Protective Action of Simvastatin in the Development of Aortic and Hepatic Lesions in Hypercholesterolemic Rabbits
As simvastatin is the most prescribed and distributed drug for high cholesterol by the National Health Service the authors carry out an experimental work to study special detailed effects of this drug. The authors studied the effect of simvastatin on the development of atherosclerotic lesions in aortas of rabbits submitted to a high-cholesterol diet, at 1.5%. The authors studied 30 New Zealand rabbits, males, adults, distributed in three groups according to diet: (A) cholesterol, (B) cholesterol + simvastatin (100 mg/day) and (C) normal. We took blood samples to evaluate cholesterol and plasma triglycerides at times zero, five and nine weeks and found lower serum cholesterol levels in the treated group. After nine weeks, we sacrificed the animals and examined the aortas for the extent of the atheromatous lesion area evaluated by computerized planimetry and the height of the lesion analyzed by morphometry, in histological sections of thoracic and abdominal aorta. There was no statistically significant difference between groups A and B in relation to the percentage of the injured area. However, in rabbits treated with simvastatin, smoother and less relief lesions were observed macroscopically by us and confirmed by morphometric analyses of atheroma plaque thickness. We observed intense morphological changes in the liver of the two groups of animals with a hypercholesterolemic diet, although to a slightly lower degree in those treated with simvastatin. We concluded that simvastatin had a protective effect on the volume of atherosclerotic lesions in aortas of hypercholesterolemic rabbits.
Introduction
As simvastatin is the most prescribed and distributed drug for high cholesterol by the National Health Service the authors carry out an experimental work to study special detailed effects of this drug [1]. With the use of hypocholesterolemic drugs, a reduction in clinical events is observed, explained by the relationship of lipid content and foamy cells of cleft plaques and the positive repercussions of this protective effect on plaques with “high risk” morphology. With such therapeutic intervention, such lesions are effectively stabilized and consequently, the incidence of clinical events is also decreased [2].
Several researchers have proven, through experimental investigations, that the reduction of blood lipids causes the regression of the atherosclerotic picture. After prolonged exposure to cholesterol-rich atherogenic diets, the animals now have plasma lipid levels higher than 600 mg/dl, with a large increase in coronary arterial collagen, elastin and cholesterol (most in esterified form). Later, when the animals switch to a vegetarian-type “regression diet”, plasma lipids fall rapidly to levels considered normal (140 mg/dl), but arterial lipids and connective tissue partially regress over 20 to 40 months. Histopathological evaluations, in turn, prove that the size of the atherosclerotic plaque is also reduced during this treatment regimen [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16].
Clarkson, et al. [7], studying lipid-fed primates, investigated to which plasma cholesterol levels should be reduced in so that arterial lesions regress. By repeated manipulation of the diet of animals with atherosclerosis, with serial measurements of plasma cholesterol, cholesterol levels were close to 7.8 mmol/l (300 mg/dl) or 5.2 mmol/l (200 mg/dl) during the regression phase of the experiment. These findings showed that when plasma cholesterol was kept high, the progression of atherosclerosis was slower, being interrupted in the second year. However, when cholesterol was kept lower, there was a regression of arterial lesions, more markedly in the second year. Therefore, serum cholesterol levels close to 200 mg/dl do not lead to a growth of pre-existing lesions, on the contrary, and may lead to regression of the lesion.
Still, it is already well established that high plasma cholesterol levels pose a risk for the development of atherosclerotic disease. Therefore, lipid-reducing therapy is expected to reduce the risk of atherosclerosis and its consequences, especially coronary heart disease and its peripheral vascular complications. In the “Coronary Primary Prevention Study of Clinical Studies of Lipid Research”, it was found in hypercholesterolemic men that a 1% decrease in plasma cholesterol levels reduces the risk of ischemic heart disease by 2%. Extrapolating this correlation to the general population, treatment with cholesterol-lowering drugs should substantially reduce the risk of ischemic heart disease in patients with hypercholesterolemia.
The “vastatins” represented by lovastatin, simvastatin and pravastatin constitute a very effective class of medicines in the treatment of hypercholesterolemia. These substances have different degrees of inhibitory activity on the limiting enzyme of cholesterol synthesis (Hydroxy Methyl Coenzyme Reductase - HMG-CoA reductase) and also on specific liver receptors, increasing the catabolism of Low Density Lipoprotein Cholesterol (LDL-c).
Lovastatin, simvastatin and pravastatin are drugs absorbed by hepatocytes by intermediate carrier transport mechanisms, thus having access to HMG-CoA hepatic reductase [17]. In contrast, the uptake of these three drugs by peripheral cells occurs by passive diffusion. Pravastatin, because it has a hydrophilic property, significantly limits its penetration into the lipid membranes of peripheral cells, unlike lovastatin and simvastatin that can easily penetrate peripheral cells. Due to this characteristic, the access of pravastatin in the undesired sites is restricted, avoiding unwanted side effects. On the other hand, lovastatin and simvastatin, because they present penetration into extrahepatic tissues, may be more act at the level of the fatty plaque, allowing its regression [18, 19].
The introduction of lovastatin in the United States in 1987 [20], and simvastatin in Europe in 1989 [21, 22] marked a new era in the treatment of hypercholesterolemia, competitively inhibiting the enzyme HMG-CoA reductase that controls intracellular cholesterol synthesis [23].
The active form of simvastatin specifically inhibits HMG- CoA reductase, the enzyme that catalyzes the conversion of HMG to mevalonate in the cholesterol biosynthesis pathway. At therapeutic doses, however, the drug does not completely block conversion. Thus, mevalonate is available in the biologically necessary quantities. The inhibiting action of simvastatin, occurring at an early stage of the cholesterol biosynthesis pathway and being rapidly metabolized to acetyl-CoA, does not cause accumulation of potentially toxic steroids to the body [24].
In clinical studies, simvastatin has been shown to be effective in the marked reduction of total cholesterol levels (32%) in LDL (40%), moderate decrease in triglycerides (18%) and moderate increase in High Density Lipoprotein Cholesterol (HDL-c) (14%) [21, 25].
Simvastatin, significantly reducing blood cholesterol levels in humans, has a protective effect on the inhibition and regression of atherosclerosis as observed in studies in patients with family homozygous hypercholesterolemia [26]. In a study with 4,000 patients with ischemic heart disease and hypercholesterolemia treated with simvastatin, observed over a period of three years, there was a reduction in fatal or non-fatal myocardial infarction and sudden death (Scandinavian Study) [19].
Similar results were observed in rabbits with diet-induced hypercholesterolemia supplemented with cholesterol and treated with three concentrations of simvastatin, with a dose-dependent inhibitory effect by simvastatin on atherosclerosis. In this study, it was observed that animals treated with simvastatin prevented an increase in serum cholesterol level, inhibiting the increase of Very Low Density Lipoprotein (VLDL) and LDL-c. At the dose of 10 mg/kg, the HDL-c level was slightly reduced compared to the control, but these values were significantly higher than the control group without an atherogenic diet. In this dose, inhibition of total cholesterol increase was found by 96%, which may be the cause of HDL-c elevation inhibition. As these animals presented a hyperlipidemia due to the diet, therefore an exogenous source, with a study of absorption of radiative cholesterol, the authors observed that simvastatin inhibited the absorption of cholesterol from the gastrointestinal wall, thus preventing exogenously induced hypercholesterolemia. It was also observed that the concentration of total cholesterol in the aortic wall was lower in the group treated with simvastatin at the concentration of 10 mg/kg and also prevented the development of atherosclerosis in the aorta and coronary arteries. Thus, the hypolipidemic effect of simvastatin is the main mechanism by which the development of atherosclerosis is inhibited [27].
Studying the action of three HMG-CoA reductase inhibitors (Lovastatin, Simvastatin, Pravastatin) in hypercholesterolemia and atherosclerosis in rabbits developed hyperlipidemic through diet, Thiery, et al. [28, 29] found lower concentration of beta-Very Low Density Lipoprotein (beta-VLDL) in treated animals. However, the study of the aortas showed fewer lesions and lower concentration of tissue cholesterol in animals treated with simvastatin and lovastatin.
