Case Report about Co-Axial Circuit Causing Hypercarbia
Bain Co-axial anesthesia circuits have been used to administer general anesthesia since 1972. Co-axial circuits have many benefits, however in current anesthesia practice they have one significant pitfall that is undetectable during automated machine checkout. Disconnection of the inner tube of a co-axial breathing circuit leading to hypercarbia and high inspiratory Carbon Dioxide can go unrecognized during machine checkout. We present an anesthetic case where immediately after induction of anesthesia, hypercarbia and high inspiratory Carbon Dioxide were recognized. Troubleshooting ensued and a proximal disconnection of the inner tube of the co-axial circuit was discovered. Prior to induction of anesthesia utilizing a co-axial circuit, visual inspection of the circuit integrity should be performed until technology advances and a method is developed to detect this type of disconnection.
Background
The Bain’s co-axial circuit is popular in anesthesia practice for its lightweight and adaptable design. In recent years, its co-axial design has been adapted for circle absorbers where the afferent limb is contained within the outer efferent portion of the circuit. There are many published reports of malfunction of the inner tube of the Bain’s co-axial circuit [1, 2]. We report a case where an unrecognized proximal disconnection of the inner tube of a co-axial breathing circuit led to high inspiratory baseline of the capnography and false scare of malignant hyperthermia.
Case Presentation
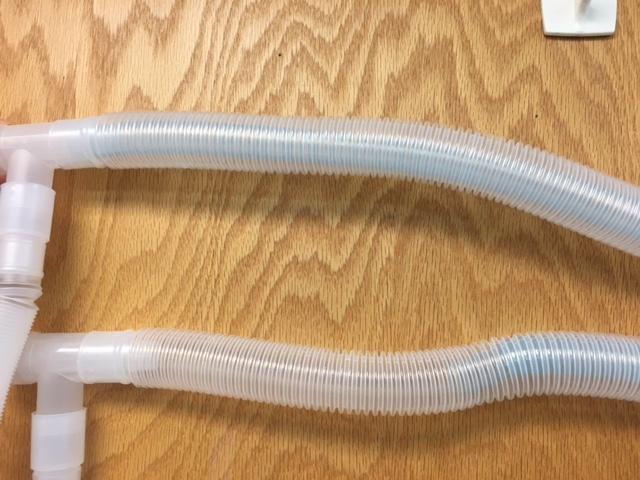
A 29-year-old female patient, weighing 59 kg, ASA 1, was scheduled for vaginal hysterectomy. Preoperative assessment revealed acceptable pulmonary function, complete blood count, and renal function. Hemodynamic parameters and body temperature were within normal limits. There was no documented family history of malignant hyperthermia. A routine self-check was performed on a Draegar Perseus A500 anesthesia machine and showed ready-to-use status with no alarms. The patient received 2 mg midazolam premedication, and the induction of anesthesia was accomplished with intravenous fentanyl 100mcg, propofol 150mg, and vecuronium 10mg; the trachea was intubated with 7mm endotracheal tube and connected to a Draeger Perseus A500 anesthesia machine via a Westmed Unilim co-axial circuit. Anesthesia was maintained with 2% sevoflurane and 100% oxygen. Vital signs monitored included blood pressure, pulse oximetry, electrocardiogram and end tidal carbon dioxide (ETCO2). A Foley catheter was placed. Within the first few minutes of induction, it was noticed that the ETCO2 was increasing progressively from an initial 38 to 67 mmHg. The baseline of the capnogram showed an upward shift of the inspiratory carbon dioxide (IMCO2), indicating rebreathing. The soda lime canister was cool to the touch and non-discolored but was still changed to fresh absorbent. This did not change the findings on the capnography. The minute ventilation was increased to 12 L/min and the I: E ratio adjusted to 1:1 without any corresponding significant decrease in the ETCO2 or IMCO2 values. The capnography sensor and gas sampling line tubing was changed. When no improvement resulted, the ETT was disconnected from the co-axial circuit. An Ambu bag with a clear elbow connector together with new gas sampling line was connected to the ETT, and manual ventilation was initiated using an auxiliary oxygen source on the anesthesia machine. Additional help was called and a malignant hyperthermia cart was requested. The hemodynamic parameters and body temperature remained normal. Within a few minutes of manual ventilation, the capnography showed a dramatic return of ETCO2 to 35 mmHg with no inspiratory CO2. The co-axial circuit on the machine was replaced and old circuit was inspected. Sevoflurane was turned off and activated carbon filters were placed on the new circuit. Total intravenous anesthesia was initiated using a propofol infusion. After confirming normal ventilator performance by running self-check, the ETT was reconnected to a new circuit. Capnography showed a normal ETCO2 of 40 mmHg and a return of baseline IMCO2 to zero. It was determined that hypercarbia was not due to increased production from a hypermetabolic state, but rather, from improper elimination leading to significant rebreathing of CO2. The surgery was completed, and the patient was extubated with no adverse postoperative event. The inspiratory and expiratory valves of the anesthesia machine were examined after the procedure and were found to be intact and functioning well. Further visual examination of the faulty co-axial circuit revealed intact outer transparent tubing, while the inner blue inspiratory tube was found disconnected from its proximal seating (Figure 1). Displacement of this nature may not be easily detected without careful observation of the circuit components.
