Vitamin D Status and its Relation to Obesity in Adolescent Schoolgirls in Kolkata- An Epidemiological Pilot Study
Context: Due to lack of adequate sunlight exposure, children and adolescents, particularly girls are at risk of developing Vitamin D deficiency with subsequent health consequences. Obesity, which is increasing in prevalence due to sedentary habits, is also associated with Vitamin D deficiency. However, Indian data on Vitamin D status of adolescent girls with reference to obesity is lacking. Objective: To study the prevalence of Vitamin D deficiency and to find its association with body composition and obesity parameters in adolescent schoolgirls in Kolkata. Methods: Cross-sectional, observational, single centre study. 160 adolescent schoolgirls (10-18 years) with no known illness were assessed for weight, height, body mass index (BMI), waist hip ratio (WHR), visceral fat content (VFC) and serum 25(OH) D level Results: Mean serum 25(OH) D level was 18.7±12.1 ng/ml. 77% were Vitamin D deficient (<20ng/ml) and 13% had vitamin D insufficiency (21-29 ng/ml). In Spearman’s coefficient test BMI was positively correlated with serum 25(OH) D level (r=0.165, p=0.037), negatively correlated with WHR (r=-0.329, p=0.0008) but no significant correlation was found with VFC (r=-0.055, p=0.491). Linear regression analysis also revealed significant negative correlation of serum 25(OH) D with WHR (coefficient -48.902, p=0.0002, 95%CI -73.977±-23.827). Receiver operating characteristic ROC) curve analysis showed WHR cut off 0.92 having 78.9% accuracy in predicting serum 25(OH) D level of 20 ng/ml, with 75.6% sensitivity and 32.8% specificity. Conclusion: Vitamin D deficiency is highly prevalent in adolescent schoolgirls in Kolkata. In this group, obesity is inversely correlated with Vitamin D status with waist hip ratio being a strong negative predictor of Vitamin D status.
Introduction
Vitamin D is a steroid hormone, essential for calcium and bone mineral metabolism. The primary site of Vitamin D synthesis is the epidermis, where 7-dehydrocholesterol is converted to cholecalciferol by ultraviolet B rays. In the liver, cholecalciferol is metabolized into 25-hydroxyvitamin D from which metabolically active 1.25 dihydroxyvitamin D is subsequently synthesized in the kidneys. Food is a poor source of Vitamin D, except for selected sources, such as oily fish, egg yolk and shiitake mushrooms [1]. Due to sedentary lifestyle and lack of sunlight exposure, children and adolescents, particularly girls, are at risk for having Vitamin D deficiency. In this population, low levels of Vitamin D may impair growth and development and have a deleterious effect on bone health [2] Figure 1.
A study by Marwaha RK, et al. showed very high prevalence of hypovitaminosis D of about 90% in healthy schoolchildren in northern India and girls to be worse affected than boys [3]. Subsequent studies from Kangra and Kullu districts of Himachal Pradesh and Eastern India (Kolkata) also revealed 80% and 86% of adolescent school children respectively to have Vitamin D deficiency [4, 5]. Recent data of Vitamin D status in Indian children from semirural areas documented 71% prevalence of Vitamin D insufficiency in spite of high percentage (80%) of reported sunlight exposure of at least 2 hours or more [6] (Figure 2).
Obesity is known to be associated with decreased Vitamin D status [7, 8]. Vitamin D, being fat-soluble, is readily stored in adipose tissue, and thus, it could be sequestered in the larger body pool of fat of obese individuals resulting is reduced bioavailability and lower serum 25(OH)D concentrations. Another hypothesis suggests that obese people due to the sedentary lifestyle and less physical activity have less sun exposure and Vitamin D deficiency [10] (Figure 3).
