Inhalation of Helium-Oxygen Mixture in Two Cases of Maternal Respiratory Distress during Labor and Delivery
Inhaled mixtures of helium-oxygen have been rarely used in spontaneously ventilating patients presenting with airway obstruction during labor and delivery. We present two patients, each suffering from severe tracheal narrowing due to extra-tracheal compression by goiter and each presenting with respiratory distress during the second stage of the labor. Inhaled helium/oxygen was administered to relieve respiratory distress; routine labor and assisted vaginal delivery ensued without further maternal or neonatal complication. We review the rationale for the use of inhaled helium/oxygen in such patients. We also review the anesthetic plan for unexpected abdominal delivery, including airway management for general anesthesia.
Introduction
Inhalation of helium/oxygen has been life-saving in patients afflicted respiratory distress secondary to a narrow airway [1]; it was first reported in the obstetric literature thirty years ago [2]. We could find no recent reports of helium/oxygen inhalation therapy in a parturient with upper airway obstruction. We report two parturients, each with severe tracheal stenos is (goiter), presenting with onset of significant respiratory distress. Inhaled helium/oxygen alleviated maternal distress. Maintenance of effective epidural analgesia during a passive second stage led to assisted vaginal delivery of a healthy neonate.
Presentation of Cases
Case 1
At 392/7 weeks’ gestational age, a 28-year-old primigravida presented for induction of labor (IOL) with a diagnosis of fetal growth restriction. An anesthesiologist performed a routine evaluation. Recently emigrated, available medical/prenatal records did not document any previous evaluation of her large goiter. She complained of episodic shortness of breath with anxiety but denied:
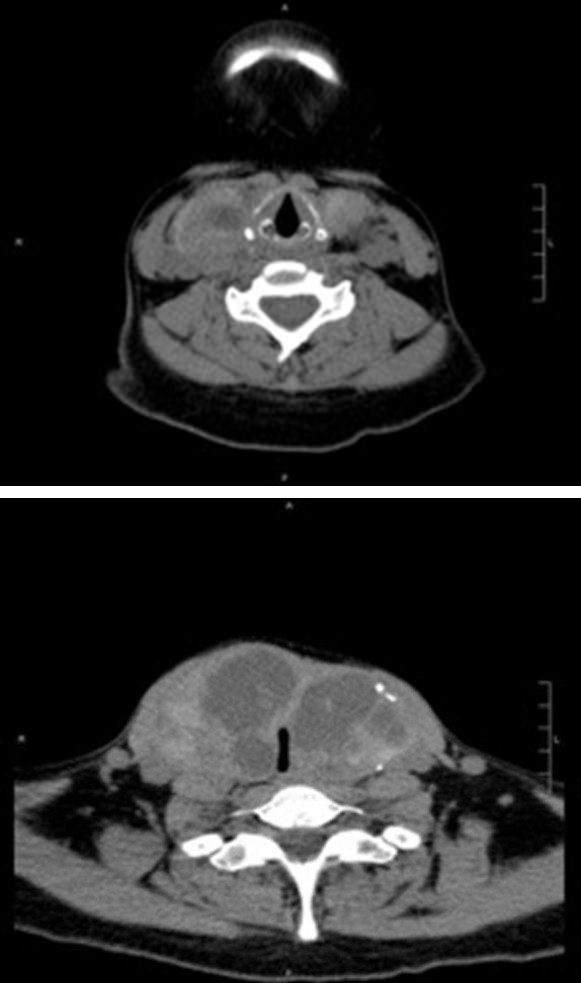
stridor; other respiratory complaints; difficulty in swallowing; symptoms of obstructive sleep apnea; or, orthopnea. She measured BMI= 23.5 kg/m2. Physical exam was notable for a large bilateral-extending, multinodular goiter. She demonstrated: mild limitation to neck extension/flexion/rotation; full mouth opening; intact dentition; partial view of her uvula (wide-mouth opening); and, could not bite her upper lip. Cricoid, (any) tracheal, and thyroid cartilage were non-palpable. Auscultation revealed bilateral, equal air entry; no wheezing or stridor. Computed tomography (CT) demonstrated multinodular goiter (Figure1) compressing a 3.4 cm cranio-caudal length of upper cervical trachea; narrowest measurements were 3.4 mm (transverse) and 17 mm (antero-posterior) (Figure 1). Normal thyroid function was confirmed. An ENT surgeon-performed flexible fiber-optic laryngoscopy was deemed “unremarkable;” though thyroidectomy was offered, planned either separate from or concomitant with abdominal delivery. The patient deferred surgery due to multiple social issues. Patient/obstetricians were counseled of a potential problem in airway management, either as part of general anesthesia (i.e., immediate abdominal delivery) or for resuscitation (e.g., after cardio respiratory collapse). We suggested “early” induction of neuraxial analgesia to:“determine a working catheter;” decrease any need for routinely obstetrician- administered