In rabbits with hereditary hyperlipidemia (WHHL), Fukuo et al. [30], studied the correlation between lipid concentration and atherosclerosis in animals treated with simvastatin. In this study, rabbits at 3 and 10 months of age were used receiving simvastatin daily for 24 weeks, with a significant reduction in serum levels of total cholesterol, triglycerides and beta lipoproteins, with greater reduction in the group of younger animals. Also in this group, the extent of atheromatous lesions of the thoracic and abdominal aortas was smaller in the treated animals than in the control group. Therefore, the use of cholesterol-lowering drugs in hypercholesterolemic patients is indicated as a preventive measure against the development of atherosclerosis, as has been demonstrated in clinical and experimental studies.
Aims of the study
Based on studies of atherosclerosis induction in animal models and the possibility of using this model for the research of pharmacological agents in hyperlipidemia and atherogenic processes, we developed an experimental atherosclerosis protocol to analyze the effect of a hypocholesterolemic agent on the development of atherosclerosis. We studied the action of simvastatin in rabbits submitted to a high-cholesterol diet, analyzing its action in relation to the following aspects: a) Biochemical and hematological changes in blood samples taken during the observation period; b) Installation of atherosclerotic lesions in the aorta, evaluating the compromised area; c) Histopathological and morphometric analysis of the atheromatous lesion; d) Histopathological analysis of the liver.
Methods
Animals
The group consisted of thirty male rabbits, adults, New Zealand, weighing on average 3.0 kg. Upon arriving at our experimental laboratory, they were submitted to a prophylactic treatment with Tetmosol solution. After identification and after 15 days of acclimatization, the animals were distributed into three groups:
| Group A | Cholesterol 1,5% | |||
|---|---|---|---|---|
| n= 10 | T0 | T5 | T9 | Weeks |
| Group B | Cholesterol 1,5% + Simvastatin 10 mg/day | |||
| n= 10 | T0 | T5 | T9 | Weeks |
| Group C | Normal chow | |||
| n= 10 | T0 | T5 | T9 | Weeks |
During the experiment, there was loss of a group B animal, as a result of an accident in the manipulation of the rabbit, leaving this group with nine animals.
We kept the animals in individual wire cages. The cages remained in a ventilated place, and bowls were supplied with water and chow.
Diet
Common chow: The appropriate rabbit chow was manufactured by Nutriments Purina Ltda., whose basic composition consists of corn, dehydrated alfalfa, wheat bran, soybean meal, calcium carbonate, salt, molasses, vitamins and minerals.
1.5% cholesterol chow: We prepared the atherogenic chow at 1.5 g of cholesterol for every 100 g of chow, spraying, on the normal rabbit chow the cholesterol dissolved in chloroform, in the proportion of 1 g to 4.5 ml of chloroform. This mixture was prepared two days before consumption, for total evaporation of the solvent. We offer every morning 20 g of normal rabbit chow that served as placebo. We made the cholesterol chow every three days, packing it in plastic bags with 1200 grams, enough for a week.
Cholesterol chow 1.5% + simvastatin 10 mg/day: The simvastatin at the dosage of one tablet per day per rabbit (10 mg) was crushed by us, mixed with chloroform and incorporated into 20 g of chow, being administered daily to the animals.
Reagents
Pure substances
- Cholesterol PA - Merck - A 3670;
- Chloroform PA - Merck - Ref.21506;
- Sudam III PA - Merck - Ref. 15928;
- Hematoxylin - Eosin;
- Papaverine PA 50 mg/ml - ICM Biomed. Ind. Com, S/A;
- Xilol PA - Brazilian Chemical Union
- Absolute commercial alcohol;
- Commercial sulfuric ether.
Reagents Marketed: Reagents in kits marketed by Trilab and Abbott laboratories, used in the assays of total cholesterol, triglycerides, transaminases and gamma glutamyl transferase (GGT).
Specific diluents
Coulter T 890 Instrument-specific diluents for hemoglobin, hematocrit and white blood cell and platelet counts.
Conservation solutions
- 10% buffered formaldehyde solution
- Phosphate Buffer Saline Solution (PBS) pH 7.2
- Ethylenediamine tetraacetic acid (EDTA) - anticoagulant used in blood collection for hematological parameter assays.
Medicines and anesthetics
- Simvastatin - 10 mg
- Tetmosol - monosulfiram - Lab. Welcome I.C.I. Ltda. - topical use in dilution 1:3;
- Kaomagma — antidiarreic administered if necessary. - Fontoura Wyeth Laboratory. Usage: 1 teaspoon in 500 ml of water;
- Ketalar - injectable ketamine hydrochloride - use: 5 mg/ kg body weight;
• Rompum - hydrochloride of 2 - 2.6 - xyllidin - 5.6 - hydroxyhydro 4-4-1-3 thiazine - injectable. 2% aqueous solution - Bayer. Usage: 35 mg/kg body weight.
Stereo
- Centrifuge
- Automated Abbott for biochemical measurements of total cholesterol, triglycerides, transaminases and GGT;
- Coulter-series T 890 - automated quantitative analysis instrument for hematological assays;
- Common optical microscope for histopathological analysis and coupled to a cariometric eyefor morphometric analysis;
- Summographics Summasketch MM 1201 tablet coupled to microcomputer scan, version 3.0 by Jandel Scientilic.
Laboratory Methods
We performed biochemical measurements analyzing total cholesterol, triglycerides, glutamic-oxalacetic transaminase (GOT), pyruvic glutamic transaminase (PGT), GGT, hematocrit, hemoglobin, platelet and white blood cell count.
The collection was performed after fasting for 12 to 14 hours. We took a blood sample in EDTA for hematocrit, hemoglobin, white blood cell count and platelets. We collected 10 ml of blood that was left at rest at room temperature for retraction and centrifugation for 10 minutes at 3000 rpm to obtain the serum for biochemical assays of total cholesterol, triglycerides and enzymatics of transaminases and GGT. The methodology used in the assays was as follows: a) total cholesterol - dosed by specific automated colorimetric enzymatic method by hydrolysis of cholesterol esters in cholesterol; b) triglycerides - dosed by automated colorimetric enzymatic method automated by hydrolysis of triglycerides; c) Aspartate Aminotransferase (AST) or GOT and Serum glutamate pyruvate transaminase (SGPT), now called Alanine aminotransferase (ALT) or PGT, using specific substrates for each determination, obtaining as final product nicotinamide adenine dinucleotide (NAD+), whose formation speed is directly proportional to the amount of enzyme in the serum; d) GGT, the final product is p-nitroanilin, also proportional to the enzyme present in the serum.
Animal Sacrifice and Removal of Aortas
We weighed the animals weekly and the chow intake was also controlled by us weekly as well. We took blood samples at zero, five and nine weeks. At the time of sacrifice, we anesthetized the animals with Rompum (35 mg/kg weight) and Ketalar (5 mg/kg weight) intramuscularly. After anesthetized, they were attached to a channel for dissection. We performed laparotomy and isolation of the aorta from the aortic arch to the iliac bifurcation. Before being processed, the aortas were infused with a 12% papaverine solution in Phosphate Buffer Saline Solution - 37°C. We removed the aortas, opening them longitudinally, trapping them in sthene plates and fixing them in buffered formaldehyde for 24 hours.
Histopathological Analysis of the Aortas
Macroscopic evaluation: After fixation, the aortas were noded by us with Sudam III, so that the lipid content of the plaque was evidenced. We analyzed the stained aortas comparatively for macroscopic evaluation in relation to the intensity of presence of fatty plaques.
Evaluation of the extent of atheromatous lesions: The open, fixed and stained aortas were reproduced by us in acetate sheets, to quantify the extent of the affected aorta area through computerized planimetry, performed by us on a tablet coupled to a microcomputer. We expressed the results as a percentage of injured area in relation to the total area of the aorta.
Microscopic evaluation: We removed a transverse section of the aorta, with approximately 5 mm, from the region in the initial 2 cm corresponding to the thoracic aorta. This fragment presented a site with greater impairment within the delimited area. We removed the other fragment from the area between 7 and 12 cm from the aorta, corresponding to the abdominal aorta region. We process these fragments by conventional histological methods of paraffin inclusion and slides with hematoxylin and eosin, in which we performed histopathological analysis of changes in the intima and media layers of the aortas.
