the cause in only 20-30% of people with epilepsy overall. In middle life, trauma becomes more common as a cause of seizures (although it is only responsible for about 3-4% of cases in the population as a whole), while tumor, although the most feared cause of seizures, is responsible for only about 6% of incident cases of epilepsy (approximately 13% in the elderly). Cerebrovascular disease is the commonest identified etiology of seizures overall, being the cause in approximately 15%. In the older age groups, it is responsible for only 30-50% of cases. Even with modern neuroimaging and other modes of investigation, no cause can be identified in the majority of people developing seizures [23].
Classification of Epileptic Seizures
Understanding the classification of epileptic seizures is the first step toward the correct diagnosis, treatment and prognostication of the condition. Specific seizure types or syndromes often respond better to specific medications or surgical approaches. Some seizure types or syndromes carry a benign prognosis or high likelihood of seizure remission by a certain age. Other seizure syndromes may carry a far poorer prognosis, and early knowledge of this allows focused treatment and lifestyle modifications for patients and families [24]. A revised operational classification of seizure types was presented by the ILAE. The purpose of such a revision is to recognize that some seizure types can have either focal or generalized onset, to allow classification when the onset is unobserved, to include some missing seizure types, and to adopt more transparent names. Because current knowledge is insufficient to form a scientifically based classification, the 2017 Classification is operational (practical) and based on the 1981 Classification which extended in 2010 (Figure 3)[25].
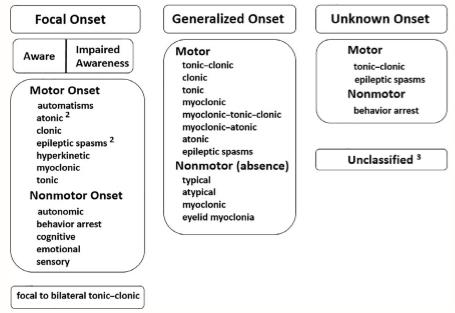
Partial (focal) seizure: Partial seizures have onset on one side of the brain, resulting in focal symptoms. Partial seizures are classified as simple or complex according to loss of consciousness. In simple partial seizure there is no alteration in consciousness or memory. It can be motor seizures with twitching, or non-motor with abnormal sensations; abnormal visions, and sounds or smells. Seizure activity can spread to the autonomic nervous system. Complex partial seizure characterized by loss or impaired of consciousness and involuntary motor actions (Automatism) [23, 26, 27].
Treatment of Epilepsy
The objective of treatment is to bring the electrical activity in the brain under control while maintaining quality of life. The standard medical treatment of epilepsy is with antiepileptic drugs (AEDs), which are known generally as anticonvulsants. Antiepileptic drugs can be effective, but like all drugs acting on central nervous system (CNS) have side effects. Although the majority of people with epilepsy can anticipate good seizure control with the correct antiepileptic drugs, about 30% of people continue to have seizures. Non- pharmacological treatments which include ketogenic diet, surgical resection, and vagal nerve stimulation can be helpful to reduce seizure frequency for patients with refractory seizures [15, 28].
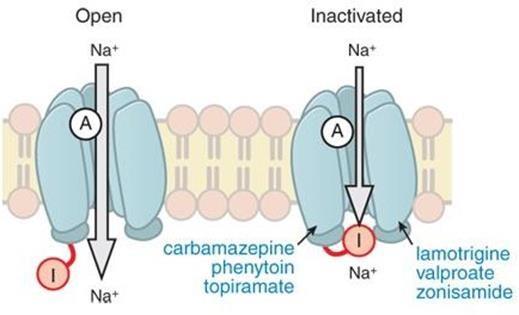
Antiepileptic drugs (AEDs): AEDs are the first choice of treatment of epilepsy. The main goal of anticonvulsant treatment is a significant reduction in seizure frequency and severity and maintaining normal lifestyle for epileptic patient. The selection of AED is principally determined by several factors including efficacy, toxicity, type of seizure, the Physicist’s familiarity with drug, and AED cost [29, 30]. All AEDs have the ability to decrease neuronal excitation or increase neuronal inhibition by one or more of pharmacological processes, including modification of voltage-gated ion channels (Na+, Ca+2, K+), potentiation of GABA-ergic activity, inhibition of glutamatergic process and modification of neurotransmitter release [31]. A new AED is successful if it has at least one of the following properties: greater efficacy than other drugs in the treatment refractory epilepsy, the ability to prevent or delay the epileptic onset, broad usefulness in other non- epileptic CNS disorders, fewer side effects than available drugs and ease of use such as linear pharmacokinetic, lack of drug interaction and once or twice daily dosing [32, 33]. Mechanism of Action of AEDs • Voltage Gated Na+ Channels Ion channels are extremely important membrane integral proteins that regulate trans-membrane potential of the cell. Voltage gated Na+ channels generate the upstroke of the action potential by allowing Na+ to rapidly enter the cell upon reaching the threshold voltage. Some AEDs are thought to principally affect the voltage- dependent Na+ channels. The traditional AEDs, Phenytoin and Carbamazepine are thought to exert their anti- epileptic effects by prolonging the inactivation of Na+ channels that may account for the termination of the sustained, rapid and repetitive firing induced in neurons by a trans-membrane current pulse. At high concentrations, Valproate could contribute to the long- lasting inactivation of Na+ channels. Lamotrigine one of the newer AEDs, also prolongs the inactivation of Na+ channels. Abolition of the sustained, rapid and repetitive firing of isolated neurons was also observed with, Topiramate and Zonismaide (Figure 4). These drugs block high-frequency repetitive spike firing, which is believed to occur during the spread of seizure activity, without affecting ordinary on-going neural activity. This elucidates their ability to protect against seizures without causing a generalized impairment of brain function [34, 35, 36].
in AED action has not been elucidated. The low-voltage calcium channel T-type opens with slight depolarization, and are quickly inactivated. The low-threshold Ca2+current regulate repetitive electrical activity of thalamic neurons and probably participate in generating generalized absence seizures. Ethosuximide is one of AEDs that inhibit this T- calcium channel, (Figure 5)[35, 36, 37].
