Migration of Central Venous Catheter into the Pleural Space: A Rare Fatal Complication Averted
A 63 year old female operated for aortic valve replacement had a complication of a misplaced subclavian central venous catheter into the pleural space. A major complication was averted because of the chest tube drain which was placed intraoperatively and a quick diagnosis by visualization of the serous drainage in the immediate postoperative period.
Introduction
Central venous catheters has gained a widespread application as an important access for fluid administration, inotropes, chemotherapy and other uses like central venous pressure monitoring, transvenous cardiac pacing, measurement of central venous oxygen saturation. The optimal position of the tip of CVC’s is still a debate [1, 2]. The most accepted position of the catheter should be inside a large central vein either superior vena cava or inferior vena cava, ideally outside of the pericardial sac, and parallel with the long axis of the vein, such that the tip does not about the vein or the heart wall at an acute angle or end [3]. Any deviation from the above said position can misplace the tip of the catheter.
Case Report
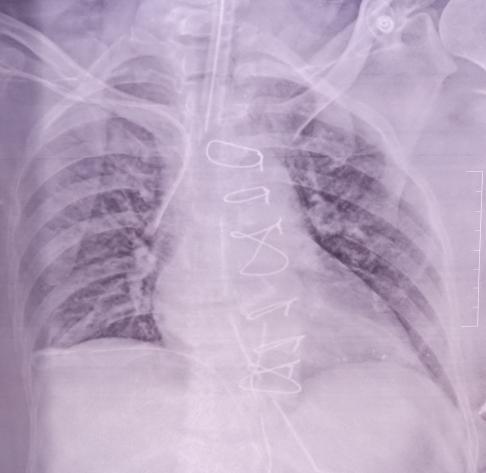
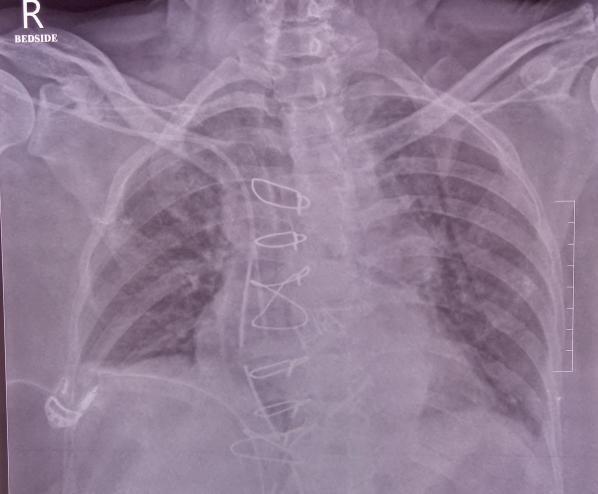
A sixty three years old female underwent aortic valve replacement under general anaesthesia. Post induction patient was positioned for subclavian vein central venous cannulation with a 7Fr. Triple lumen catheter and the catheter was placed successfully. Intra vascular placement of catheter was confirmed by aspiration of blood in all the three ports. Initially there was some resistance in the back flow of blood in the central lumen though other lumen had a good back flow. Patient underwent aortic valve replacement under cardiopulmonary bypass. While weaning of the CPB, patient was started on inotropes and connected to the proximal ports and the central port was kept free for intravenous boluses and for CVP measurement. Throughout the procedure and during the postoperative period CVP measurement was low; the inotropes connected was well acting. Immediate post-op CXR was taken and catheter was well placed though it was little lateral to the SVC (Figure 1). In the first postoperative day CXR was repeated as per the institute’s protocol the catheter tip was found to be displaced laterally compared to the previous CXR (Figure 2). Aspiration attempted in all the ports but no free flow of blood seen. Incidentally IV paracetamol injection was given in the central port of the CVC over 10 Min. Suddenly the chest drain had 100 ml of serous fluid after infusion of the IV paracetamol. We suspected of catheter migration into the pleural space and the catheter was partially withdrawn till free flow of blood aspiration was confirmed and a guide wire is passed at that position and the CVC is inserted via the same site with free flow after full placement of the catheter. Check X-ray was done which was well placed in position (Figure 3). Since this patient had a pleural and a meditational drain placed insitu, there was no collection of fluid or blood in the pleural or pericardial space after repositioning of the catheter.