Evaluation of lesion height by morphometric method: We determined the height of the atheromatous lesion through a morphometric evaluation performed on histological sections obtained from fragments of the thoracic and abdominal aorta, with the aid of a karyometric eyepiece coupled to a common optical microscope. We used an 80x magnification and the results were expressed in micrometers (µm). We performed the determinations in the most representative plate of the histological section, in the one with the highest height. We measured the heights of the atheroma plates in the intimate layer and the thickness of the middle layer of the fragments corresponding to the thoracic and abdominal aorta.
Histopathological analysis of the liver: We fixed liver fragments in buffered formaldehyde and prepared slides with hematoxylin and eosin for histopathological study. We analyzed the following parameters: hydropic degeneration, steatosis, inflammatory infiltrate in parenchyma and portal space, expressing changes in mild (+), moderate (++) and intense (+++).
Statistical Analysis
In the analysis of the results, given the nature of the variables studied, we used the nonparametric tests, taking into account the nature of the distributions of the values or the variability of the measurements performed [31]. We apply the following tests:
1) Analysis of Variance by Kruskal-Wallis posts: in order to compare the values of the variables at times zero, five and nine weeks between the studied groups. When it showed significant difference, this analysis was complemented by the multiple comparison test[32]; 2) Analysis of Variance by Friedman posts: with the objective of comparing the time of experiment zero, five and nine weeks within each studied group A, B and C separately. This analysis when significant was complemented by the multiple comparison test [32]; 3) Mann-Whitney test for two independent samples: when we compared groups A and B in the variables of computerized planimetry and morphometric study of the aortas; 4) Wilcoxon test: in order to compare plaque thickness in the thoracic aorta region with abdominal aortic.
In all tests, we fixed the level of rejection of the null hypothesis at 5% (α ≤ 0.05) and marked the significant values with an asterisk.
Results
Biochemical Assays
Serum cholesterol levels: Serum cholesterol levels were dosed at times zero, five and nine weeks, and there was no statistically significant difference between groups A, B and C (52, 42, 41 mg/dl). However, after five weeks we observed a significant increase in the animals belonging to groups A and B (424 and 611 mg/dl), fed a hypercholesterolemic diet. After nine weeks, while in group A the cholesterol level increased significantly (1483 mg/dl) in group B, treated with simvastatin, the cholesterol level remained similar to that of the fifth week (661 mg/dl) (Table 1). Serum triglyceride levels: We found a slight increase in triglycerides in animals submitted to a hypercholesterolemic diet. After five weeks, a statistically significant increase was observed only in group A. After nine weeks, we found in groups A, B and C, respectively: 153 mg/dl, 113 mg/dl and 49 mg/dl (Table 2). Serum levels of transaminases and GGT: We observed an increase in got GOT, PGT and GGT transaminases in the group treated with simvastatin after nine weeks. Hematological Assays
We performed hemoglobin, hematocrit, platelet and white blood cell counts to control the clinical conditions of the animals, not finding any serious alterations that could compromise the development of the experiment. We verified in groups A and B, who received a hypercholesterolemic diet, a slight reduction in hemoglobin and hematocrit assays.
Weight Control and Chow Consumption
We did not observe weight loss in the three groups studied, remaining around 3200 to 3400 grams, despite the decrease in daily consumption of hypercholesterolemic diet.
Macroscopic Evaluation of Aortic Lesions
We performed a macroscopic examination of the aortas and observed, after nine weeks of atherogenic diet, a large lipid deposition in the arterial intima in both hypercholesterolemic groups (Figures 1A-1C). In group A, we noticed lesions with higher number and intensity in the aortic arch region, being less pronounced in the most distal sections of the artery. In group B, the lesions were moderate with distinctly lower, smoother and sparse plaques.
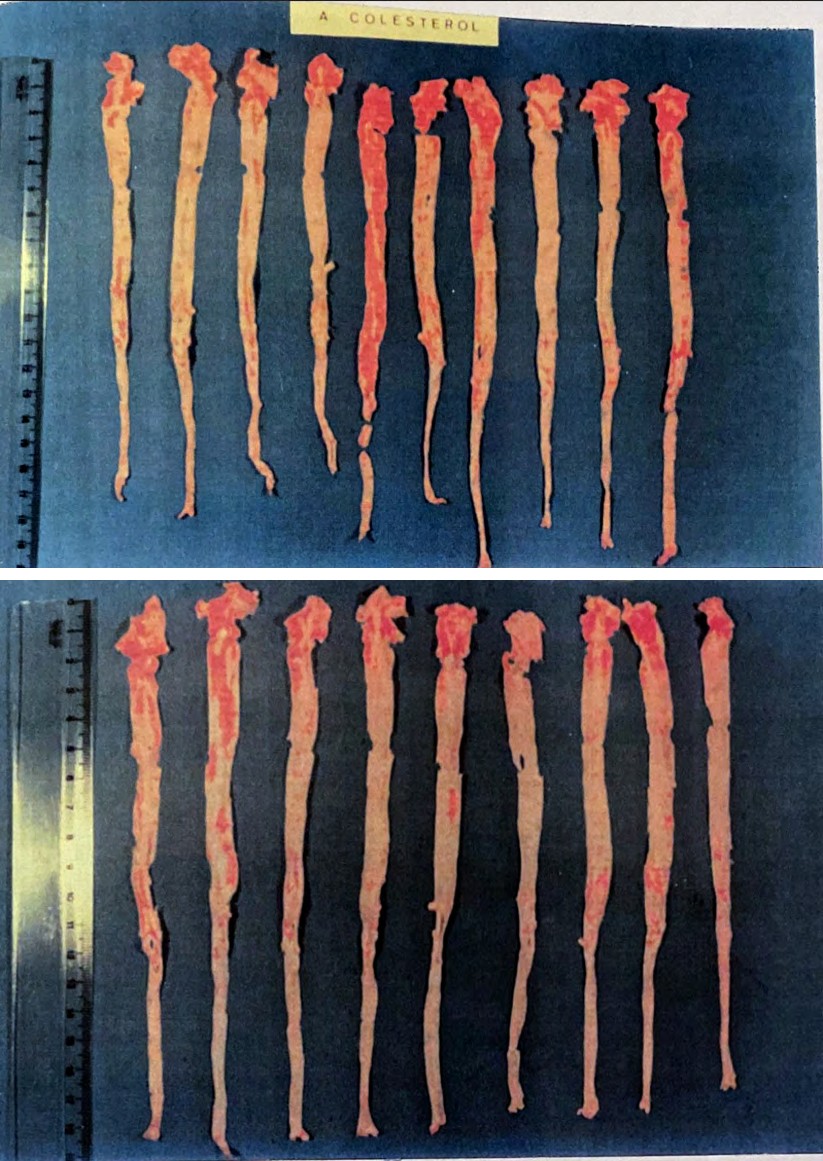
Figure 1A: Macroscopic aspect of aortas of rabbits with Sudam III for visualization of atheroma plaques. Group A (hypercholesterolemic).
Figure 1B: Macroscopic aspect of aortas of rabbits with Sudam III for visualization of atheroma plaques. Group B (cholesterol + simvastatin).