Discussion
Bain’s co-axial circuit was introduced into anesthesia practice in 1972 by Bain and Spoerel [3]. The inner, colored inspiratory tube can malfunction or be defective. Any disconnection or loss of integrity increases the dead space profoundly, leading to hypercapnia and its complications. Several reports implicating detachment of the inner tube and consequent hypercarbia have been published since the introduction of the Bain co-axial circuit [4, 5]. We suggest a few ways to address this problem. The first option is for the manufacturer to redesign the co-axial circuit to make the outer tubing very transparent so as to facilitate visualization of the inner tube and its connection to its seating. The second option is to avoid using co-axial circuits and to use separate limbs for inspiration and expiration. The final option would be to develop appropriate low pressure checks and alarms to sense this type of disconnection. The following causes of intraoperative hypercarbia have been conventionally listed: Ventilatory – hypoventilation, bronchial intubation, rebreathing, COPD and asthma. Metabolic – Malignant hyperthermia, fever, sodium bicarbonate therapy and tourniquet release. Mechanical – exhausted soda lime CO2 absorber, malfunctioning expiratory/ inspiratory valves, inadequate fresh gas flow and water in sampling adapter/tubing. We must now also consider a disconnection of the central inner tube of co-axial breathing circuit as a factor that could cause rebreathing of CO2, leading to intraoperative hypercarbia. Various methods for testing the central inner tube integrity for co-axial circuits have been proposed, all of which rely on pressurization of the circuit or the creation of a Venturi effect [6]. Because the circuit used in this case was intact from outside and passed the self-check test, we did not detect the problem before surgery. The normal capnogram [7] should not have any inspired CO2. (Figure 2)
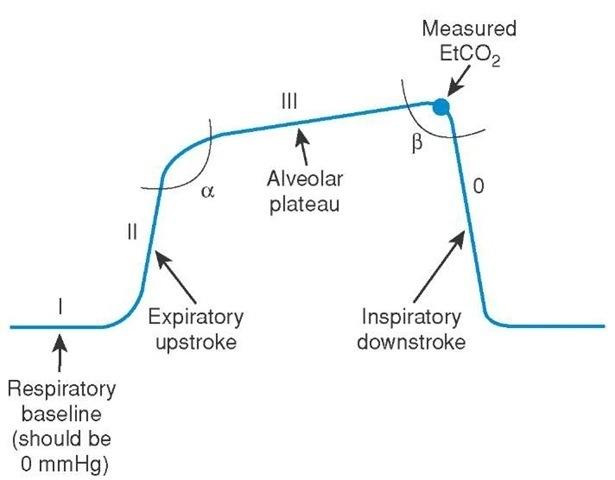
Figure 2: Expiratory limb: Phase I – CO2 from anatomic dead space; Phase II – transition from dead space to alveolar gas; Alpha angle – between Phase II and III is indirect indicator of V/Q status; Phase III – CO2 from alveoli; Inspiratory limb: Beta angle – between Phase III and inspiratory down stroke; Phase O – Beginning of next inspiratory cycle. The most common causes of inspired CO2 seen in capnogram are as follows:
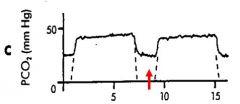
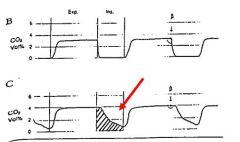
Increased apparatus dead space – can be seen in pediatric cases with extra-long circuit; elevated ETCO2 level with normal ETCO2- arterial CO2 gradient seen. Exhausted soda lime CO2 absorber – usually detected by change in color of soda lime granules to purple color; elevated ETCO2 level with normal ETCO2-arterial CO2 gradient seen. Incompetent unidirectional valves will show elevated ETCO2 level with decreased ETCO2-arterial CO2 gradient seen. Expiratory valve malfunction will show elevated baseline, normal B-angle and rebreathing occurs during expiratory limb of waveform (Figure 3).
We share this case report as a warning and a reminder that the integrity of the co-axial circuit must be visually inspected before inducing general anesthesia. We would like to add a disclaimer that the views expressed in this article do not necessarily represent the views of the VA hospital or United States government.
References
-
Jellish WS, Nolan T, Kleinman B (2001) Hypercapnia related to a faulty adult coaxial breathing circuit. Anesth Analg 93(4): 973-974.
-
Youssef EY, Iyasere G (2010) Severe intraop hypercapnia complicating unusual malfunction of inner tube of coaxial bain’s circuit. Oman med J 25.
-
Bain JA, Spoerel WE (1972) A streamlined anesthetic system. Canadian Anaes Soc J 19: 426.
-
Ghai B, Makkar JK, Bhati A (2006) Hypercarbia and arrhythmias resulting from faulty Bain circuit. Anesth Analg 102(6): 1903-1904.
-
Gooch C, Peutrell J (2004) A faulty Bain circuit. Anesthesia 59(6): 618.
-
Heath PF, Marks LF (1991) Modified occlusion tests for the Bain breathing system. Anesthesia 46(3): 213- 216.
-
Kodali, Bhavani Shanker Physiology of capnography.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index