Voltage gated calcium channels molecular structure and mechanism of inactivation are similar to the voltage- gated sodium channels. They are divided into several subtypes, L, N, P/Q, T and R, according to their electrophysiological characteristics. Blockade of N or P/Q channels inhibits the presynaptic release of excitatory amino acids. However, a potential role for these channels
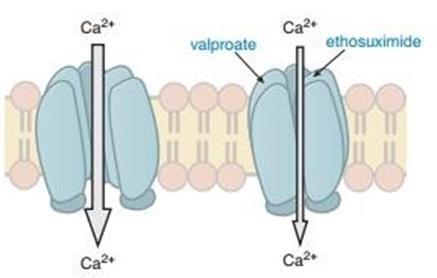
Figure 5: anti-epileptic drugs enhanced Ca+2 channel inactivation. • Potassium Channels γ-Aminobutyric acid 1 (GABA) is recognized as the main inhibitory neurotransmitter in the cerebral cortex. GABA is formed within GABA-ergic axon terminals by decarboxylation of glutamic acid by glutamic acid decarboxylase (GAD) to GABA. It is released into the synaptic junction and then acts at one of two types of GABA receptors: GABAA receptors and GABAB receptors. The GABAA receptors are ligand-gated ion channels that

• Glutamate Receptor
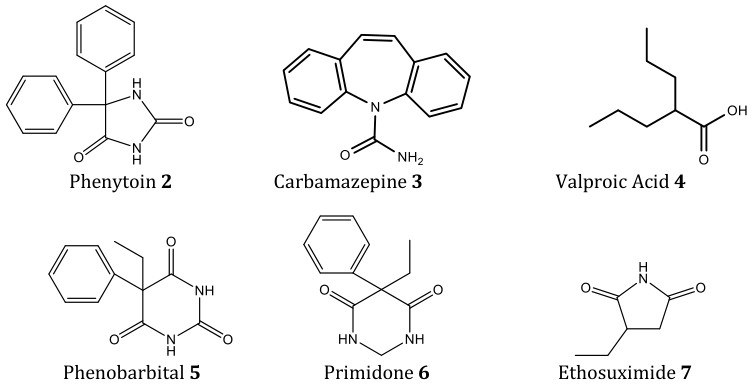
Glutamate is the main excitatory neurotransmitter in the CNS. When Glutamate binds to glutamate receptors, the receptors facilitate the flow of both sodium and calcium ions into the cell, while potassium ions flow out of the cell, resulting in excitation. Four glutamate receptor types have been identified within the CNS. Three of these receptors, α-amino-3-hydroxy-5- methyl- 4isoxazolepropionic acid (AMPA), N-methyl-D-aspartate (NMDA), and kainate, are coupled to ion channels. The fourth type of glutamate receptor is the metabotropic glutamate receptor that acts via G protein influence on various second messenger systems and ion channel activity. AEDs that modify these receptors are antagonistic to glutamate [40, 41]. • Synaptic Vesicles Protein 2A (SV2A) Most of the first generation or old AEDS are very effective and continue to be used up-to- date. These include phenytoin 2, Carbamazepine 3, Valproate 4, Benzodiazepines, Phenobarbital 5, Primidone 6, and Ethosuximide 7. The drawbacks for these drugs are there effect on metabolic enzymes either induction or inhibition. That makes new alternative antiepileptic recommended [44, 45]. The clinical indications and efficacy of these drugs are summarized in (Table 1) [46].
SV2 is an integral membrane protein present on all synaptic vesicles; it is consisting of three isoforms, designated SV2A, SV2B, and SV2C. SV2A is the most widely distributed isoform, being nearly ubiquitous in the CNS; SV2A appears to be integral to the process of neurotransmitter exocytosis into the synaptic cleft. Inhibition of this protein appears to result in abroad- spectrum attenuation of excitatory activity. Levetiracetam is the first of several agents able to inhibit the synaptic vesicle protein 2A (SV2A) as well as Brivaracetam [42]. • Classification of Antiepileptic Drugs It is very difficult to classify AEDs depending on their mechanism of action because some of them act by several mechanisms, new modes of action are discovered, and in some cases the mechanisms of anticonvulsant action are incompletely described. All these facts make the mechanism-based selection of anticonvulsant drugs a difficult mission [43]. They are classified chronologically to the following generations:
• First Generation
| Antiepileptic Drugs | Partia | l | Generalized toinc-clonic | Absence | Myoclonic | Tonic/ atonic | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Phenytoin | X | X | _ | _ | _ | ||||||||||||
| Carbamazepine | X | X | _ | _ | _ | ||||||||||||
| Valproate | X | X | X | X | X | ||||||||||||
| Benzodiazepines | A | _ | E | A | A | ||||||||||||
| Phenobarbital | X | X | _ | _ | X | ||||||||||||
| Primidone | X | X | _ | E | _ | ||||||||||||
| Ethosuximide | _ | _ | X | _ | _ |
Table 1: Efficacy and indication of antiepileptic drugs by seizure type (United State or European indication) A: adjunctive only,
• Second Generation
The choice of AEDS was limited to the old agents till the new second generation discovered and approved. These include Felbamate 8, Gabapentin 9, Lamotrigine 10, Topiramate 11, Tiagabine 12, Oxcarbazepine 13, Levetiracetam 14, Pregabalin 15, Zonisamide 16 and Vigabatrin17. They are better tolerated and safer than old drugs. They also have advantages of fewer side effects (table 2) minimum drug interactions in addition to the wide spectrum of activity. All the drugs in this group are approved to manage partial seizure. Falbamate, lamotrigine and Topiramate are used to control generalized seizure in addition to the partial type [47, 48, 49, 50, 51].
| AED | Serious | Non serious | ||||||
|---|---|---|---|---|---|---|---|---|
| Felbamate | Aplastic anemia, hepatotoxicity | Anorexia, insomnia | ||||||
| Gabapentin | Sedation, weight gain | |||||||
| Lamotrigine | Stevens-Johnson syndrome | Insomnia | ||||||
| Topiramate | Kidney stones, glaucoma | Paresthesia, cognitive impairment, weight loss | ||||||
| Tiagabine | Spike-wave stupor | Tremor, sedation, impaired Concentration | ||||||
| Levetiracetam | Sedation, behavioral change | |||||||
| Oxcarbazepine | Hyponatremia, rash | Ataxia, diplopia | ||||||
| Zonisamide | Kidney stones Rash | Paresthesia, weight loss | ||||||
| Pregabalin | Sedation, weight gain |
Table 2: Summary of adverse effects.