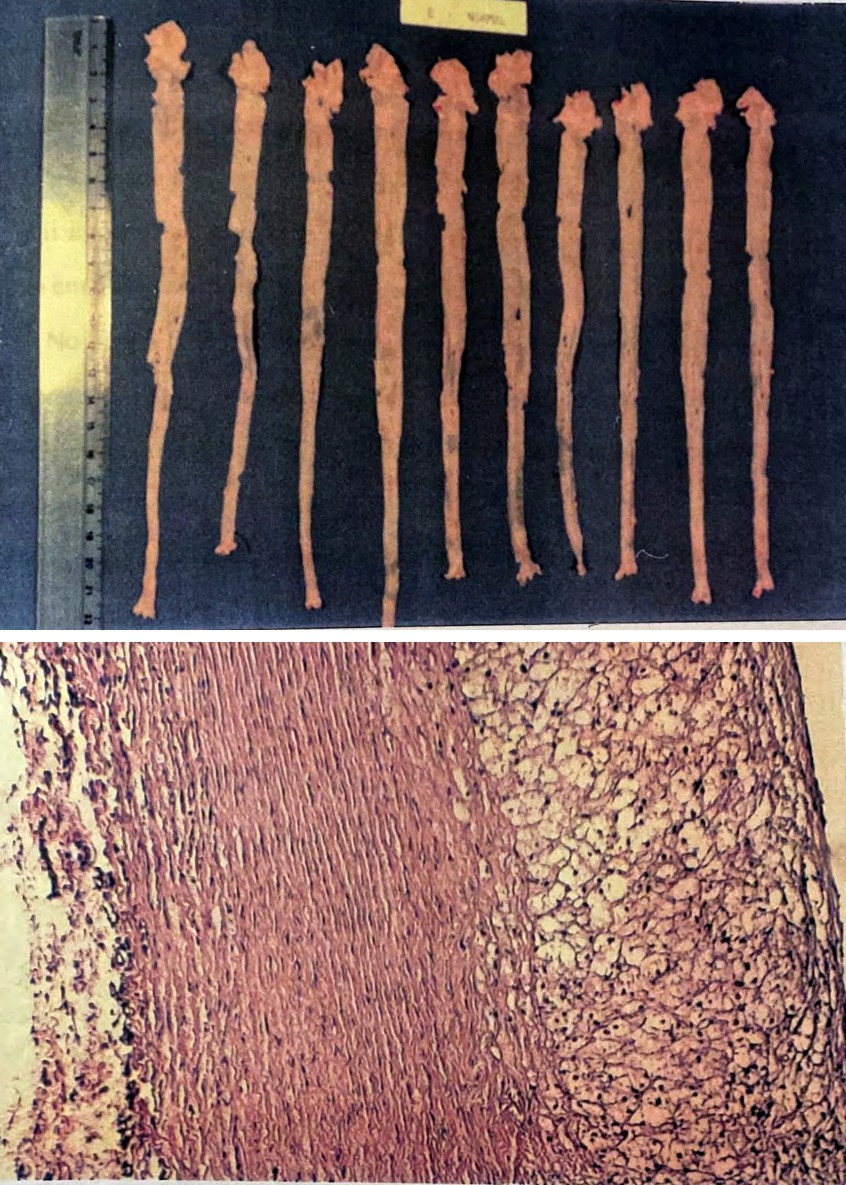
Figure 1C: Macroscopic aspect of normal rabbit aortas. Group C (normal).
Microscopic Evaluation of Aortic Lesions
In the microscopic analysis of the lesions, we observed intense proliferation of foamy cells in the intimate layer of the aorta, with eccentric localization in the circumference of the vessel. In these plates, we observed intense lipid content in macrophages. This aspect was observed in all samples from animals submitted to a hypercholesterolemic diet (Figures 2A-2C).
Figure 2A: Photomicrograph of the aorta with intense thickening of the intima in group A rabbits (hypercholesterolemic diet). HE - 100x.
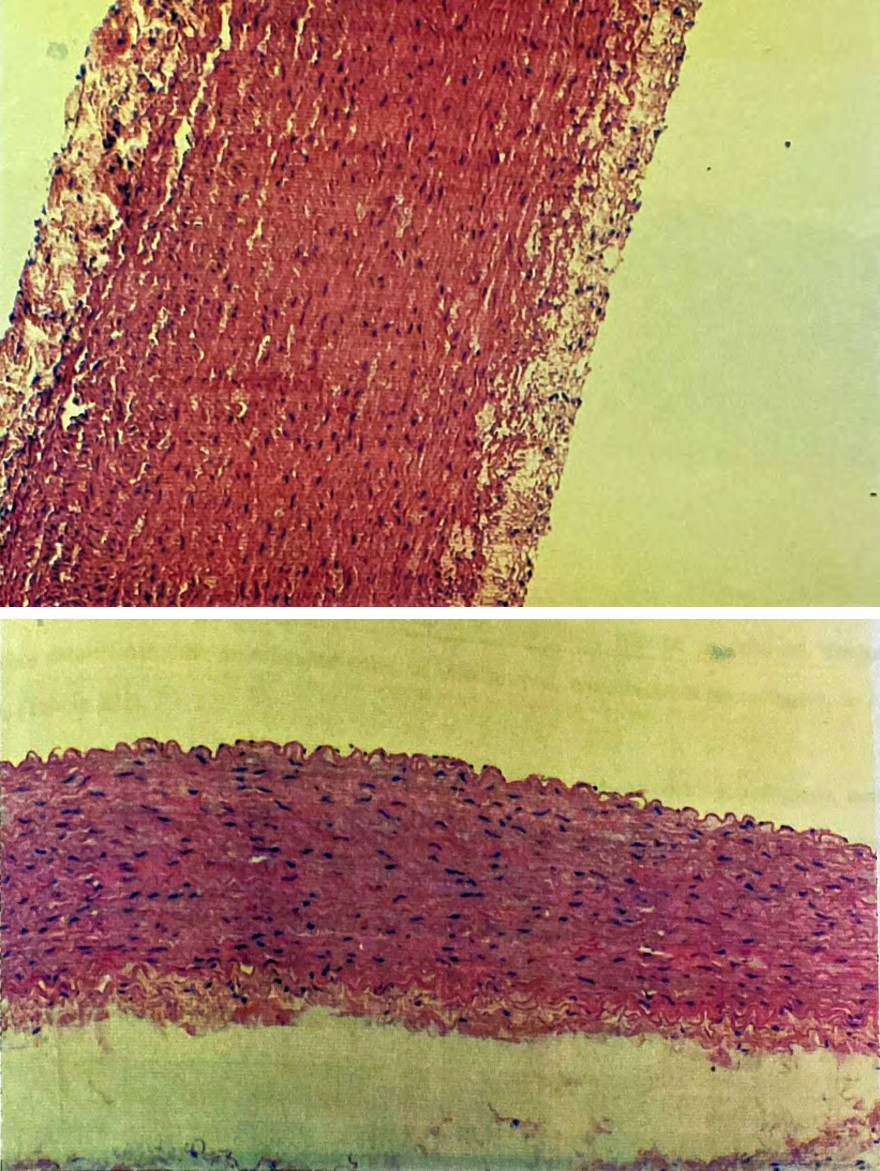
Figure 2B: Photomicrograph of aorta with moderate thickening of the intima in rabbits of Group B. HE - 100x.
Figure 2C: Photomicrography of the aorta without histological alterations in rabbits with normal diet. HE - 100x.
In group A, with a hypercholesterolemic diet and without medication, we noticed a thickening of the tunic intima of the arteries in all cases, with moderate to intense degree in 90% of the cases studied and presence of fibrosis in 20% of the cases. In all those considered an intense degree, the location was in the thoracic aorta. The thickening of the tunic mean was present in 60% of the cases with moderate degree.
In group B, there was a more evident regression of intima thickening, with only 25% presenting moderate degree, all with lipid deposition, 10% with fibrosis and 10% without any thickening of the intima. The middle tunic was thickened by 50%, being only 15% with moderate degree.
In group C (normal diet) moderate thickening of the intima occurred in 10%, but without lipid deposition or fibrosis. The thickening of the tunic media occurred with the same frequency. In this group, 90% showed no impairment.
Evaluation of the Extent and Height of Atheromatous Lesions
Through macroscopic analysis of stained aortas with Sudam III, we evidenced fatty plaques whose compromised area was quantified by computerized planimetry. We found that the group that received normal chow (Group C) did not present any atheromatous lesion, and was therefore excluded from the statistical analysis. In the comparison between the hyperlipidemic groups treated and not treated with simvastatin (A and B), we observed great individual variation, however, not observing a statistically significant difference between the two groups in relation to the percentage of injured area.