parenteral opioid analgesia’; and mitigate against induction of general anesthesia due to failed neuraxial surgical anesthesia. We conjectured that second-stage expulsive efforts (might lead to respiratory decompensation. Within hours, she reported rupture of membranes with regular contractions. Auscultation (lungs) was unchanged. Per routine, combined spinal- epidural (CSE) analgesia was induced and maintained; infusion of dilute local anesthetic/opioid solution to provided satisfactory analgesia. Three hours later, the patient (in second stage)was encouraged by her attendants to perform Valsalva-assisted expulsive efforts. Respiratory distress developed, including both peripheral oxygen desaturation (SpO2 = 85-89%) and stridor, was unresponsive to inhaling supplemental high-flow oxygen. The patient then inhaled a mixture (70%/30%) of helium- oxygen. Respiratory rate, work of breathing and anxiety all decreased;SpO2 increased (> 97%). and stridor resolved. Expulsive efforts were discontinued. Twenty- five minutes later, she underwent vacuum-assisted vaginal delivery without maternal or neonatal complications. The patient and her husband were advised to immediate follow up with ENT surgeon. An appointment was offered but declined. She was lost to follow up.
1A
1B Figure 1A and 1B: CT Neck: 1A Glottis. 1B pronounced mass effect on the upper cervical trachea which at its narrowest point measures 3.4 mm x transverse 17 mm AP. The narrowing is seen over a 3.4 cm craniocaudal distance.
Case 2
At 34 weeks’ estimated gestational age, a 29 year-old multipara (routine vaginal deliveries) presented for consultation due to goiter. The goiter had doubled in size during pregnancy. She reported shortness of breath while supine or walking. Airway exam revealed large goiter and inability to palpate cricoid,(any) tracheal or thyroid cartilage. CT demonstrated a large goiter with retrosternal extension; trachea measured 9mmx 7mm (narrowest) and deviated to the right (Figure 2). Normal thyroid function was confirmed. An ENT surgeon performed a flexible fiber-optic laryngoscopy deemed “unremarkable.” Multi-disciplinary discussion planned an IOL before 39 weeks’ gestation due to the growing size of the mass and previous poor clinic attendance. On
admission, auscultation (lungs) was unremarkable. Per routine protocol, CSE analgesia was induced and maintained; infusion of dilute local anesthetic/opioid solution provided satisfactory labor analgesia for 8 hours. During planned “passive” second stage and descent of the fetal head onto the perineum, the patient appeared tachypneic, complaining of being short of breath, though SpO2remained unchanged. Now inhaling a (70%/30%) mixture of helium/oxygen she reported her breathing “improved” and tachypnea abated. Auscultation before and after inhalation of the helium/oxygen revealed clear (no wheezing/stridor) breath sounds. Encouraged to perform three “open-glottis”expulsive efforts the fetal head descended; she underwent forceps-assisted-vaginal delivery without maternal or neonatal complications. Fifteen minutes later, without respiratory difficulty, the inhaled helium/oxygen mixture was discontinued.

2A
2B Figure 2A and 2B: CT Neck: 2A Glottis. 2B mass effect on the trachea and esophagus to the right with moderate narrowing measuring 9x7 mm at the narrowest segment at C6-C7 level.