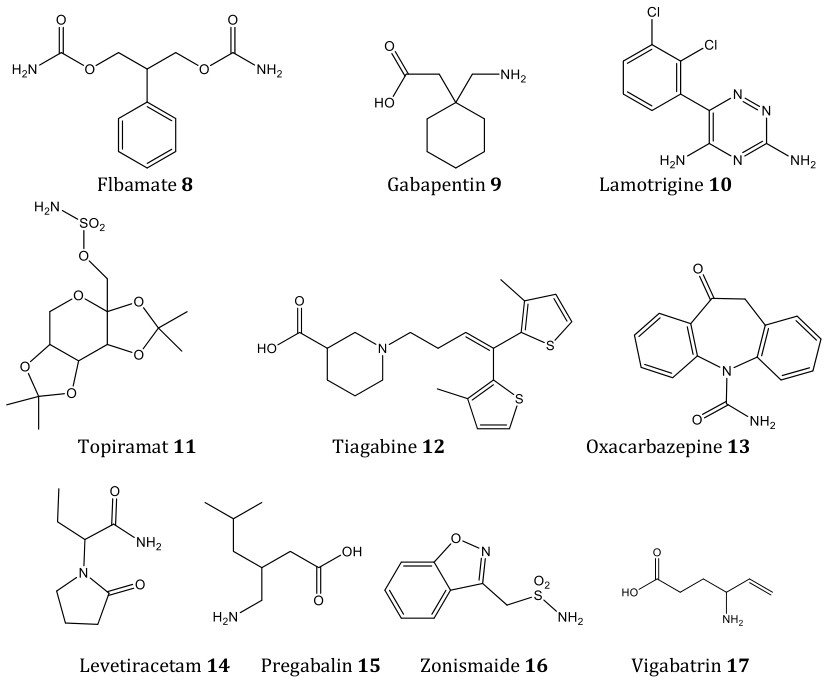
Levetiracetam 14 Pregabalin 15 Zonismaide 16 Vigabatrin 17
• Third Generation
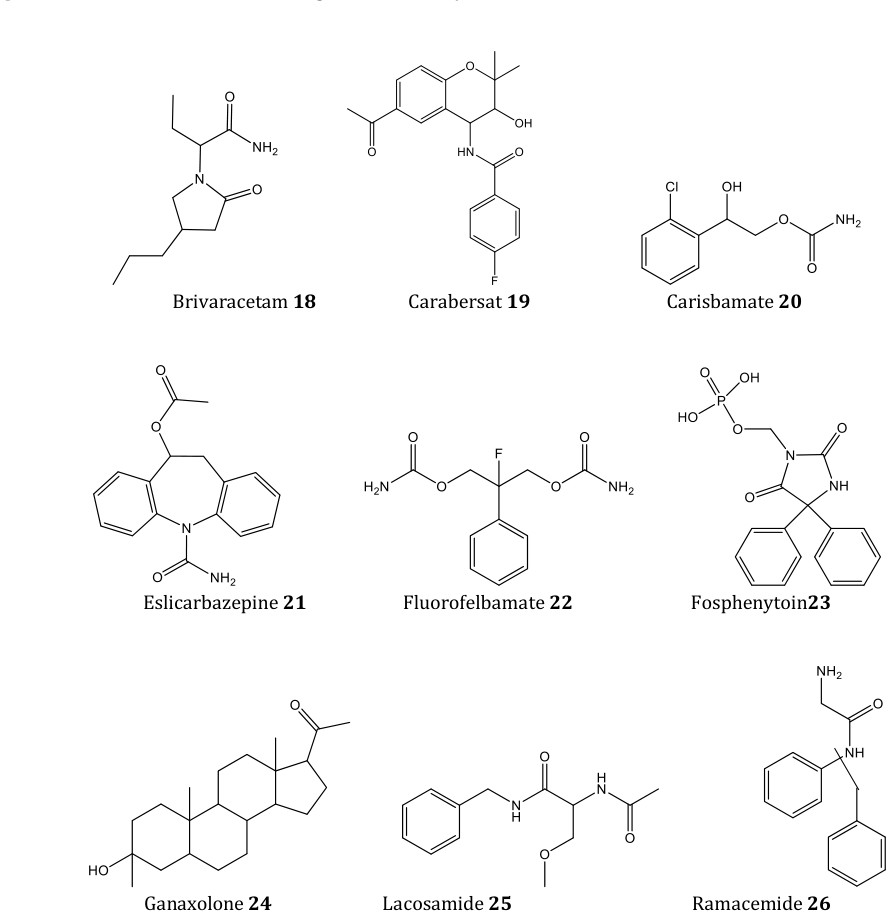
There are advanced AEDs have been developed and licensed latterly by pharmaceutical companies, which include Brivaracetam 18, Carabersat 19, Carisbamate 20, Eslicarbazepine 21, Fluorofelbamate 22, Fosphenytoin 23, Ganaxolone 24, Lacosamide 25, Remacemide 26, Retigabine 27, Rufinamide 28, Safinamide 29, Seletracetam 30, Soretolide 31, Talampanel 32, Stiripentol 33 Valrocemide 34 and Losigamone 35. They present a new and preferable approach to curing epilepsy, these attributed to their multiple diverse molecular mechanisms of action. Comparing to previous generations of AEDs the third-generation agents show superior tolerability, milder side effects, less drug and hormone interactions and enhance pharmacokinetics profiles [52, 53, 54]. The mechanism of action of AEDs of different generations could be summarized in (Table 3) [42].
| Mechanism of action | Effect on neuronal transmission | First-generation AEDs | Second/third- generation AED | s |
|---|---|---|---|---|
| Na+ channel blocked (fast inactivation) | Slowed recovery from inactivated state | Phenytoin | Topiramate | |
| Carbamazepine | Zonisamide | |||
| Valproate | Oxcarbazepine | |||
| Lamotrigine | ||||
| Felbamate | ||||
| Rufinamide | ||||
| Ca+2 channel blocked | Post-synaptic inhibitory action | Ethosuximide (T- type) Valproate | Topiramate | |
| Zonisamide | ||||
| Gabapentin | ||||
| Lamotrigine | ||||
| Pregabalin | ||||
| GABA agonism/potentiatio | Inhibitory activity by permitting n hyperpolarization | Benzodiazepines | Felbamate | |
| Barbiturates | Topiramate | |||
| Valproate | Vigabatrin | |||
| Stiripentol | ||||
| Retigabine | ||||
| NMDA receptor Blockade | Decreased excitatory synaptic activity | Felbamate | ||
| AMPA receptor Blockade | Decreased excitatory synaptic activity | Topiramate | ||
| SV2 A vesicle Inhibition | Decreased excitatory synaptic activity | Levetiracetam Seletracetam | ||
| Sodium channel Blockade (slow inactivation) | Recovery of neurons Oxcarbazepine from prolonged depolarization | Lacosamide | ||
| Potassium channel Blockad | e | Retigabine |
Table 3: Summary of antiepileptic drugs' proposed mechanisms
New Concept for Developing Anticonvulsant Drugs
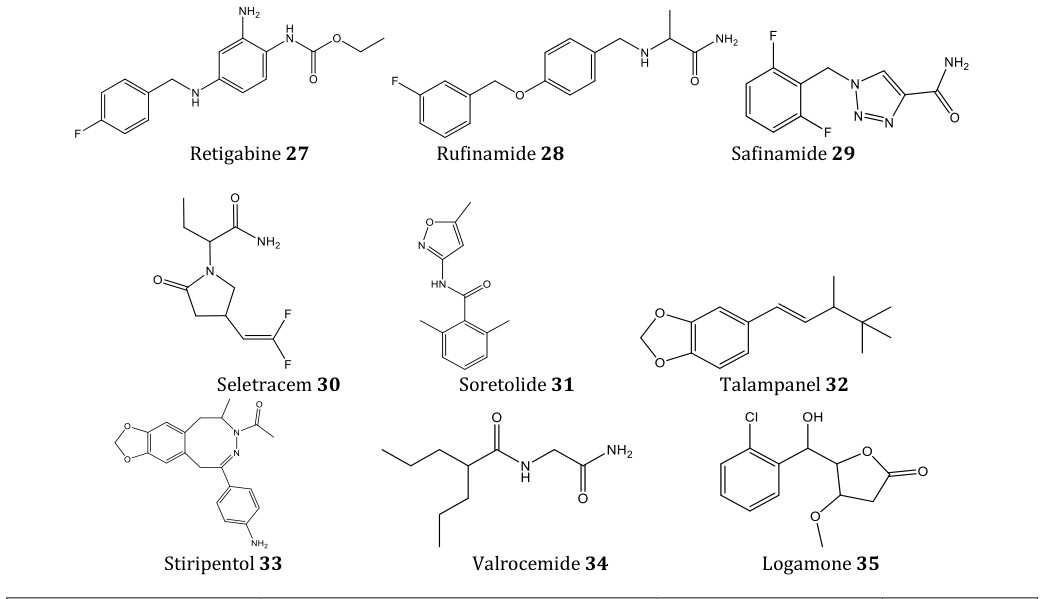
Although there are more than 20 approved AEDs with different chemical structures and targets of mechanism, they can provide seizure control for 60 - 70% of patients. Multidrug resistant syndrome and refractory epilepsy are the biggest challenge in treatment of epilepsy, they lead to defect access of AED to their target in CNS. Moreover, the marketed drugs carry severe side effects such as drowsiness, hepatotoxicity, anemia, and teratogenicity. Therefore, there is pivotal need to discover more safe and effective drugs [33, 55, 56]. It is difficult to use rational methodologies in the discovery of new antiepileptic drugs; this is attributed to the insufficient information on the cellular mechanism of epilepsy in human with the complex mechanism of action of most of the antiepileptic drugs. Consequently, another design approach based on the existence of different pharmacophores that were established through the analysis of structural characteristics of clinically effective drugs as well as other antiepileptic compounds was adopted. In the literatures, it is well documented that one of the important core fragments is defined by the presence of hydrogen donor/acceptor unit, one electron donor atom, and a hydrophobic domain (aryl ring substituted/un- substituted). These structural features were found in the first-generation drugs such as Carbamazepine or Phenytoin, and the newest drugs e.g, Felbamate and Retigabine (Figure 7) [43, 57, 58].