When we performed the morphometry of the fatty plate in histological sections, with the aid of a cariometric ocular, we verified plaques with lower height in the group that received the medication simvastatin (group B), both in relation to the thoracic and abdominal aortic plates. In the thoracic region, in addition to the fatty lesions being present in greater numbers, they also had higher height than those of the abdominal region, although in group B the difference between the lesions of the two regions was not statistically significant.
Histopathological Study of the Liver
Through a histological study of the liver, we verified hydropic degeneration in all animals submitted to the hypercholesterolemic diet, being slightly more pronounced in group A. In this group we observed hydropic degeneration with moderate intensity (++) in seven animals (70%); intensity (+) in two animals (20%). In group B, three animals (33%) presented liver alterations with hydropic degeneration with moderate intensity (++), predominantly in this group (55%), alterations graded as mild (+). Hepatic steatosis was observed in three animals in group A and two in group B, with mild intensity. We verified the presence of parenchymal and portal inflammatory infiltrate in some animals of all groups (Figures 3A-3C).
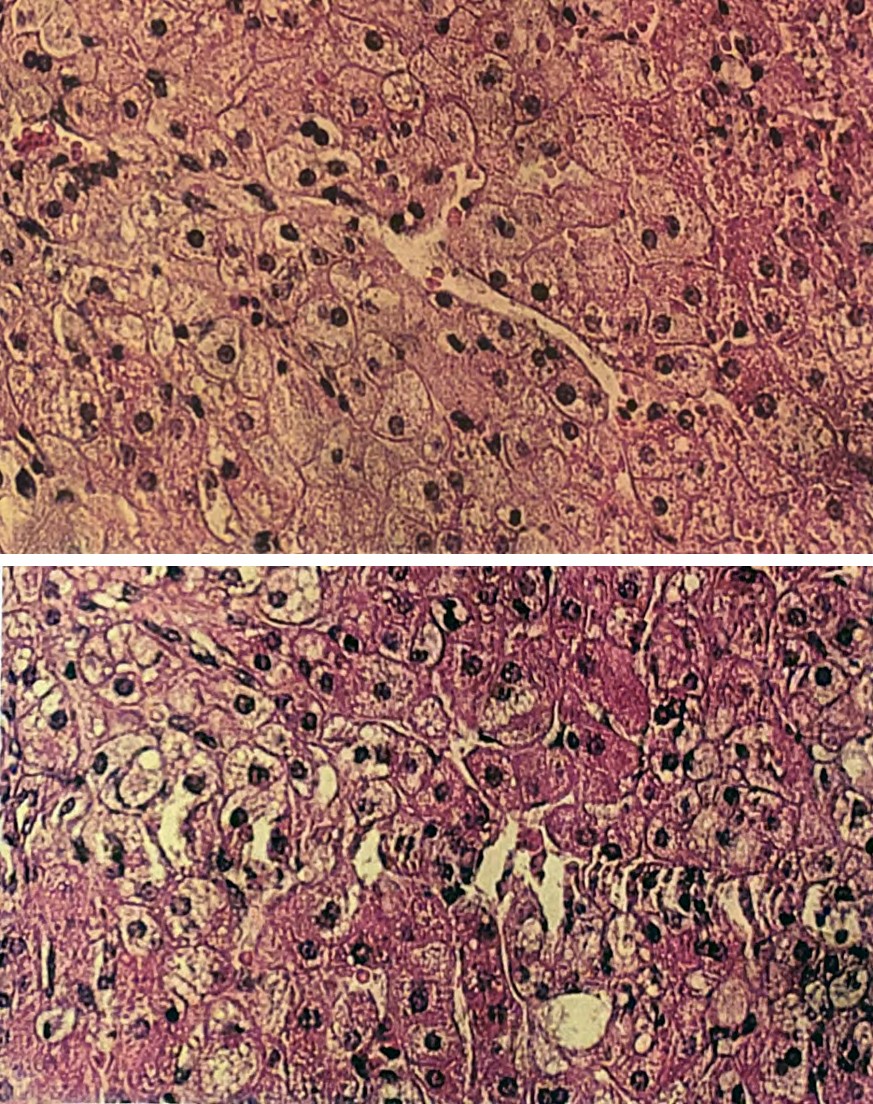
Figure 3A: Photomicrograph of the liver noting ballooned hepatocytes - reticular degeneration - and conserved portal spaces in a rabbit with nine weeks of hypercholesterolemic diet. HE - 250x.
Figure 3B: Photomicrography of the liver with macrogoticular and microgoticular steatosis in rabbit with nine weeks of hypercholesterolemic diet. HE - 250x.
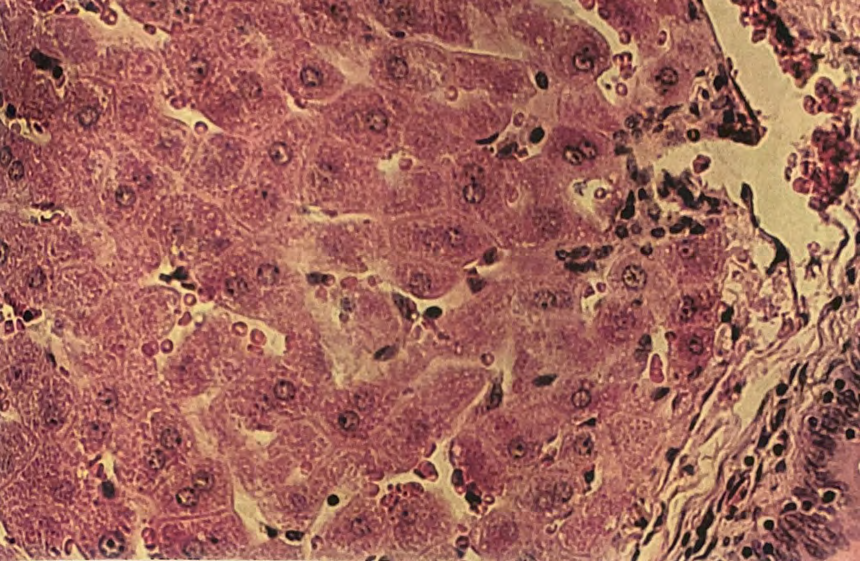
Figure 3C: Photomicrography of the liver without histological changes in rabbit scans with a normal diet. HE - 250x.
Discussion
There are numerous contributions of animal models in atherosclerosis studies. A large number of studies were conducted to better understand the pathogenesis and consequently the therapy of the disease for later application in humans.
The choice of the animal model to be used depends on the variable to be studied, with attention to studies that correlate the type of lesion to be induced and the susceptibility of the animal species.
In our study, we used rabbits fed cholesterol-rich diet as a model for the study of the development of atherosclerosis. Although rabbit is the animal most frequently used in atherosclerosis research, many researchers have criticized the use of this animal, because the lesions result from extremely lipidemic conditions, with topography and the type of lesions different from those found in man. However, the use of different types of diet has induced different types of lesions, some of them closer to human lesions [33].
In the induction of hyperlipidemia, through the hypercholesterolemic diet, different concentrations of cholesterol have been used. In our study, we used the methodology described by Badimon, et al. [15], but using the cholesterol concentration of 1.5%, according to the model developed by Thomaz [34], obtaining significant atherosclerotic lesions after nine weeks of diet. Through this model, we analyzed the effect of simvastatin on the development of atherosclerotic lesion. Simvastatin is a hypercholesterolemic agent, being effective in reducing total cholesterol and LDL levels, inhibiting the action of the enzyme HMG-CoA reductase. With the inhibition of this enzyme, there is a depletion of liver cholesterol, causing a compensatory increase in the number of hepatic LDL-c receptors, concomitant removal of LDL for circulation and decrease of plasma cholesterol.
When in our study we dosed serum cholesterol, we verified similar initial levels of total cholesterol, with no significant difference between the groups (52, 42 and 45 mg/dl, respectively for groups A, B and C). However, after the fifth week, we observed a significant increase in the animals of group A, fed cholesterol, as well as group B, treated with simvastatin (424 and 661 mg/dl). After nine weeks, while in group A the cholesterol level increased significantly (1483 mg/dl), in group B it remained close to that of the fifth week (661 mg/dl) (Table 1). These results are close to those obtained by Badimon, et al. [15], who observed total serum cholesterol around 1559 mg/dl, as well as those obtained by Cotrim [35] of 1342 mg/dl although using a diet with cholesterol at 0.5% and for a period of 90 days. Jorge, et al. [36] reported levels of 1907 mg/dl after eight weeks of hypercholesterolemic diet.