Discussion
Any further decrease in upper airway radius increases turbulence, impedance and work of breathing (i.e., to create negative intrathoracic pressure).The inhalation of helium (65-70%)/oxygen (30-35%) as a therapeutic gas improves respiratory mechanics, amelioratingdyspnea in patients with upper airway obstructive lesions [3]. Substituting helium in a mixture with oxygen decreases overall density of inhaled gas, decreasing the effort to create negative pressure. Our patients demonstrated severe airway compression. Though an established therapy in previously reported cases of partial upper airway obstruction, [1] inhalation of a mixture of helium/oxygen has rarely been reported in labor. In both cases presented, inhalation of a helium-oxygen (70%/30%, respectively) ameliorated respiratory distress presenting during second stage of labor. In second stage of labor, there are increased maternal oxygen requirements and hyperventilation due to: increased vaginal discomfort; voluntary/involuntary Valsalva-associated expulsive efforts; and, progressive metabolic academia [4]. Hyperventilation worsens turbulent flow of air and the sense of dyspnea [3]. Hypothesizing that Valsalva-associated expulsive effort in patients with extra-thoracic tracheal compression would make gas flow more turbulent, abeyance of expulsive efforts and initiation of inhaled of helium/oxygen mitigated maternal respiratory decompensation and improved maternal oxygenation. In hopes of mitigating any relationship between obstetric pain and increased work of breathing, neuraxial analgesia was induced “early” in labor. If this option had been rejected, then other forms of analgesia were considered. We believed that intravenous opioid analgesia (nurse-administered or even patient-controlled intravenous analgesia using fentanyl or remifentanil) might produce opioid-induced respiratory depression. Other forms of labor analgesia were considered. Over 60 years ago, Robert Hingson [5] described inhalation of helium/oxygen/cyclopropane to produce obstetric analgesia. Today, the use of inhaled nitrous oxide/oxygen (50%/50%) is accepted by some clinicians as an effective analgesic in labor [6]. The inhalant that we utilized contained 70% helium/ 30% oxygen. The respiratory therapists assigned to our Unit believed that initiating inhalation using a tank containing a fixed ratio of helium/oxygen was simpler than varying (blending) other ratios.If needed, higher concentrations of oxygen can be blended by respiratory therapists [7].
However, blending an inhalant with 50% nitrous oxide/30% helium would have precluded the use of increased inspired oxygen concentrations. In these two cases, the mixture was not varied. We did not analyze inspired and expired gas in these cases to verify the labeled mixture. The use of par cervical block and pudendal nerve block have been well reported to provide satisfactory analgesia for first and second stages of labor, respectively; their efficacy and side effects are well-reported [8]. Bilateral parasympathetic blocks have been reported to provide satisfactory analgesia [9]. Even intravenous infusion of dexmedetomidine was considered as a drug that would not further exacerbate any maternal respiratory decompensation [10]. The infusion of supplemental low- dose ketamine labor analgesia [11] was rejected due to the possibly increased airway secretions. If anesthesia for abdominal delivery was indicated (e.g., cephalopelvic disproportion or acute fetal decompensation),then we planned to inject the in situ neuraxialcatheter. Demonstrating satisfactory regional analgesia/anesthesia “early” in labor was therefore reassuring. If neuraxial anesthesia was deemed ineffective before surgery, we believed risk of airway management outweighed the benefit of a shorter decision-to-delivery time; CSE or single-injection spinal anesthesia would have been induced. If neuraxial anesthesia was deemed ineffective during surgery, then we first planned on infiltration with local anesthetic [12] supplemented by intravenous infusion of dexmedetomidine. Injection of intravenous ketamine was considered [13] but rejected due to the risk of increased airway secretions. If tracheal intubation was indicated (i.e., general anesthesia or part of maternal resuscitation), then the plan was to: preserve spontaneous ventilation; use awake fiber-optic assist; and, insert a small-sized (5.5mm ID) reinforced tracheal tube (Rusch R). Consultants experienced with rigid bronchoscopy were on standby; cricothyroidotomy or tracheotomies were not feasible. We planned any needed post-cesarean analgesia using PCEA with infusion of local anesthetic with/without low concentrations of lipid soluble epidural opioids and/or adjuvant intravenous dexmedetomidine [14]. After abdominal delivery, the patient would have been kept in an area of “intensive nursing” during the period of epidural infusion. Advanced planning was done to insure immediate availability of the proper resources, both materials (such as the helium/oxygen tanks and breathing apparatus) and personnel (availability of expert bronchoscopists) required to execute our plan of management. Discussion among the different physician and nursing groups involved in our patients’ care led us to our decision to manage these two patients on our Labor and Delivery Unit; and, not having them labor and deliver in an Intensive Care Unit or in a general-purpose operating room. Fetal safety of inhaled maternal helium has never been proven. However, helium is an inert gas. Fetal (neonatal) blood concentrations should decrease quickly after discontinuation of maternal inhalation (or delivery). In the gravid ewe model, short-term inhalation of 80% helium leads to a maternal blood helium concentration of about 7% with fetal blood helium concentration of about 1% [15]. In neither case presented was there decompensation of the electronic fetal heart rate recording associated with inhalation of helium. Each neonate was born vigorous.
