An Anesthetic Management of Emergency Caesarean Section through Low-Dose Sequential Combined Spinal-Epidural Blockade with Maternal Wolff-Parkinson-White Syndrome
Wolff-Parkinson-White (WPW) syndrome is a rare conduction system disorder of the heart that the abnormal accessory conduction pathway is located in between the atriums and ventricles. The anesthetic management of WPW syndrome patients is challenging because it can cause life threatening complication such as paroxysmal supraventricular tachycardia (PSVT) or atrial fibrillation. However, the most effective anesthetic management of WPW syndrome patient has not well been reported. The authors faced a WPW pregnant patient who requires emergency caesarean section due to fetal destress, and considered epidural anesthesia for rapid onset as emergency condition. We performed low-dose sequential combined spinal-epidural blockade (CSE) for anesthesia. Spinal anesthesia was performed with less than conventional dose due to hemodynamic stability, and additional local anesthetic injection through the epidural catheter. We describe a case of WPW patient who had emergency cesarean section and review the anesthetic management of WPW syndrome.
Jun Ho Lee1,2*, Minjong Ki1, Ki Jae Lee1, Jeong Seob Kim1 and Deokkyu Kim1
Medical School and Hospital, Korea
250-1240; Email: gojuno@yahoo.com
syndrome.
An Anesthetic Management of Emergency Caesarean Section through Low-Dose Sequential Combined Spinal-Epidural Blockade with Maternal Wolff-Parkinson-White Syndrome
Introduction
Cardiac arrhythmia is one of the most common cardiac complications in pregnancy [1]. Although the mechanism Anaesth Critic Care Med J
of increased arrhythmia in pregnancy is still not clearly understood, it is likely caused by a combination of hemodynamic, hormonal, and autonomic changes [2]. Among the cardiac arrhythmias the most common arrhythmia is paroxysmal supraventricular tachycardia (PSVT), and Wolff-Parkinson-White (WPW) syndrome also presents considerable frequency [3].
WPW syndrome is a conduction system disorder of the heart that is caused by the abnormal accessory conduction pathway is located in between the atriums and ventricles. It is also generally known as pre-excitation syndrome. The prevalence of WPW syndrome is about 0.1 - 0.3%, and up to 50% of the patents can develop paroxysmal tachycardia including PSVT, atrial fibrillation and less commonly atrial flutter [4]. Ventricular fibrillation can be precipitated by a critically timed premature atrial beat that travels down the bypass tract and catches the ventricle at a vulnerable period. These may induce myocardial ischemia, hypoperfusion and hypoxia [5].
Pregnancy promotes the development of tachycardia in asymptomatic pre-excitation syndrome patients. During pregnancy, physiologic volume overload can lead to elevate the left ventricular end-diastolic pressure, which can increase myocardial hypersensitivity [3]. Furthermore, because significant changes in the physiology of conduction and predisposition caused by drugs and techniques used in emergency cesarean section may increase the risk of mothers and fetuses, understanding proper anesthetic management of WPW syndrome is important. Here, we present a case of asymptomatic WPW patient who had emergency cesarean section due to fetal distress and review the anesthetic management of WPW syndrome.
Case Report
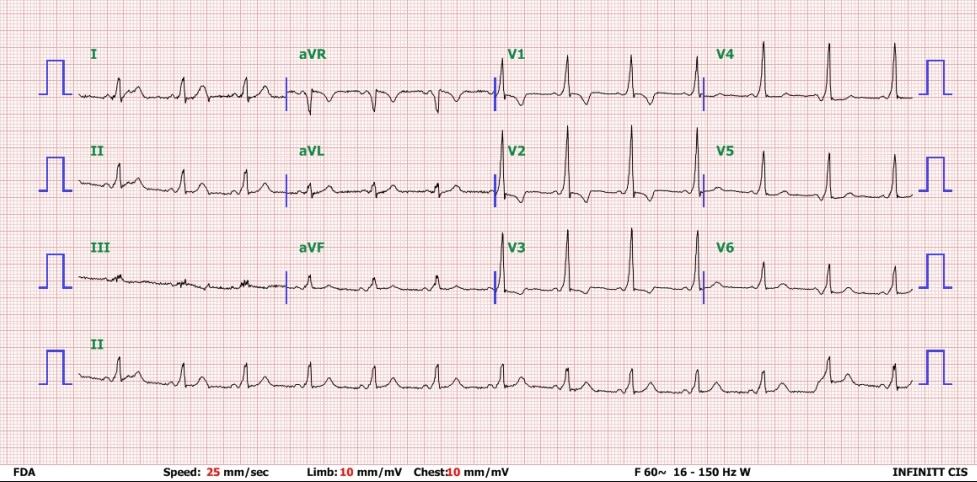
A 40-year-old female patient with 40 weeks of pregnancy diagnosed with WPW syndrome was admitted for emergency cesarean section with fetal distress. Her weight was 72 kg, height was 153 cm and BMI was 30.8. She had history of abortion three times previously, and had never been diagnosed as WPW syndrome. In the department of our ER she was diagnosed as WPW syndrome for the first time. Other medical history was not documented. At admission of operating room, initial vital sign was blood pressure 112/78 mmHg, heart rate 78 beats /min, respiratory rate 20 breaths /min, Oxygen saturation 98%. She had fasted more than 8 hours before surgery, and there was no abnormal sign in the complete blood count, chemistry, coagulation profiles, Chest X-ray and electrocardiography. The electrocardiogram presented a typical finding of WPW syndrome (Figure 1). In lead I, II and V1-6, short PR intervals and “delta waves” were found. A delta wave is indicated as slurring of the upstroke of the QRS complex.