Our study was in agreement with Thomaz [34], who used a diet with 1.5% cholesterol and found cholesterol in the fifth week, 1084 md/dl and in the ninth week 1469 mg/dl. Our results are also compatible with Uint [37] who administered a 1.0% hypercholesterolemic diet for 15 weeks to a group of rabbits, in a comparative study of varied diets, obtaining hypercholesterolemia and subsequent induction of thoracic aortic lesions.
| Group A | Group B | Group C | ||||||
|---|---|---|---|---|---|---|---|---|
| T 0 | T 5 | T 9 | T 0 | T 5 | T 9 | T 0 | T 5 | T 9 |
| 56 | 308 | 1210 | 41 | 581 | 840 | 28 | 18 | 26 |
| 66 | 436 | 1415 | 62 | 704 | 201 | 55 | 28 | 23 |
| 20 | 326 | 1385 | 36 | 506 | 793 | 24 | 15 | 19 |
| 73 | 604 | 1395 | 65 | 794 | 1051 | 27 | 14 | 15 |
| 22 | 724 | 1360 | 43 | 504 | 510 | 48 | 36 | 33 |
| 39 | 451 | 1130 | 32 | 289 | 218 | 67 | 40 | 68 |
| 53 | 328 | 1595 | 35 | 708 | 570 | 21 | 8 | 13 |
| 43 | 260 | 1315 | 31 | 702 | 924 | 37 | 14 | 24 |
| 62 | 372 | 1820 | 33 | 712 | 845 | 33 | 16 | 13 |
| 85 | 428 | 2205 | 71 | 35 | 33 | |||
| 52 | 424 | 1483 | 42 | 611 | 661 | 41 | 22 | 27 |
Table 2: Rabbits with hypercholesterolemic diet (Group A), (diet with cholesterol + simvastatin (Group B) and diet with normal re
(T0 X T5 X T9) X2 critical = 5,99
| Group A | Group B | Group C |
|---|---|---|
| X² calc = 20,00* | X² calc = 14,00* | X² calc = 12,60* |
| T₀ < T₉ | T₀ < T₅′, T₉ | T₀ > T₅′, T₉ |
Table 3: Rabbits with hypercholesterolemic diet (Group A), (diet with cholesterol + simvastatin (Group B) and diet with normal re
| T0 | T5 | T9 | 58 | 101 | 182 | 49 | 45 | 123 | 60 | 61 | 50 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| H calc= 1,82 | H calc = 20,86* | H calc = 24,89* | 72 | 104 | 92 | 66 | 84 | 191 | 51 | 71 | 35 |
| NS | A, B > C | A > B > C | 69 | 97 | 120 | 65 | 74 | 240 | 58 | 46 | 51 |
| 104 | 204 | 148 | 68 | 152 | 69 | 89 | 72 | 41 |
Table 5: Rabbits with hypercholesterolemic diet (Group A), (diet with cholesterol + simvastatin (Group B) and diet with normal re
The use of simvastatin in hypercholesterolemic rabbits, whether induced by diet or genetically hyperlipidemic, has been studied by other authors, whose results are in agreement with some of the parameters analyzed by us. Thus, Fukuo, et al. [30] found a significant reduction in total serum cholesterol, LDL cholesterol and triglycerides, after administering simvastatin at a dose of 10 mg for 24 weeks to genetically hyperlipidemic Watanabe rabbits. A decrease in the installation of lesions in the thoracic and abdominal aorta was observed only in young animals.
Jorge, et al. [36] reported preservation of endothelial function and improvement of the dose-response curve to acetylcholine, both with simvastatin and pravastatin in hypercholesterolemic rabbits. In our study, we used the simvastatin dosage of 10 mg/day/rabbit, corresponding to approximately 3 mg/kg of weight and verified with this dosage a lower serum cholesterol level in the group that received the drug than in the group that received only the hypercholesterolemic diet.
Kobayashi, et al. [27] administering different doses of simvastatin (2.5, 5 and 10 mg/kg/day) for three months to rabbits fed 1% cholesterol, found that the cholesterol level was reduced from 2263 mg/dl to 981 mg/dl, 445 mg/dl, 94 mg/dl, respectively, and aortic involvement with atheromatous lesions was 18.7%, 8.4% and 0%, compared with 43.5% of the untreated group.
In addition to the cholesterol level, we also dose the serum triglyceride level, in which we see a slight increase in the cholesterol-fed groups. After nine weeks, we found a statistically significant increase in the two groups with hyperlipidemic diet (group A = 153 mg/dl, group B = 113 mg/dl and group C = 49 mg/dl) (Table 2). However, this increase may be due to the methodology used in the assays (automated methodological analysis), which is influenced by serum turbidity.
| Group A | Group B | Group C | ||||||
|---|---|---|---|---|---|---|---|---|
| T 0 | T 5 | T 9 | T 0 | T 5 | T 9 | T 0 | T 5 | T 9 |
| 70 | 143 | 71 | 44 | 88 | 85 | 82 | 73 | 58 |
| 58 | 101 | 182 | 49 | 45 | 123 | 60 | 61 | 50 |
| 72 | 104 | 92 | 66 | 84 | 191 | 51 | 71 | 35 |
| 69 | 97 | 120 | 65 | 74 | 240 | 58 | 46 | 51 |
| 104 | 204 | 148 | 68 | 152 | 69 | 89 | 72 | 41 |
| 68 | 150 | 156 | 30 | 43 | 51 | 91 | 76 | 51 |
| 41 | 106 | 198 | 42 | 64 | 86 | 40 | 54 | 41 |
| 44 | 103 | 70 | 30 | 92 | 80 | 91 | 52 | 55 |
| 68 | 88 | 136 | 94 | 116 | 90 | 63 | 77 | 51 |
| 59 | 200 | 357 | 138 | 91 | 57 | |||
| 65 | 130 | 153 | 54 | 84 | 113 | 76 | 67 | 49 |
Table 4: Rabbits with hypercholesterolemic diet (Group A), cholesterol + simvastatin diet (Group B) and diet with normal diet (Gr
(T0 X T5 X T9) X2 critical = 5,99
| Group A | Group B | Group C |
|---|---|---|
| $X^{2 calc = 15,20* | X^{2 calc = 8,22* | X^{2 calc = 7,80* |
| T0 < T5, T9}$ | $T_{0 < T_{5, T9}$ | $T_{0 > T_{9}$ |
| $H calc= 3,14 | H calc= 14,27* | H calc= 18,22* |
| NS | A > B, C | A, B > C |
Table 6: Rabbits with hypercholesterolemic diet (Group A), cholesterol + simvastatin diet (Group B) and diet with normal diet (Gr
Regarding the enzymatic assays of transaminases and GGT, we observed in group B alterations to a lesser degree than the group that received only cholesterol (group A). This variation may have been due to hepatic intracellular metabolism being overloaded by lipid accumulation. The transaminases assays were less altered in the group treated with simvastatin, due to perhaps the lower increase in the level of circulating cholesterol in this group and consequently, lower liver overload. Through the histopathological study, we also observed slightly less marked liver alterations than in the group treated with the drug.
For indirect follow-up of the clinical and nutritional evolution of the animals, we performed hematological measurements: blood count, hematocrit, white blood cell count and platelets. Although variability was observed in hematometric measurements, they do not compromise the subsidiary laboratory information of the follow-up of the clinical evolution of the animals. These assays showed large individual variations, serving, however, as laboratory support to monitor the clinical evolution of the animals. Hemoglobin values were 9.5 g/dl, 11.0 g/dl, 14.0 g/dl, and also groups A and B presented lower hematocrit values at the end than at the beginning of the experiment, but did not reach anemia levels.
Silver, et al. [38] describe the possibility of anemia in rabbits submitted to a hypercholesterolemic diet. The authors report hemolytic anemia and acanthocytosis and hepatic hemosiderosis in rabbits with a high-cholesterol diet for more than a year, mainly in dogs and pigs. We also observed an increase in the number of white blood cells in the three groups and similarity in the number of platelets between the groups.