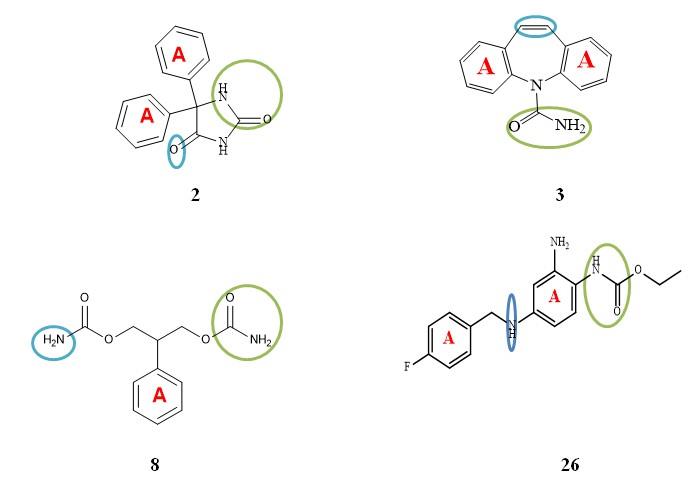
Compounds contain heterocyclic quinazolines and quinazolinones are considering available scaffolds in drug research as they possess vital pharmacological properties.
These nucleuses can be termed as ‘Master key’ for antiepileptic therapy as it is an important scaffold of many reported anticonvulsant drugs (Figure 8) [59, 60].
Chemistry of Quinazolinone
Quinazolinone and their derivatives represent a building block for more or less 150 naturally occurring alkaloids isolated from numerous families of plant kingdom, animals and microorganisms []. Quinazolinone is a heterocyclic chemical compound with two joined aromatic rings, benzene ring and pyrimidine ring 36, and one of the carbons oxidized to ketone oxygen. This 4-oxo derivative of quinazoline is called 4(3_H_)- quinazolinone 37.
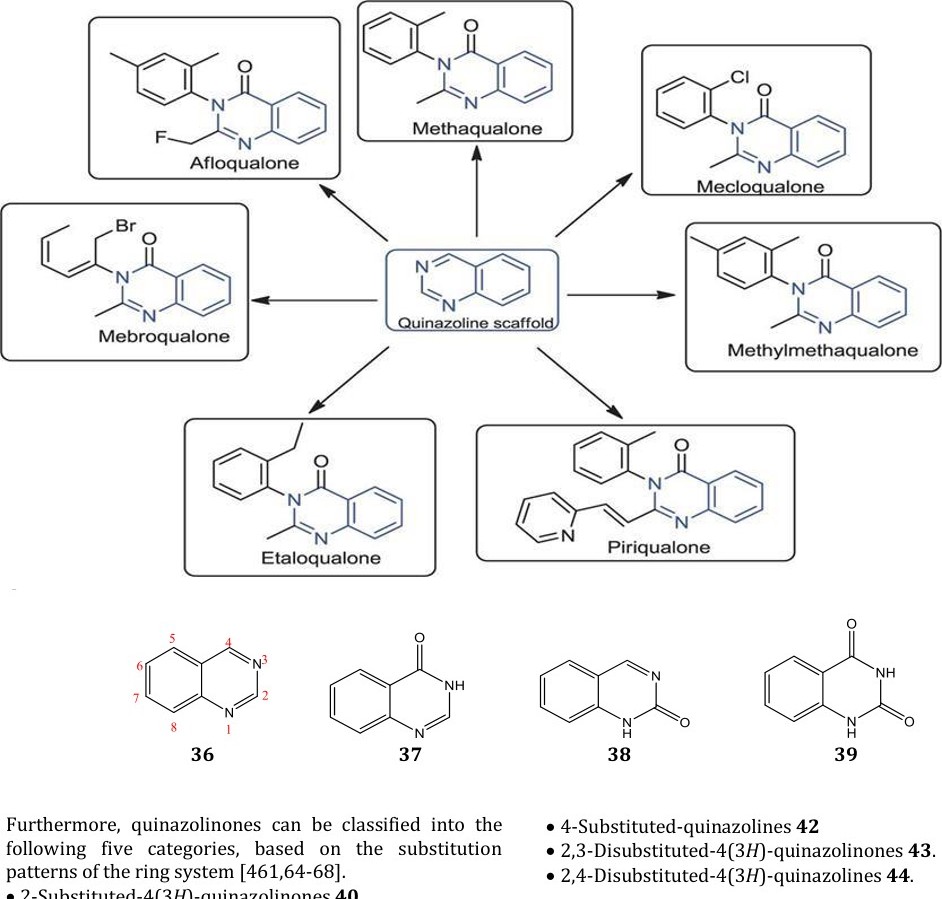
According to the keto or oxo group position, these compounds may be classified into three types: 2(1_H_) quinazolinones 38, 4(3_H_) quinazolinones 37 and 2, 4(1_H_, 3_H_) quinazolinediones 39. The 4(3_H_) quinazolinones are most abundant and significant in medicinal chemistry possessing a multitude of pharmacological action. Moreover, they are prevalent either as intermediates or as natural products in many proposed biosynthetic pathways.
40 41 42
43 44
Utility of qunazolinones in medicinal chemistry was triggered in the early of 1950s with discovery of febrifugine 45, a quinazolinone alkaloid, which was isolated from the Chinese plant Aseru (Dichroa febrifuga _Lou_r) and was reported to possessing antimalarial potential [72]. Moreover, trypanthrin 46 has been the active principle of a Japanese traditional herbal remedy for fungal infections. It also has antibacterial, antitubercular and antileishmanial activities. Deoxyvascinon 47 has been extensively used in herbal medicines for cough, cold, bronchitis and asthma [73].
Physical Properties of Quinazolinone
Commonly, quinazolinones are solid in nature with high melting points. These are water insoluble substances but readily soluble in alkali and form stable salts. Moreover, quinazolinones are stable to distillation
Biological Activity of Quinazolinone Ring
45 46 47
Quinazolinones analogues have been described as privileged structures. These structures represent molecules which are capable of binding at multiple sites with high affinity and facilitate more rapid discovery of useful medicinally active compounds [74].