High levels of leptin, IL-6 and hepatic steatosis in obesity may also may affect synthesis of Vitamin D [11, 12]. Studies have demonstrated that 1% increase in fat weight is associated with a 1.15 ± 0.55 nmol/L reduction in serum calcifediol [13]. On the other hand, literature suggest role of Vitamin D in insulin synthesis and tissue sensitivity to insulin due to various mechanisms [14]. Vitamin D stimulates expression of insulin sensitivity genes, interacts with Vitamin D receptors and insufficiency leads to secondary hyperparathyroidism, enhanced lipogenesis, reduce insulin sensitivity and increase fat mass [15]. Children with suboptimal Vitamin D level have been shown to have three to four fold greater risk of insulin resistance [16]. Although studies looking at Vitamin D levels in Indian adolescents found high prevalence of vitamin D deficiency (94.7%) in obese children [17], data regarding their association with obesity and body composition is lacking in this population. To fill this knowledge gap, this study has been designed to look at the prevalence of Vitamin D deficiency and to find its association with body composition and obesity parameters in adolescent schoolgirls.
Materials and Methods
Settings and study design
This cross-sectional, observational, single centre study was done in a private Christian Missionary school in Kolkata and Department of Endocrinology, Nilratan Sircar Medical College and Hospital, Kolkata. The institutional ethics committee approved the study and written informed consent of guardian was taken according to proforma. The study was financially supported by a research grant provided by Endocrine Society of Bengal.
Inclusion and Exclusion Criteria
Adolescent schoolgirls (10-18 years) with no known illness and attending heath awareness camps in the school campus were included. Students with any known illness and history of drug intake in preceding 6 months were excluded.
Study Method
At the scheduled visit, a detailed questionnaire documenting demographic information, relevant medical and treatment history was filled. Weight was measured with a portable weighing scale and height was measured with a portable stadiometer with the measurement corrected to the nearest 1 mm. The body mass index (BMI) was calculated from measurements of height and weight as per formula (BMI=weight in kg/height in meters square). Waist and hip circumference were measured using stretch resistant tape. Waist hip ratio (WHR) was calculated. Body fat was estimated using Bioelectrical Impedance method with a Tanita DC-13C Total Body Composition Analyzer. Serum 25(OH) D was measured by chemiluminescence method in Beckman Coulter Access 2 Immunoassay System which has a total imprecision ≤10.0% CV at concentrations >15.0 ng/mL (37.5 nmol/L), and Standard Deviation(SD) ≤1.5 ng/mL (3.8 nmol/L) at concentrations ≤15.0 ng/mL. Relevant precautions and standards in sample collection, transportation were maintained.
Vitamin D deficiency was defined by 25(OH) D level below 20 ng/ml and insufficiency as 21-29 ng/ml according to Endocrine Society clinical practice guideline [18].
Sample Size
A total of one hundred and sixty (160) adolescent schoolgirls were included in our study. Sample size was based on the vitamin D status of adolescent schoolchildren in a previous study from Kolkata which showed 86% prevalence of Vitamin D deficiency. Assuming a similar vitamin D status among the participants of the present study, a total of 101 participants were required to estimate prevalence of vitamin D deficiency with an assumed sensitivity and specificity of 90% with 90% power in a two‐sided 95% confidence interval.
Statistical Analysis
Statistical analysis was carried out using SPSS statistical software (version 19.0). Data are presented as number (%), mean ± SD. For variables on categorical scale, chi-square test or Fischer exact test was used to find association between the study variables. Pearson or Spearman correlation test was used to find correlation between the study variables on continuous scale. A p-value less than 0.05 was considered as statistically significant.
Results
The participants (n=160) had mean (±SD) age of 13.8 (±1.8) years, with BMI 22.4 kg/m2 (±4.7). The waist hip ratio and visceral fat content were 0.89 (±0.07) and 34.64% (±13.95) respectively (Table 1).