The most relevant findings relate to the evaluations of aortic lesions, observing lesions in greater number and intensity in the region of the aortic arch of group A animals, being less pronounced in the more distal parts of the artery. In group B, the lesions were moderate with distinctly lower, smoother and sparse plaques.
We added to the microscopic morphometric analyses, where we could observe intense lipid content in macrophages, discriminating the degree of associated fibrosis, according to groups A: B, and C. The regression of thickening of the intima in the treated group, of 146 μm and 83 μm in the thoracic and abdominal aortas, respectively, in relation to 313 μm and 148 μm in the group without medication, confirm the findings of several researchers regarding the protection of the vessel and endothelium in particular. We believe it is appropriate to introduce, at this point, a resumption of the issue from the point of view of the literature in general.
A place of synthesis, the endothelium can be considered the largest paracrino organ of the organism, which responds to various stimuli producing and locally secreting a large number of metabolically active compounds that act in neighboring cells [39]. Among the multiple biological functions of the endothelium, the following stand out [40]:
- Synthesis of connective tissue components such as collagen, elastin, proteoglycans (heparin, heparin- sulfate) and glycoproteins (linin, fibronectin, thrombospondin, factor VIII - von Willebrand complex);
- Production of anticoagulant, fibrinolytic factors (eg, tissue plasminogen activator - tPA) and procoagulants;
- Secretion of mitogenic factors;
- Synthesis of relaxing substances of smooth muscle cells (vasodilators) as a relaxation factor of the endothelium (EDRF), hyperpolarizing factor derived from the endothelium (EDHF) and prostacyclin;
- Synthesis of vasoconstrictor substances, in response to appropriate stimuli: endothelins, endoperoxides,
- Receptor-modulator of vasoactive substances and involved in platelet aggregation and coagulation: acetylcholine, serotonin, thrombin, adenosine nucleotides, arachidonic acid, bradykinin, vasopressin;
- Metabolism and inactivation of catecholamines, serotonin and other platelet products.
- Hypercholesterolemia influences vascular reactivity and endothelium, i.e., in the presence of hypercholesterolemia, the vessel responds to certain stimuli with vasoconstriction instead of vasodilation.
When atherosclerosis regression is induced in experimental animals, the vessel reacts normally again, that is, it produces vasodilation under the action of acetylcholine and platelets. In this process, the integrity of the endothelium is always necessary.
The regression of atherosclerosis, therefore, becomes a process of great importance, especially for two basic aspects: 1. Plaque regression, no matter how small, significantly alters the resistance of the stenosis and favors the restoration of blood flow; 2. The reduction of hypercholesterolemia restores the normal vasodilator capacity of the vessel, provided that the endothelium remains intact.
Atheromatous plaques may assume several morphological characteristics compromising the artery, modifying vasomotor tone or obstructing vessel light. It can occupy an eccentric position located only in an arc of the circumference of the vessel or concentric, involving the entire circumference. As the eccentric plates do not affect the entire circumference of the vessel, with a residual arch with the medial structure intact, it maintains the ability to vary vascular tone. Plaques that are not yet visible angiographically are mainly eccentric, and the frequency of this type of lesion is lower the higher the degree of risk of stenosis. Many patients with unstable angina have at least one stenosis with more than 50% of the vessel diameter. In addition to the location of the plaque in the vessel wall, the severity of stenosis may be dependent on plaque constitution with regard to the relative proportion between lipid content and collagen. In general, lesions of high degree of stenosis (> 70% of the affected diameter) are predominantly collagenous, with lower lipid content and histologically complex, with proliferation of smooth muscle cells [41].
Atherosclerotic lesion is therefore characterized by an accumulation of cells overloaded with esterified cholesterol (foamy cells), underlying the arterial endothelium. Most of these cells are derived from circulating monocytes that turn into resident macrophages, although some are derived from arterial smooth muscle cells that migrate from the media to the intima and undergo transformations.
The morphometry of fatty plaques in histological sections revealed to be the source of the most original data of the present investigation, because the affected area of the aorta and the topography of its lesions did not discriminate the two hypercholesterolemic groups. If we observed, however, for the heights of the lesions and consequently their volumes, they presented significantly lower values in the group that was treated with simvastatin.
By the light of even more recent studies [36], the regression observed in the plate, whether at the area or height level, occurs basically due to the decrease in circulating LDL-c levels. In our case, in which we used simvastatin, this happened in the measurement of height and, consequently, the volume of lesions. We believe we can infer, therefore, that the lipid composition in the plates also decreased, because we worked with young plates, of recent formation, corroborated by the reports of histological analyses.
The influence of simvastatin in the process resulting from its intracellular action of inhibition of cholesterol synthesis was to reduce cholesterol concentration, stimulate the appearance of receptors on the surfaces of cell membranes, or to restore the catabolism function of LDL lipoproteins, with a reduction of cholesterolemic levels of
44.6%. This mechanism was triggered by simvastatin in a condition in which hypercholesterolemia caused by diet had already practically saturated the response of LDL receptors, as explained by Brown & Goldstein [42] in a “mimicry” of the genetic condition of family hypercholesterolemia. Extrapolation to the clinical reasoning of this work done in fibroblast culture, plus that of the animal model used in this investigation obviously deserves caution, however, it is justified by the confrontation with absolutely concordant data in man, obtained in multicenter studies and arteriographic regression studies, such as those reported and compiled by Brown, et al. [43].
Finally, we believe it is worth emphasizing that the improvements evaluated by laboratory analyses and histological measurements, through the use of simvastatin, can revert into other benefits, such as plaque stabilization and endothelial tonic function better restored.
Conclusion
- We found that the group of rabbits treated with hypercholesterolemic diet and simvastatin presented, after nine weeks, a significantly lower cholesterol level than the group not treated with the drug.
- The surface of the aorta compromised with fatty lesions was similar in both hypercholesterolemic groups.
- There was a protective effect by simvastatin, evaluated by the thickness of the atheroma, with a fatty plaque with lower height in the intima layer of the aorta.
- In the liver histological analyses of animals with a hypercholesterolemic diet, we observed intense morphological changes with hydropic degeneration and steatosis, although to a slightly lower degree in the group treated with the drug.
References
-
Ministry of Health. Technical Note No. 325/2013
-
Brown BG, Zhao XQ, Sacco DE, Albers JJ (1993) Lipid lowering and plaque regression. New insights into prevention of plaque disruption and clinical events in coronary disease. Circulation 87(6): 1781-1791.
-
Clarkson TB, Lofland HB (1961) Effects of cholesterol- fat diets on pigeons susceptible and resistant to atherosclerosis. Circ Res 9: 106-109.
-
Clarkson TB, King JS Jr, Lofland HB, Feldner MA, Bullock BC (1973) Pathologic characteristics and composition of diet-aggravated atherosclerotic plaques during “regression”. Exp Mol Pathol 19(3): 267-283.
-
Clarkson TB, Prichard RW, Bullock BC, Clair RW, Lehner ND, et al. (1976) Pathogenesis of atherosclerosis; some advances from using animal models. Exp Mol Pathol 24(3): 264-286.
-
Clarkson TB, Lehner ND, Wagner WD, St Clair RW, Bond MG, et al. (1979) A study of atherosclerosis regression in _Macaca mulatta_. I. Design of experiment and lesion induction. Exp Mol Pathol 30(3): 360-385.
-
Clarkson TB, Bond MG, Bullock BC, Marzetta CA (1981) A study of atherosclerosis regression in Macaca mulatta. IV. Changes in coronary arteries from animals with atherosclerosis induced for 19 months and then regressed for 24 or 48 months at plasma cholesterol concentrations of 300 or 200 mg/dl. Exp Mol Pathol 34(3): 345-368.
-
Clarkson TB, Bond MG, Bullock BC, McLaughlin KJ, Sawyer JK (1984) A study of atherosclerosis regression in Macaca mulatta. V. Changes in abdominal aorta and carotid and coronary arteries from animals with atherosclerosis induced for 38 months and then regressed for 24 or 48 months at plasma cholesterol concentrations of 300 or 200 mg/dl. Exp Mol Pathol 41(1): 96-118.