On the bases of various literature survey, quinazolinones derivatives show various pharmacological activities such as antimalarial [75], anti-inflammatory [76], anticonvulsant [77], sedative and hypnotic [78], antihypertensive [79], anti-diabetic [80], antimicrobial [81, 82, 83, 84, 85], antioxidant [86], anticancer [87, 88, 89], anti- histamine [90], anti-asthmatic [91], and anti- parkinsonism [92]. Furthermore, several of these compounds exhibited dihydrofolate reductase inhibition [93, 94], and also used as kinase inhibitors [95] . Presently, a large number of quinazolinone derivatives are patented and available in the market as potential drugs for various diseases (Table 4) [69, 96].
| Name of drug | Category | Structure | ||||||
|---|---|---|---|---|---|---|---|---|
| Metolazone | Diuretic | |||||||
| Prazosin | Antihypertensive | |||||||
| Gefitinib | Tyrosine kinase inhibitor: anticancer | |||||||
| Proquazone | NSAID |
Table 4: Successful quinazolinone based clinically available drugs.
Quinazolin-4(3_H_)-one constitutes a good template for the preparation of some new anticonvulsant agents, since
48 49
50 51 52 R= 4-Ph 54 R=Ph 53 R = 4-Cl 55 R= 4-F-Ph 56=R =4-Cl-Ph
Novel derivatives of 6,8-diiodo-2-methyl-3-substituted benzyl-quinazolin-4(3_H_)-ones were synthesized by Zayad et al, and evaluated for their anticonvulsant activity by the MES-induced seizure and SC PTZ tests. The neurotoxicity was assessed using rotarod test. All the tested compounds showed considerable anticonvulsant activity in at least one of the anticonvulsant tests. Compounds 57-59 proved to the most potent compounds of this series with relatively low neurotoxicity with the reference drugs. The presence of electron-withdrawing group at aromatic ring enhanced the activity when compared to un-substituted or electron-donating group in the benzyl ring [103].
57 R= 4-Cl
58 R= 4-F 59 R= 4-Br
SCPTZ- induced seizures, Methaqualone and Sodium Valproate were taken as reference drugs. Compounds 60- 62 was found to be the most potent compound of the series accompanied with relatively low toxicity as compared with the reference drugs. Moreover, the obtained results showed that compounds 60-62 could be useful as a model for future design, optimization, and that compounds 63 and 64 having R = ethyl and n-propyl groups, respectively were found to be the most active of the series with no motor impairment effect. Moreover, they showed reduced CNS depressant effect in comparison to the standard drug Carbamazepine. On the basis of these finding, it can be conclude that the activity may be attributed to the presence of adequate long and straight aliphatic chain ethyl and propyl that provide adequate lipophilicity which lead to enhancement in the blood brain barrier (BBB) crossing capacity of the compounds in addition to well fitted to receptor site [109].
63 R = C2H5 64 R = C3H7
Novel 2,3,8- trisubstituted-4(3H)-quinazolinone derivatives were prepared by El-Azab et al, the compounds assessed as antiepileptic agents, being compared with the reference drugs Methaqualone and Sodium Valproate. Compounds 65 -67 produced the strongest activity in this class with relatively low neurotoxicity. The structural activity correlation revealed that compounds having acetic acid hydrazide fragments at position 8 possess significant anticonvulsant activity 65- 67. More interestingly, the ester or thioester of acetic acid hydrazide such as compounds, 66 and 67 showed the most potent activity in compared with its parent acetic acid hydrazide 65; this may be attributed to their high lipid solubility [110].
73: R = Cl 75: R = I 74: R = F 76: R= Br
site, hydrogen bonding domain, an electron donor group and another hydrophobic-hydrophilic site controlling the pharmacokinetic properties of the anticonvulsants. Findings of this study indicated that different substitutions on the distal aromatic ring resulted in variation in antiepileptic effect. The simple phenyl ring with fluoro or chloro substitution in _para-_position exhibited the most potent activity and did not exhibit neurotoxicity at highest administered dose [114].
Khan et al, reported 25 new synthesis derivatives of quinazolinon-4(3H)-one and evaluated for anticonvulsant activity of the synthesized compounds, it was observed that compounds, 90 and 91 proved to be of clinical significance. The quinazolinone nuclei pretended as the mainstay for the inducing the anticonvulsant activity. The introduction of the benzyloxy tetrazole moiety as the core fragment synergized the activity. The amplification of the anticonvulsant stimulus attributed to the presence of the free carbonyl. Moreover, the major role was played by the heterocyclic pyridinyl moiety conjugated through the alkyl linkage to the tetrazole nuclei [97].
90 91
1. Perucca E, Covanis A, Dua T (2014) Commentary: Epilepsy is a Global Problem. Epilepsia 55 (9): 1326- 1328.
2. WHO (2019) Epilepsy. World Health Organization.
3. Thijs RD, Surges R, O'Brien TJ, Sander JW (2019) Epilepsy in adults. lancet 393(10172): 689-701.
4. Singh A, Trevick S (2016) The Epidemiology of Global Epilepsy. Neurol Clin 34(4): 837-847.
5. Beghi E, Giussani G, Abd-Allah F, Abdela J, Abdelalim A, et al. (2019) Global, regional, and national burden of epilepsy, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 18(4): 357-375.
6. Tellez-Zenteno JF, Hernandez-Ronquillo L (2017) Epidemiology of neurocysticercosis and epilepsy, is everything described? Epilepsy Behav 76: 146-150.
7. Bell G, Sander J (2001) CPD-Education and self- assessment The epidemiology of epilepsy: the size of the problem. Seizure 10(4): 306-316.
8. Burneo JG, Tellez-Zenteno J, Wiebe S (2005) Understanding the burden of epilepsy in Latin America: a systematic review of its prevalence and incidence. Epilepsy Res 66(1-3): 63-74.
9. Carpio A, Hauser WA (2015) Epilepsy in the developing world. Curr Neurol Neurosci Rep 9(4): 319-326.
10. Khan SA (2015) Epilepsy awareness in Saudi Arabia.
Neurosciences 20(3): 205-206.
11. Benamer HT, Grosset DG (2009) A systematic review of the epidemiology of epilepsy in Arab countries. Epilepsia 50(10): 2301-2304.
12. Alshahrani AM, Pathan A, Alruwais JF, Alduhayshi
AM (2019) Knowledge, attitude, and believes of epilepsy in local communities of Saudi Arabia. J Family Med Prim Care 8(3): 1065-1069.
13. Shakirullah S, Khan A, Nabi M (2014) The
prevalence, incidence and etiology of epilepsy. Int J Clin Exp Neurol 2(2): 29-39.
14. Beghi E, Giussani G (2018) Aging and the Epidemiology of Epilepsy. Neuroepidemiology 51(3- 4): 216-223.
15. Lawal M (2005) Management and treatment options for epilepsy. Br J Nurs 14(16): 854-858.
16. De Boer HM, Mula M, Sander JW (2008) The global burden and stigma of epilepsy. Epilepsy Behav 12(4): 540-546.
17. Brown C (2016) Pharmacological management of epilepsy. Prog Neurol Psychiatry 20(2): 27-34c.
18. Huang H, Zhou H, Wang N (2015) Recent advances in epilepsy management. Cell Biochem Biophys 73(1): 7- 10.
19. Farghaly WM, Elhamed MAA, Hassan EM, Soliman
WT, Yhia MA, et al. (2018) Prevalence of childhood and adolescence epilepsy in Upper Egypt (desert areas). Egypt J Neurol Psychiat Neurosurg 54(1): 34.