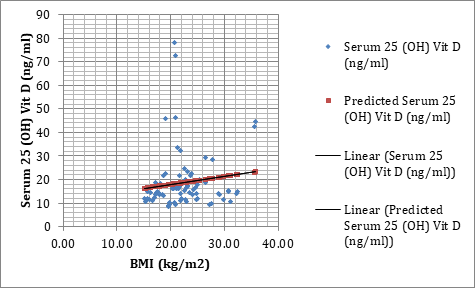
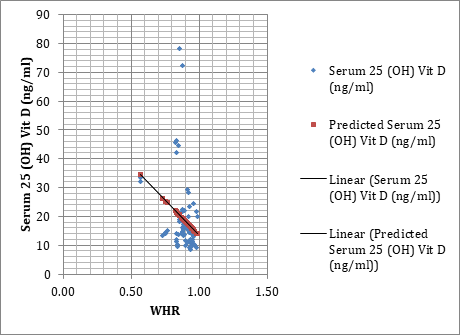
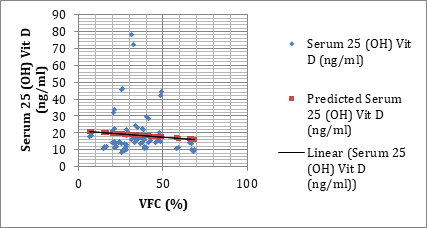
Mean serum 25(OH) D level was 18.7±12.1 ng/ml with 77% adolescent schoolgirls being Vitamin D deficient and 13% having Vitamin D insufficiency. Only one in ten children had sufficient Vitamin D. In Spearman’s coefficient test, BMI was positively correlated with serum 25(OH) D level (r=0.165, p=0.037) but no significant correlation was found with VFC (r=-0.055, p=0.491). Serum 25(OH) D was negatively correlated with WHR which was statistically significant (r=-0.329, p=0.0008) (Table 2).
| Mean±SD | |
|---|---|
| Age (yrs) | 13.83±1.84 |
| Weight (kg) | 52.86±12.27 |
| Height (cm) | 153.26±5.94 |
| BMI (kg/m2) | 22.44±4.65 |
| WC (cm) | 80.60±10.74 |
| HC (cm) | 90.67±10.26 |
| WHR | 0.89±0.07 |
| VFC (%) | 34.64±13.95 |
| Serum 25 (OH) Vit D (ng/ml) | 18.72±12.17 |
Table 1: Baseline characteristics of study population.
| Correlation Coefficient (r) | p-value | Remark | |
|---|---|---|---|
| Age (yrs) | 0.46 | <0.00000 | Positive Significant correlation |
| Weight (kg) | 0.262 | 0.00081 | Positive Significant correlation |
| Height (cm) | 0.258 | 0.00098 | Positive Significant correlation |
| BMI (kg/m2) | 0.165 | 0.03663 | Positive Significant correlation |
| WC (cm) | 0.043 | 0.59214 | No Significant correlation |
| HC (cm) | 0.227 | 0.00397 | Positive Significant correlation |
| WHR | -0.329 | 0.00082 | Negative Significant correlation |
| VFC (%) | -0.055 | 0.49109 | No Significant correlation |
Table 2: Spearman’s coefficient (test): Correlation of 25(OH) D levels with different parameters.
We performed linear regression analysis which revealed significant negative correlation of serum 25(OH) D with WHR (coefficient -48.902, p=0.0002, 95%CI -73.977±-23.827) (Table 3).
| Coefficients | Standard Error | P-value | 95% CI | |
|---|---|---|---|---|
| Age (yrs) | 2.031 | 0.5 | <0.0000 | 1.043±3.020 |
| Weight (kg) | 0.151 | 0.078 | 0.0554 | -0.0036±0.305 |
| Height (cm) | 0.173 | 0.162 | 0.2877 | -0.148±0.494 |
| BMI (kg/m2) | 0.333 | 0.207 | 0.1088 | -0.075±0.741 |
| WC (cm) | -0.137 | 0.089 | 0.129 | -0.313±0.040 |
| HC (cm) | 0.093 | 0.094 | 0.3244 | -0.093±0.279 |
| WHR | -48.902 | 12.695 | 0.0002 | -73.977±-23.827 |
| VFC (%) | -0.072 | 0.069 | 0.2983 | -0.209±0.064 |
Table 3: Linear Regression Analysis: Serum 25(OH) D v/s different parameters.