Discussion
The complication arising out of placing central venous catheter is not uncommon. A complication in subclavian vein cannulation is more compared to internal jugular cannulation. Although in most of the cardiac surgical centres, internal jugular vein is preferred, in our institute we prefer to cannulate the subclavian vein in view of prolonged CVP access, easy maintenance and good patient tolerability. In this case there was initial resistance while passing the guide wire, we suspected of CVC in the in nominate vein. The other possibilities could be right internal thoracic vein and right pericardiophrenic vein. The internal thoracic vein arises from the superior epigastric vein and drains into brachiocephalic vein. The pericardiophrenic veins are the vena comitans of the pericardiophrenic arteries and drains into the internal thoracic or brachiocephalic vein. In the postoperative CXR, the tip was lateral to the SVC and the possibility of the catheter tip being in the internal thoracic or pericardiophrenic vein could not be ruled out. The sudden gush of serous fluid in the chest drain following paracetamol infusion made us to confirm that the tip was in the pleural space. Misplaced catheters have been reported in all possible anatomical position which includes arteries, mediastinum, pleura, pericardium, trachea, oesophagus, sub-arachnoid space and other aberrant sites. The misplacement can occur at any time which may be during the time of insertion or it may occur during later stages, the cause of it could be migration of the tip. Migration of the tip of the catheter to the pleural space has been reported in literature with fatal complication with hemothorax, pericardial tamponade, pneumothorax or pleural effusions [4, 5, 6, 7]. It has been radio graphically demonstrated that the catheter tip can significantly move up cephalad, from mid-right atrium to low SVC, when the patient sits up; this migration was greater for CVC placed in the subclavian veins in females and in obese patients [8]. Mild tip migration has also been described in association with breathing movements. A mean variation of 9mm of catheter tip movement was observed in expiration, but not in inspiration [9]. In this case we found to see the tip migration in later stages through the chest x- ray taken in the post operative day 1 and the sudden gush of fluid in the chest drains. To prevent malposition of the catheters various techniques have been studied. When a subclavian approach is used, making certain that the J-tip of the guide wire must be pointed caudad during insertion improves its successful guidance [10]. Other technique to prevent misplacement of catheter into the internal jugualar vein is to compress the ipsilateral jugular vein [11] or to flex the head towards the ipsilateral side which can narrow the os of the internal jugular vein [12]. This patient though a fatal complication is prevented by early diagnosis and the exit point would have been above the superior vena cava there was no tamponade or bleeding. Major complications of misplacement of the tip of central venous catheters can be prevented by meticulous placement with a proper knowledge of the anatomy of the vessels and imaging during cannulation plays a major role in a successful placement. Checking all the ports for aspiration of blood, x-ray, and CVP measurement can confirm the presence in the proper anatomy.
Conclusion
Even though there is advancement in the techniques of insertion, the placement of catheters is not without any complication. Extreme diligence is needed while placing a central venous catheter to avoid complications.
References
-
Fletcher SJ, Bodenham AR (2000) Editorial II: Safe placement of central venous catheters: where should the tip of the catheter lie? Br J Anaesth 85(2): 188- 191.
-
Vesely TM (2003) Central venous catheter tip position: a continuing controversy. J Vasc Interv Radiol 14(5): 527-534.
-
Gibson F, Bodenham A (2013) Misplaced central venous catheters: applied anatomy and practical management. Br J Anaesth 110(3): 333-346.
-
Schummer W, Schummer C, Rose N, Niesen WD, Sakka SG (2007) Mechanical complications and malposition of central venous cannulations by experienced operators. A prospective study of 1794 catheterizations in critically ill patients. Intensive Care Med 33(6): 1055-1059.
-
Walshe C, Phelan D, Bourke J, Buggy D (2007) Vascular erosion by central venous catheters used for total parenteral nutrition. Intensive Care Med 33(3): 534-537.
-
Merrer J, De Jonghe B, Golliot F, Lefrant JY, Raffy B, et al. (2001) Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. JAMA 286(6): 700-707.
-
Granziera E, Scarpa M, Ciccarese A, Filip B, Cagol M, et al. (2014) Totally implantable venous access devices: retrospective analysis of different insertion techniques and predictors of complications in 796 devices implanted in a single institution. BMC Surg 14: 27.
-
Nazarian GK, Bjarnason H, Dietz CA Jr, Bernadas CA, Hunter DW (1997) Changes in tunneled catheter tip position when a patient is upright. J Vasc Interv Radiol 8 (3): 437-441.
-
Pan PP, Engstrom BI, Lungren MP, Seaman DM, Lessne ML, et al. (2013) Impact of phase of respiration on central venous catheter tip position. J Vasc Access 14(4): 383-387.
-
Tripathi M, Dubey PK, Ambesh SP (2005) Direction of the J-tip of the guidewire, in Seldinger technique, is a significant factor in misplacement of subclavian vein catheter: a randomized, controlled study. Anesth Analg 100(1): 21-24.
-
Kusminsky RE (2007) Complications of Central Venous Catheterization. J Am Coll Surg 204(4): 681- 696.
-
Ambesh SP, Dubey PK, Matreja P, Tripathi M, Singh S (2002) Manual occlusion of the internal jugular vein during subclavian vein catheterization: a maneuver to prevent misplacement of catheter into internal jugular vein. Anesthesiology 97(2): 528-529.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index