20. (1989) Proposal for revised classification of epilepsies and epileptic syndromes. Commission on Classification and Terminology of the International League Against Epilepsy. Epilepsia 30(4): 389-399.
21. Moshé SL, Perucca E, Ryvlin P, Tomson T (2015)
Epilepsy: new advances. lancet 385(9971): 884-898.
22. Major P, Thiele EA (2007) Seizures in Children:
Determining the variation. Pediatr Rev 28(10): 363- 371.
23. Hart YM (2012) Epidemiology, natural history and classification of epilepsy. Medicine 40(9): 471-476.
24. Rudzinski LA, Shih JJ (2010) The classification of seizures and epilepsy syndromes. Continuum (Minneapolis, Minn.) 16(3 Epilepsy): 15-35.
25. Fisher RS, Cross JH, French JA, Higurashi N, Hirsch E,
et al. (2017) Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia 58(4): 522- 530.
26. Shneker BF, Fountain NB (2003) Epilepsy. Dis Mon
49(7): 426-478.
27. Fisher R, Saul M (2010) Overview of epilepsy.
Comprehensive Epilepsy Center Stanford Neurology: Stanford. pp 1-56.
28. Smithson WH, Walker MC (2012) ABC of Epilepsy.
John Wiley & Sons: Chichester, West Sussex, UK, 201: 1-48.
29. Asconape JJ (2002) Some common issues in the use of antiepileptic drugs. Semin Neurol 22(1): 27-39.
30. Wang Y, Chen Z (2019) An update for epilepsy research and antiepileptic drug development: Toward precise circuit therapy. Pharmacol Ther 201: 77-93.
31. Brodie MJ (2010) Antiepileptic drug therapy the story so far. Seizure 19(10): 650-655.
32. Bialer M, White HS (2010) Key factors in the discovery and development of new antiepileptic drugs. Nat Rev Drug Discov 9(1): 68-82.
33. Perucca E, French J, Bialer M (2007) Development of new antiepileptic drugs: challenges, incentives, and recent advances. Lancet Neurol 6(9): 793-804.
34. Moulard B, Bertrand D (2002) Epilepsy and sodium channel blockers. Expert Opin Ther Pat 12(1): 85-91.
35. Rogawski MA, Löscher W (2004) The neurobiology of antiepileptic drugs. Nat Rev Neurosci 5(7): 553- 564.
36. Hilal-Dandan R, Brunton L (2013) Goodman and Gilman Manual of Pharmacology and Therapeutics. 2nd (Edn.), McGraw Hill Professional: Philadelphia.
37. Lasoń W, Chlebicka M, Rejdak K (2013) Research
advances in basic mechanisms of seizures and antiepileptic drug action. Pharmacol Rep 65(4): 787- 801.
38. Barrese V, Miceli F, Soldovieri MV, Ambrosino P,
Iannotti FA, et al. (2010) Neuronal potassium channel openers in the management of epilepsy: role and potential of retigabine. Clin Pharmacol 2: 225-236.
39. Treiman DM (2001) GABAergic mechanisms in epilepsy. Epilepsia 42(3): 8-12.
40. Lasoń W, Dudra-Jastrzębska M, Rejdak K, Czuczwar
SJ (2011) Basic mechanisms of antiepileptic drugs and their pharmacokinetic/pharmacodynamic interactions: an update. Pharmacol Rep 63(2): 271- 292.
41. White HS, Smith MD, Wilcox KS (2007) Mechanisms
of action of antiepileptic drugs. Int Rev Neurobiol 81: 85-110.
42. Cook AM, Bensalem-Owen MK (2011) Mechanisms
of action of antiepileptic drugs. Therapy 8(3): 307- 313.
43. Estrada E, Peña A (2000) In silico studies for the rational discovery of anticonvulsant compounds. Biorg Med Chem 8(12): 2755-2770.
44. Löscher W (1998) New visions in the pharmacology of anticonvulsion. Eur J Pharmacol 342(1): 1-13.
45. Abou-Khalil B (2017) Old-Generation Antiepileptic
Drugs. In: Koubeissi MZ, Azar NJ, (Eds.), Epilepsy Board Review: A Comprehensive Guide, 1st ( Edn.), Springer: New York, pp: 213-223.
46. Abou-Khalil B, Schmidt D (2012) Antiepileptic drugs:
advantages and disadvantages. In: Stefan H, Theodore W, (Eds.), Handbook of Clinical Neurology, Elsiver: Amsterdam 108, pp: 723-739.
47. Sirven JI, Fife TD, Wingerchuk DM, Drazkowski JF
(2007) Second-generation antiepileptic drugs' impact on balance: a meta-analysis. Mayo Clin Proc 82(1): 40-47.
48. Bialer M (2006) New antiepileptic drugs that are second generation to existing antiepileptic drugs. Expert Opin Investig Drugs 15(6): 637-647.
49. Gerlach AC, Krajewski JL (2010) Antiepileptic Drug
Discovery and Development: What Have We Learned and Where Are We Going? Pharmaceuticals (Basel) 3(9): 2884-2899.
50. LaRoche SM (2007) A new look at the second- generation antiepileptic drugs: a decade of experience. Neurologist 13(3): 133-139.
51. LaRoche SM, Helmers SL (2004) The new antiepileptic drugs: scientific review. Jama 291(5): 605-614.
52. Luszczki JJ (2009) Third-generation antiepileptic drugs: mechanisms of action, pharmacokinetics and interactions. Pharmacol Rep 61(2): 197-216.
53. Vohora D, Saraogi P, Yazdani MA, Bhowmik M,
Khanam R, et al. (2010) Recent advances in adjunctive therapy for epilepsy: focus on sodium channel blockers as third-generation antiepileptic drugs. Drugs Today (Barc) 46(4): 265-277.
54. Vardanyan R, Hruby V (2016) Antiepileptic Drugs. In
Synthesis of Best-Seller Drugs, Academic press: Boston pp: 155-177.
55. Mahato AK, Srivastava B, Nithya S (2011) Chemistry,
structure activity relationship and biological activity of quinazoline-4 (3H)-one derivatives. Inventi Rapid Med Chem 2(1): 400-402.
56. Espinosa-Jovel C, Toledano R, Aledo-Serrano A,
Garcia-Morales I, Gil-Nagel A (2018) Epidemiological profile of epilepsy in low income populations. Seizure 56: 67-72.
57. Abbas SES, Awadallah FM, Ibrahim NA, Said EG,
Kamel G (2013) Design and synthesis of some 3- substituted-2-[(2, 4-dichlorophenoxy)-methyl] quinazolin-4 (3H)-one derivatives as potential anticonvulsant agents. Chem Pharm Bull 61(7): 679- 687.
58. Pandeya SN, Raja AS, Stables JP (2002) Synthesis of isatin semicarbazones as novel anticonvulsants-role of hydrogen bonding. J Pharm Pharm Sci 5(3): 266- 271.