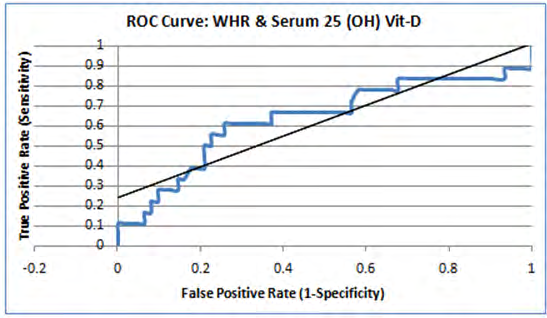
In ROC curve analysis, WHR cut off 0.92 showed 78.9% accuracy in predicting serum 25(OH) D level of 20 ng/ml, with 75.6% sensitivity and 32.8% specificity (Figure 4).
Discussion
In our study in a private Christian Missionary school in Kolkata, 90% of the adolescent school children had serum 25(OH) D level below normal range (<30 ng/ml). This high prevalence of hypovitaminosis D was similar to existing Indian data of Vitamin D deficiency in the same age group [3, 4, 5, 6, 17]. Importantly, all the children were from good socioeconomic background with adequate nutrient status. This suggest that sedentary lifestyle, poor sun exposure and other factors also play a major role in maintenance of normal Vitamin D status apart from nutrition. The association of obesity with Vitamin D deficiency is reported in literature and a possible mechanistic explanation is the sequestration of 25(OH) D in adipose tissue. In the present study, we did not find any significant correlation between serum 25(OH) D level and BMI or VFC, but there was significant negative correlation with WHR. Literature suggests WHR as better indicator than BMI, as obesity parameter for prediction of metabolic syndrome and future cardiac risk in adults [19].
So, the negative correlation of Vitamin D and WHR as obesity parameter is clinically relevant in view of high prevalence of both hypovitaminosis D and obesity in adolescent growing children, emerging due to the convergence of two epidemics as a result of adoption of a sedentary lifestyle by modern societies. Nutritious diet, adequate exercise, outdoor activity and acquiring a healthy lifestyle is the key to prevent both these emerging health problem in growing children in our country.
To the best of our knowledge, this was the first study in Indian adolescent school children which looked at the association of Vitamin D deficiency with different obesity parameters. The limitations of our study include gender bias as only girls were included and representation from only good socioeconomic background. Also, being an epidemiological cross sectional study, no cause effect relationship could be established.
Conclusion
Vitamin D deficiency is highly prevalent in adolescent schoolgirls in Kolkata. Obesity is inversely correlated with Vitamin D status with WHR has strong negative correlation among obesity parameters. WHR cut off 0.92 has reasonable diagnostic accuracy and sensitivity in predicting possible hypovitaminosis D in this adolescent age group.
References
-
Holick MF (2005) The vitamin D epidemic and its health consequences. J Nutr 135(11): 2739S‐2748S.
-
Bueno AL, Czepielewski MA (2008) A importância do consumo dietético de cálcio e vitamina D no crescimento. J Pediatr (Rio J) 84(5): 386-394.
-
Marwaha RK, Tandon N, Reddy D, Reddy HK, Aggarwal R, et al. (2005) Vitamin D and bone mineraldensity status of healthy schoolchildren in northern India. Am J Clin Nutr 82(2): 477-482.
-
Kapil U, Pandey RM, Goswami R, Sharma B, Sharma N, et al. (2017) Prevalence of Vitamin D deficiency and associated risk factors among children residing at high altitude in Shimla district, Himachal Pradesh, India. Indian J Endocrinol Metab 21(1): 178-183.
-
Basu S, Gupta R, Mitra M, Ghosh A (2015) Prevalence of vitamin d deficiency in a pediatric hospital of eastern India. Indian J Clin Biochem 30(2): 167‐173.