Summary
Key in these two cases was early evaluation and careful multidisciplinary planning, including (but not limited to): “early” labor determination of a “working “neuraxial catheter; allowing a passive second stage; willingness to accept/perform operative vaginal delivery;“stand-by” assistance with rigid bronchoscopy; and, gathering of resources/equipment (e.g. canisters, blenders) to the labor suite. We believe that inhalation of helium-oxygen provided significant therapeutic benefit during labor. Given the ameliorating effects of inhaled helium/oxygen on maternal respiratory function, that helium is an inert gas, and it should be easily excreted across the placenta or lungs after birth, we would not hesitate to administer helium/oxygen to any future parturient suffering from respiratory distress secondary to a pathologic narrowing of the airway.
Author Contributions
1. Omar Alyamani MBBS: Planned and executed clinical care, planned and co-author of the manuscript
2. Shobana Bharadwaj MBBS: Planned and executed clinical care, planned and edited the manuscript
3. SrikarJonna MD: executed clinical care and contributed to the writing of the manuscript
4. Justin Li MD: executed clinical care and contributed to the writing of the manuscript
5. Andrew M Malinow MD: Planned, and authored manuscript Consent: obtained; approved by the Human Research Protection Office (UMB)
References
-
Harris PD, Barnes R (2008) The uses of helium and xenon in current clinical practice. Anaesthesia 63(13): 284-293.
-
Mallett V, Bhatia R, Kissner D, Sokol R (1989) Use of an HeO2 mixure in the management of upper airway obstruction during labor and delivery: A case report. J Reprod Med 34(6): 429-430.
-
Barach AL, Morris Eckman (1936) Effects of the Inhalation of Helium Mixed with Oxygen on the Mechanics of Respiration J Clin Investigation 15(1): 47-61.
-
Gaiser R: Physiologic changes in pregnancy. InChestnutDH, WongCA, Tsen LC, Ngan Kee WD, BeilinY, Myhre JM eds. Chestnut’s Obstetric Anesthesia: Principles and Practice, fifth edition. Phila: Elsevier/Saunders 201:22.
-
Hingson RA (1956) Western Reserve portable miniature anesthesia machine, resuscitator and oxygen inhalator in obstetrics. In Hingson RA, Hellman LM (Eds.) Anesthesia for Obstetrics. Phila: Lippincott; 167-176.
-
Richardson MG, Lopez BM, Baysinger CL, Shotwell MS, Chestnut DH (2017) Nitrous oxide during labor: maternal satisfaction does not depend exclusively on analgesic effectiveness. Anesth Analg 124(2): 548-530.
-
Ho AM, Dion PW, Karmakar MK, Chung DC, Tay BA (2002) Use of heliox in critical upper airway obstruction. Physical and physiologic considerations in choosing the optimal helium:oxygen mix. Resuscitation 52(3): 297-300.
-
Novikova N, Cluver C (2012) Local anaesthetic nerve block for pain management in labour. Cochrane Database Syst Rev.
-
Leighton BL, Halpern SH, Wilson DB (1999) Lumbar sympathetic blocks speed early and second stage induced labor innulliparous women. Anesthesiol 90(4): 1039-1046.
-
Abu Halaweh SA, Al Oweidi A KS, Abu Malooh H, Zabalawi Majd, Alkazaleh Fawaz, et al. (2009) Intravenous dexmedetomidine infusion for labour analgesia in patient with preeclampsia. Eur J Anaesthesiol 26(1): 86-87.
-
Joel S, Joselyn A, Cherian VT, Nandhakumar A, Raju N, et al. (2014) Low-dose ketamine infusion for labor analgesia: A double-blind, randomized, placebo controlled clinical trial. Saudi J Anesth 8(1): 6-10.
-
Greenhill JP (1945) Direct infiltration anesthesia in obstetrics. In Lull CB, Hingson RA eds. Control of Pain in Childbirth. 2nd edition. Phila: Lippincott 215- 219
-
Sen S, Ozmert G, Aydin ON, Baran N, Caliskan E (2005) The persistent analgesic effect of low-dose intravenous ketamine after spinal analgesia for Caesarean section. Eur J Anaesthesiology 22(7): 518-523.
-
Palanisamy A, Klickovich RJ, Ramsay M, Ouyang DW, Tsen LC (2009) Intravenous dexmedetomidine as an adjunct for labor analgesia and cesarean delivery anesthesia in a parturient with a tethered spinal cord. Int J Obstet Anesth 18(3): 258-261.
-
Spencer JAD, Anderes DC, Wollner JC, Wolton R, Rolfe P, Johnson P (1986) A technique for continuous measurements of materno-fetal gas transfer using mass spectrometry suitable for non- invasive intrapartum placental function testing in man. In Rolfe P (Eds.) Fetal Physiologic Measurements: Proceedings of the Second International Conference on Fetal and Neonatal Physiological Measurements. London: Butterworths 185-194.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index