59. Ugale VG, Bari SB (2014) Quinazolines: New
horizons in anticonvulsant therapy. Eur J Med Chem 80: 447-501.
60. Kamel M, Zaghary W, Al-Wabli R, Anwar M (2016)
Synthetic approaches and potential bioactivity of different functionalized quinazoline and quinazolinone scaffolds. Egypt Pharmaceut J 15(3): 98-131.
61. Chawla A, Batra C (2013) Recent advances of quinazolinone derivatives as marker for various biological activities. Int Res J Pharm 4(3): 49-58.
62. Mhaske SB, Argade NP (2006) The chemistry of recently isolated naturally occurring quinazolinone alkaloids. Tetrahedron 62(42): 9787-9826.
63. Khan I, Ibrar A, Ahmed W, Saeed A (2015) Synthetic
approaches, functionalization and therapeutic potential of quinazoline and quinazolinone skeletons: the advances continue. Eur J Med Chem 90: 124-169.
64. Arora R, Kapoor A, Gill N, Rana A (2011)
Quinazolinone: an overview. Int Res J Pharm 2(12): 22-28.
65. Asif M (2014) Chemical characteristics, synthetic methods, and biological potential of quinazoline and quinazolinone derivatives. Int J Med Chem pp: 27.
66. Rajput R, Mishra AP (2012) A review on biological activity of quinazolinones. Int J Pharm Pharm Sci 4(2): 66-70.
67. Tiwary B, Pradhan K, Nanda A, Chakraborty R
(2015) Implication of quinazoline-4 (3H)-ones in medicinal chemistry: a brief review. J Chem Biol Ther 1: 104-110.
68. Eguchi S (2006) Quinazoline alkaloids and related chemistry. In Bioactive Heterocycles I, Springer: Berlin, Heidelberg pp: 113-156.
69. Sharma PC, Kaur G, Pahwa R, Sharma A, Rajak H
(2011) Quinazolinone analogs as potential therapeutic agents. Curr Med Chem 18(31): 4786- 4812.
70. Ajani OO (2016) Quinazoline pharmacophore in therapeutic medicine. Bangladesh J Pharmacol 11(3): 716-733.
71. Vijayakumar B, Prasanthi P, Teja KM, Reddy M,
Nishanthi M, et al. (2013) Quinazoline derivatives and pharmacological activities: a review. IJMCA 3(1): 10- 21.
72. Koepfli J, Mead J, Brockman JA (1947) An alkaloid with high antimalarial activity from Dichroa Febrifuga1. J Am Chem Soc 6(7): 1837-1837.
73. Potewar TM, Ingale SA, Srinivasan KV (2008)
Synthesis of tryptanthrin and deoxyvasicinone by a regioselective lithiation-intramolecular electrophilic reaction approach. Arkivoc 2008(14): 100-108.
74. Jafari E, Khajouei MR, Hassanzadeh F, Hakimelahi
GH, Khodarahmi GA (2016) Quinazolinone and quinazoline derivatives: recent structures with potent antimicrobial and cytotoxic activities. Res Pharm Sci 11(1): 1-14.
75. Verhaeghe P, Azas N, Gasquet M, Hutter S, Ducros C,
et al. (2008) Synthesis and antiplasmodial activity of new 4-aryl-2-trichloromethylquinazolines. Bioorg Med Chem Lett 18(1): 396-401.
76. Alagarsamy V, Raja Solomon V, Sheorey R,
Jayakumar R (2009) 3‐(3‐Ethylphenyl)‐2‐substituted hydrazino‐3H‐quinazolin‐4‐one Derivatives: New Class of Analgesic and Anti‐Inflammatory Agents. Chem Biol Drug Des 73(4): 471-479.
77. Georgey H, Abdel-Gawad N, Abbas S (2008)
Synthesis and anticonvulsant activity of some quinazolin-4-(3H)-one derivatives. Molecules 13(10): 2557-2569.
78. Ochiai T, Ishida R (1982) Pharmacological studies on
6-amino-2-fluoromethyl-3-(O-tolyl)-4 (3H)- quinazolinone (afloqualone), a new centrally acting muscle relaxant.(II) Effects on the spinal reflex potential and the rigidity. Jap J Pharmacol 32(3): 427- 438.
79. Ismail MA, Barker S, Abou El Ella DA, Abouzid KA,
Toubar RA, et al. (2006) Design and synthesis of new tetrazolyl-and carboxy-biphenylylmethyl-quinazolin- 4-one derivatives as angiotensin II AT1 receptor antagonists. J Med Chem 49(5): 1526-1535.
80. Malamas MS, Millen J (1991) Quinazolineacetic acids and related analogs as aldose reductase inhibitors. J Med Chem 34(4): 1492-1503.
81. Patel NB, Patel JC (2011) Synthesis and antimicrobial activity of Schiff bases and 2- azetidinones derived from quinazolin-4(3H)-one. Arabian J Chem 4(4): 403-411.
82. Raghavendra NM, Thampi P, Gurubasavarajaswamy
PM, Sriram D (2007) Synthesis and antimicrobial activities of some novel substituted 2-imidazolyl-N- (4-oxo-quinazolin-3 (4H)-yl)-acetamides. Chem Pharm Bull 55(11): 1615-1619.
83. Nanda A, Ganguli S, Chakraborty R (2007)
Antibacterial activity of some 3-(Arylideneamino)-2- phenylquinazoline-4 (3H)-ones: synthesis and preliminary QSAR studies. Molecules 12(10): 2413- 2426.
84. Ilango K, Valentina P, Umarani N, Beena K (2010)
Eco-benign mediated versatile synthesis of newer quinazolin-4-(3H)-one clubbed isatin derivatives as potent antimicrobial agents. Int J Res Pharm Sci 1(2).
85. Nadendla RR, Mukkanti K, Rao GS, Babu AN (2010)
Microwave Synthesis of some new Quinazolinone Formazans for their Antimicrobial and Antihelminthic Activities. Curr Trends Biotechnol Pharm 4(1): 545- 550.
86. Saravanan G, Alagarsamy V, Prakash CR (2010)
Synthesis and evaluation of antioxidant activities of novel quinazoline derivatives. Int J Pharm Pharm Sci 2(4): 83-86.
87. Alafeefy AM, Ashour AE, Prasad O, Sinha L, Pathak S,
et al. (2015) Development of certain novel N-(2-(2-(2- oxoindolin-3-ylidene) hydrazinecarbonyl) phenyl)- benzamides and 3-(2-oxoindolin-3-ylideneamino)-2- substituted quinazolin-4 (3H)-ones as CFM-1 analogs: Design, synthesis, QSAR analysis and anticancer activity. Eur J Med Chem 92: 191-201.
88. Mahdavi M, Pedrood K, Safavi M, Saeedi M, Pordeli
M, et al. (2015) Synthesis and anticancer activity of N- substituted 2-arylquinazolinones bearing trans- stilbene scaffold. Eur J Med Chem 95: 492-499.
89. Yin S, Zhou L, Lin J, Xue L, Zhang C (2015) Design,
synthesis and biological activities of novel oxazolo [4, 5-g] quinazolin-2 (1H)-one derivatives as EGFR inhibitors. Eur J Med Chem 101: 462-475.