-
Mandlik R, Kajale N, Ekbote V, Patwardhan V, Khadilkar V, et al. (2018) Determinants of Vitamin D status in Indian school-children. Indian J Endocr Metab 22(2): 244-248.
-
Gordon CM, DePeter KC, Feldman HA, Grace E, Emans SJ (2004) Prevalence of vitamin D deficiency among healthy adolescents. Arch Pediatr Adolesc Med 158(6): 531-537.
-
Rockell JE, Green TJ, Skeaff CM, Whiting SJ, Taylor RW, et al. (2005) Season and ethnicity are determinants of serum 25-hydroxyvitamin D concentrations in New Zealand children aged 5-14 y. J Nutr 135(11): 2602- 2608.
-
Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF (2003) Decreased bioavailability of vitamin D in obesity. Am J Clin Nutr May 77(5): 1342.
-
Florez H, Martinez R, Chacra W, Strickman-Stein N, Levis S (2007) Outdoor exercise reduces the risk of hypovitaminosis D in the obese. J Steroid Biochem Mol Biol 103(3-5): 679-681.
-
Targher G, Bertolini L, Scala L, Cigolini M, Zenari L, et al. (2007) Associations between serum 25-hydroxyvitamin D3 concentrations and liver histology in patients with non-alcoholic fatty liver disease. Nutr Metab Cardiovasc Dis 17(7): 517-524.
-
Drincic AT, Armas LA, VanDiest EE, Heaney RP (2012) Volumetric dilution, rather than sequestration best explains the low vitamin D status of obesity. Obesity 20(7): 1444-1448.
-
Lenders CM, Feldman HA, Von Scheven E, Merewood A, Sweeney C, et al. (2009) Relation of body fat indexes to vitamin D status and deficiency among obese adolescents. Am J Clin Nutr 90(3): 459-467.
-
Seida JC, Mitri J, Colmers IN, Majumdar SR, Davidson MB et al. (2014) Clinical review: Effect of vitamin D3 supplementation on improving glucose homeostasis and preventing diabetes: A systematic review and meta- analysis. J Clin Endocrinol Metab 99(10): 3551-3560.
-
Kong J, Li YC (2006) Molecular mechanism of 1,25-dihydroxyvitamin D3 inhibition of adipogenesis in 3T3-L1 cells. Am J Physiol Endocrinol Metab 290(5): 916-924.
-
Cediel G, Corvalán C, Aguirre C, de Romaña DL, Uauy R (2016) Serum 25-Hydroxyvitamin D associated with indicators of body fat and insulin resistance in prepubertal chilean children. Int J Obes (Lond) 40(1): 147‐152.
-
Varshney S, Khadgawat R, Gahlot M, Khandelwal D, Oberoi AK, et al. (2019) Effect of high-dose Vitamin D supplementation on beta cell function in obese Asian- Indian children and adolescents: A randomized, double blind, active controlled study. Indian J Endocr Metab 23(5): 545-551.
-
Holick MF, Binkley NC, Bischoff Ferrari HA, Gordon CM, Murad MH, et al. (2011) Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 96(7): 1911‐1930.
-
Noble RE (2001) Waist-to-hip ratio versus BMI as predictors of cardiac risk in obese adult women. West J Med 174(4): 240‐241.
- Origin, Evolution, and Functional Impact of Short Insertion- Deletion Variants in Human Genomes: A Review
- Harnessing Molecular Glues for Next-Generation Vaccine, Cancer and Cardiovascular Disease Drug Development: A Comprehensive Review
- Lateral Cervical Epidermal Inclusion Cyst in a Paediatric Patient: A Rare Case Report
- Malarial Plasmodium Falciparum with Hepatitis B and C Virus Infections among Blood Donors in Ife Central Local Government Area, Ile Ife, Osun State, Nigeria
- Withanolides and Withaferin A- What’s next in Ashwagandha Research
- Designing of Dual Pulse Photoacoustic Tomography for Imaging of Drug-Response and Tumor Growth