-
Armstrong ML, Megan MB (1972) Lipid depletion in atheromatous coronary arteries in rhesus monkeys after regression diets. Circ Res 30(6): 675-680.
-
Daoud AS, Jarmolych J, Augustyn JM, Fritz KE, Singh JK, et al. (1976) Regression of advanced atherosclerosis in swine. Arch Pathol Lab Med 100(7): 372-379.
-
Faggiotto A, Ross R (1984) Studies of hypercholesterolemia in the nonhuman primate: II. Fatty streak conversion to fibrous plaque. Arteriosclerosis 4(4): 341-356.
-
Faggiotto A, Ross R, Harker L (1984) Studies of hypercholesterolemia in the nonhuman primate. I. Changes that lead to fatty streak formation. Arteriosclerosis 84(4): 323-340.
-
Small DM, Bond MG, Waugh D, Prack M, Sawyer JK (1984) Physicochemical and histological changes in the arterial wall of nonhuman primates during progression and regression of atherosclerosis. J Clin Invest 73(6): 1590-1605.
-
Armstrong ML, Heistad DD (1990) Animal models of atherosclerosis. Atherosclerosis 85(1): 15-23.
-
Badimon JJ, Badimon L, Fuster V (1990) Regression of atherosclerotic lesions by high density lipoprotein plasma fraction in the cholesterol-fed rabbit. J Clin Invest 85(4): 1234-1241.
-
Wissler RW, Vesselinovitch D (1990) Can atherosclerotic plaques regress? Anatomic and biochemical evidence from nonhuman animal models. Am J Cardiol 65(12): 33-40.
-
Duggan DE, Vickers S (1990) Physiological disposition of HMG-CoA-reductase inhibitors. Drug Metab Rev 22(4): 333-362.
-
Alberts AW (1990) Lovastatin and simvastatin-inhibitors of HMG CoA reductase and cholesterol biosynthesis. Cardiology 77(4): 14-21.
-
Jones PH (1990) Lovastatin and simvastatin prevention studies. Am J Cardiol 66(8): 39-43.
-
Alberts AW, Chen J, Kuron G, Hunt V, Huff J, et al. (1980) Mevinolin: a highly potent competitive inhibitor of hydroxymethylglutaryl-coenzyme A reductase and a cholesterol-lowering agent. Proc Natl Acad Sci USA 77(7): 3957-3961.
-
Illingworth DR, Bacon S (1987) Hypolipidemic effects of HMG-CoA reductase inhibitors in patients with hypercholesterolemia. Am J Cardiol 60(12): 33-42.
-
Illingworth DR (1991) Clinical implications of new drugs for lowering plasma cholesterol concentrations. Drugs 41(2): 151-160.
-
Hoeg JM, Brewer HB Jr (1987) 3-Hydroxy-3- methylglutaryl--coenzyme A reductase inhibitors in the treatment of hypercholesterolemia. JAMA 258(24): 3532-3536.
-
Mauro VF, MacDonald JL (1991) Simvastatin: a review of its pharmacology and clinical use. DICP 25(3): 257-264.
-
Boccuzzi SJ, Bocanegra TS, Walker JF, Shapiro DR, Keegan ME (1991) Long-term safety and efficacy profile of simvastatin. Am J Cardiol 68(11): 1127-1131.
-
Kane JP, Malloy MJ, Ports TA, Phillips NR, Diehl JC, et al. (1990) Regression of coronary atherosclerosis during treatment of familial hypercholesterolemia with combined drug regimens. JAMA 264(23): 3007-2012.
-
Kobayashi M, Ishida F, Takahashi T, Taguchi K, Watanabe K, et al. (1989) Preventive effect of MK-733 (simvastatin), an inhibitor of HMG-CoA reductase, on hypercholesterolemia and atherosclerosis induced by cholesterol feeding in rabbits. Jpn J Pharmacol 49(1): 125-133.
-
Thiery J, Basten A, Sommerburg C, Seidel D (1991) Lovastatin efficacy and tolerance in primary hypercholesterolemia. The German Lovastatin Study Group. Dtsch Med Wochenschr 116(23): 887-894.
-
Thiery J, Teupser D, Walli AK, Ivandic B, Nebendahl K, et al. (1996) Study of causes underlying the low atherosclerotic response to dietary hypercholesterolemia in a selected strain of rabbits. Atherosclerosis 121(1): 63-73.
-
Fukuo Y, Nagashima M, Saitoh A, Kobayashi Y, Terashi A, et al. (1991) Effects of simvastatin on serum lipids and atherosclerosis in WHHL rabbits. Clin Ther 13(3): 417- 424.
-
Siegel S (1975) Stadística no paramétrica. Ed Trillas, México, pp: 346.
-
Hollander M, Wolfe DA (1973) Non parametric statistical methods. John Weley & Sons, New York, pp: 503.
-
Bocan TM, Mueller SB, Uhlendorf PD, Ferguson E, Newton RS (1991) Dietary and mechanically induced rabbit iliac-femoral atherosclerotic lesions: a chemical and morphologic evaluation. Exp Mol Pathol 54(3): 201- 277.
-
Thomaz L (1992) Indução aguda de aterosclerose experimental em coelhos submetidos a dieta hipercolesterolêmica. São Paulo, Brazil [Dissertação (Mestrado). Universidade Federal de São Paulo - Escola Paulista de Medicina].
-
Cotrim FLS (1991) Indução de modelo experimental de aterosclerose em coelhos: estudo bioquímico e anátomo- patológico. São Paulo, Brazil [Dissertação (Mestrado). Universidade Federal de São Paulo - Escola Paulista de Medicina].
-
Jorge PA, Ozaki MR, Metze K (1994) Effects of simvastatin and pravastatin on endothelium-dependent relaxation in hypercholesterolemic rabbits. Exp Toxicol Pathol 46(6): 465-469.
-
Uint L (1992) Metabolism of triglyceride-rich lipid emulsions in the rabbit: effects of triton wr 1339, heparin and potentially atherogenic diets.
-
Silver MM, McMillan GC, Silver MD (1964) Haemolytic anaemia in cholesterol-fed rabbits. Br J Haematol 10(3): 271-280.
-
Healy B (1990) Endothelial cell dysfunction: an emerging endocrinopathy linked to coronary disease. J Am Coll Cardiol 16(2): 357-358.
-
Vrints C, Herman AG (1991) Role of the endothelium in the regulation of coronary artery tone. Acta Cardiol 46(3): 399-418.
-
Davies MJ, Richardson PD, Woolf N, Katz DR, Mann J (1993) Risk of thrombosis in human atherosclerotic plaques: role of extracellular lipid, macrophage, and smooth muscle cell content. Heart 69(5): 377-381.
-
Brown MS, Goldstein JL (1974) Familial hypercholesterolemia: defective binding of lipoproteins to cultured fibroblasts associated with impaired regulation of 3-hydroxy-3-methylglutaryl coenzyme A reductase activity. Proc Natl Acad Sci USA 71(3): 788- 792.
-
Brown G, Albers JJ, Fisher LD, Schaefer SM, Lin JT, et al. (1990) Regression of coronary artery disease as a result of intensive lipid-lowering therapy in men with high levels of apolipoprotein B. N Engl J Med 323(19): 1289- 1298.
- Origin, Evolution, and Functional Impact of Short Insertion- Deletion Variants in Human Genomes: A Review
- Harnessing Molecular Glues for Next-Generation Vaccine, Cancer and Cardiovascular Disease Drug Development: A Comprehensive Review
- Lateral Cervical Epidermal Inclusion Cyst in a Paediatric Patient: A Rare Case Report
- Malarial Plasmodium Falciparum with Hepatitis B and C Virus Infections among Blood Donors in Ife Central Local Government Area, Ile Ife, Osun State, Nigeria
- Withanolides and Withaferin A- What’s next in Ashwagandha Research
- Designing of Dual Pulse Photoacoustic Tomography for Imaging of Drug-Response and Tumor Growth