90. Alagarsamy V, Parthiban P, Solomon VR, Dhanabal K,
Murugesan S, et al. (2008) Synthesis and pharmacological investigation of novel 4‐(4‐Ethyl phenyl)‐1‐substituted‐4H‐[1, 2, 4] triazolo [4, 3‐a]‐quinazolin‐5‐ones as new class of H1‐antihistaminic agents. J Heterocycl Chem 45(3): 709-715.
91. Rayees S, Satti NK, Mehra R, Nargotra A, Rasool S, et al. (2014) Anti-asthmatic activity of azepino [2, 1-b] quinazolones, synthetic analogues of vasicine, an alkaloid from Adhatoda vasica. Med Chem Res 23(9): 4269-4279.
92. Kumar S, Kaur H, Singh I, Sharma M, Vishwakarma P,
et al. (2009) Synthesis, characterization and biological activity of various substituted quinazolinone derivatives containing dopamine moiety. World J Chem 4(2): 195-200.
93. Al-Rashood ST, Aboldahab IA, Nagi MN, Abouzeid LA,
Abdel-Aziz AA, et al. (2006) Synthesis, dihydrofolate reductase inhibition, antitumor testing, and molecular modeling study of some new 4 (3H)- quinazolinone analogs. Biorg Med Chem 14(24): 8608-8621.
94. Gangjee A, Kothare M, Kisliuk RL (2000) The
synthesis of novel nonclassical reversed bridge quinazoline antifolates as inhibitors of thymidylate synthase. J Heterocycl Chem 37(5): 1097-1102.
95. Khalil AA, Hamide SGA, Al‐Obaid AM, El‐Subbagh HI
(2003) Substituted Quinazolines, Part 2. Synthesis and In‐Vitro Anticancer Evaluation of New 2‐Substituted Mercapto‐3H‐quinazoline Analogs. Arch Pharm (Weinheim) 33 (2): 95-103.
96. Panneer Selvam T, Kumar PV (2011) Quinazoline
marketed drugs-A review. Res Pharm 1(1): 1-21.
97. Malik S, Khan SA (2014) Design and evaluation of new hybrid pharmacophore quinazolino-tetrazoles as anticonvulsant strategy. Med Chem Res 23(1): 207- 223.
98. Kashaw SK, Kashaw V, Mishra P, Jain N, Stables J
(2009) Synthesis, anticonvulsant and CNS depressant activity of some new bioactive 1-(4-substituted- phenyl)-3-(4-oxo-2-phenyl/ethyl-4H-quinazolin-3- yl)-urea. Eur J Med Chem 44(11): 4335-4343.
99. Gujural M, Sareen K, Kohli R (1957) Evaluation of anticonvulsant activity of 2, 3-di-substituted quinazolones: a new class of anticonvulsant drugs. Indian J Med Res 45(2): 207.
100. Salimath R, Patel S, Shah N (1956) Synthesis of 6-
halogenated-2, 3-disubstituted-4-quinazolinones III. J Ind Chem Soc 33: 140-146.
101. Barthwal J, Tandon S, Agarwal V, Dixit K, Parmar SS
(1973) Relationship between CNS depressant and enzyme inhibitory properties of substituted quinazolone 1, 3, 4-oxadiazoles. J Pharm Sci 62(4): 613-617.
102. Wolfe JF, Rathman TL, Sleevi MC, Campbell JA,
Greenwood TD (1990) Synthesis and anticonvulsant activity of some new 2-substituted 3-aryl-4 (3H)- quinazolinones. J Med Chem 33(1): 161-166.
103. Zayed M, Ahmed H, Omar A, Abdelrahim A, El-Adl K
(2013) Design, synthesis, and biological evaluation studies of novel quinazolinone derivatives as anticonvulsant agents. Med Chem Res 22(12): 5823- 5831.
104. Jatav V, Mishra P, Kashaw S, Stables J (2008)
Synthesis and CNS depressant activity of some novel 3-[5-substituted 1, 3, 4-thiadiazole-2-yl]-2-styryl quinazoline-4 (3H)-ones. Eur J Med Chem 43(1): 135- 141.
105. Pandey S, Shukla S, Pandey D, Srivastava R (2011)
Studies on anticonvulsant agents. Achievements and prospects. Russ Chem Rev 80(2): 187.
106. Kumar P, Pandeya S (2010) Anticonvulsant and Neurotoxicity Evaluation of Some Novel 3- {[Substituted]-Amino}-2-Phenyl-3H-Quinazolin-4- one. Int J Pharmacol Biol Sci 4(3): 55-61.
107. El-Azab AS, ElTahir KE (2012) Design and synthesis of novel 7-aminoquinazoline derivatives: antitumor and anticonvulsant activities. Bioorg Med Chem Lett 22(5): 1879-1885.
108. Patel HM, Noolvi MN, Shirkhedkar AA, Kulkarni AD,
Pardeshi CV, et al. (2016) Anti-convulsant potential of quinazolinones. RSC Adv 6(50): 44435-44455.
109. Gupta D, Kumar R, Roy RK, Sharma A, Ali I, et al.
(2013) Synthesis and biological evaluation of some new quinazolin-4 (3H)-ones derivatives as anticonvulsants. Med Chem Res 22(7): 3282-3288.
110. El-Azab AS, ElTahir KE (2012) Synthesis and anticonvulsant evaluation of some new 2, 3, 8- trisubstituted-4 (3H)-quinazoline derivatives. Bioorg Med Chem Lett 22(1): 327-333.
111. Kadi AA, El-Azab AS, Alafeefy AM, Abdel-Hamide S
(2009) Synthesis and biological screening of some new substituted 2-Mercapto-4-(3H)-quinazolinone analogs as anticonvulsant agents. Az J Pharm Sci 34: 135-155.
112. Zayed MF (2014) New fluorinated quinazolinone derivatives as anticonvulsant agents. J Taibah Univ Med Sci 9(2): 104-109.
113. El-Azab AS, Abdel-Hamide SG, Sayed-Ahmed MM,
Hassan GS, El-Hadiyah TM, et al. (2013) Novel 4 (3H)- quinazolinone analogs: synthesis and anticonvulsant activity. Med Chem Res 22(6): 2815-2827.
114. Prashanth M, Madaiah M, Revanasiddappa H,
Veeresh B (2013) Synthesis, anticonvulsant, antioxidant and binding interaction of novel N- substituted methylquinazoline-2, 4 (1H, 3H)-dione derivatives to bovine serum albumin: A structure– activity relationship study. Spectrochim Acta A Mol Biomol Spectrosc 110: 324-332.
- Acido Labile or Gastro Irritant Apis and Enteric Release in Galenic Practice: An Overview
- A Study on Knowledge, Attitude and Practice of Hand Hygiene among Healthcare Professionals at a Tertiary Care Hospital, India
- Influence of Inoculum Concentration on In Vivo Incubation Period of Emmia lacerata, Pathogenesis and Management of Wilt in Pepper (Capsicum annuum L.)
- Vanilla’s Chemistry
- Marine Anti-Cancer Compounds and Adverse Effects of Global Warming on Oceans: An Overview
- Serological Investigation of Chikungunya Virus Antibody among Malaria-Suspected Febrile Patients in Some Healthcare Facilities in Rivers State