Jun Ho Lee, et al. An Anesthetic Management of Emergency Caesarean Section through Low-Dose Sequential Combined Spinal-Epidural Blockade with Maternal Wolff-Parkinson-White Syndrome. Anaesth Critic Care Med J 2019, 4(3): 000156.
of sudden cardiac complication, the emergency cart containing defibrillator and anti-arrhythmic drugs was Copyright© Jun Ho Lee, et al.
prepared. The CSE was performed with needle-through- needle technique. Hartmann’s solution 0.5L was preloaded. After the patient was positioned in the left lateral position, 18G Tuohy needle was placed in the epidural space at L4/5 interspace through loss of resistance technique. Then, 27G Quincke needle was inserted through the 18G Tuohy needle, and 1.6ml of 0.5% hyperbaric bupivacaine with fentanyl 15mcg was injected in the subarachnoid space. An epidural catheter was inserted through 18G needle and it was fixed. Sensory was blocked up to T6 level, and the patient was tilted to the left lateral about 15 to 20 degrees due to prevention of supine hypotensive syndrome. The block was extended to T4 level after 10ml of 0.375% ropivacaine injection through epidural catheter.
The section was done by Pfannenstiel incision. Ten minutes after the skin incision, a neonate was born with Apgar score 9 for 1 min and 10 for 5min. Hemodynamic parameters were not significantly changed during intraoperative period, and the operation was safely terminated without the use of vasopressors or antiarrhythmic agents. After surgery blood pressure was 120/70 mmHg and heart rate was 55bpm. Postoperative analgesia was using epidural patient controlled analgesia with 0.1% ropivacaine, and sensory block was maintained with T8 level. The patient was discharged 4 days after surgery without complications such as hemorrhage or arrhythmia in perioperative period.
Discussion
There is no specific guideline of anesthetic management in patient with WPW syndrome, but the goal of anesthetic management of WPW syndrome is to avoid sympathetic activity that can cause supraventricular tachycardia such as pain, anxiety, stress response of intubation, lighter plane of anesthesia and hypovolemia [6]. There are a few hypothetical mechanisms that explain the increasing tendency of arrhythmia in pregnancy. Most of the mechanisms explain that hemodynamic, autonomic, hormonal and emotional changes related in pregnancy increase plasma catecholamine concentration, adrenergic receptor sensitivity, atrial stretch and end diastolic volumes due to intravascular volume expansion [7]. It is important to maintain a balance between sympathetic and parasympathetic nerves for safe anesthetic management for patients with WPW syndrome. Regional anesthesia has been known that has a significant advantage over general anesthesia due to less drug Jun Ho Lee, et al. An Anesthetic Management of Emergency Caesarean Section through Low-Dose Sequential Combined Spinal-Epidural Blockade with Maternal Wolff-Parkinson-White Syndrome. Anaesth Critic Care Med J 2019, 4(3): 000156.
administration and less sympathetic stimulation by intubation.
The recommended dose of hyperbaric bupivacaine for cesarean section under sufficient spinal anesthesia to reach T4 level block is 10 to 15mg [8]. However, WPW syndrome cases under spinal anesthesia alone have rarely been reported. Most of the WPW cases have used relatively low dosage of bupivacaine (7.5 – 9mg) with additional opioids [9, 10]. Many anesthetic strategies have been tried to prevent spinal induced hypotension including low dose local anaesthetics. In a systemic review, low dose bupivacaine less than 8mg decreases the side effects such as hypotension, nausea and vomiting, but the effect of anesthesia is also decreased. Thus, requirement for additional analgesics and the rate of conversion to general anesthesia can be increased with low dose anaesthetics [11]. Anesthesia induced hypotension is the most frequent complication of pregnant patient undergoing cesarean section under spinal anesthesia. For that reason, it may be necessary to use drugs such as ephedrine, epinephrine or atropine in case of bradycardia or hypotension. However, those drugs can induce tachycardia. Furthermore, pain and anxiety after incomplete blockade also can induce tachycardia [12]. Epidural anesthesia is preferred to the spinal anesthesia because epidural has better effect of controlled and segmental block with hemodynamic stability [13]. Epidural anaesthesia is hemodynamically more stable, but the onset is slower than spinal anesthesia, so that it may not be relevant to emergency operation. In this case, CSE was chosen because we wanted advantages of both spinal and epidural anesthesia such as rapid onset of spinal anesthesia and hemodynamic stability of epidural anesthesia. According to McNaught, epidural volume extension and low-dose sequential combined spinal- epidural blockade can reduce spinal dose requirement which prevents decrease of anesthetic efficacy. A small dose with epidural supplementation using local anesthetics helps to reduce hypotension and provides better cardiovascular stability for high risk patients [14].
WPW syndrome patients require anesthetic management with an emphasis on prevention of intraoperative sympathetic stimulation such as pain, anxiety and light anaesthetics due to decrease of anesthetic efficacy. Low-dose spinal anesthesia has a risk of maintaining adequate anesthesia in WPW patient. Because it was an emergent situation due to fetal distress, we selected epidural volume extension and low-dose sequential combined spinal-epidural blockade as a Copyright© Jun Ho Lee, et al.
method of anesthesia considering safety and promptness. The authors performed spinal anesthesia with lower than usual recommended dose for hemodynamic stability, and applied epidural volume extension by injecting local anaesthetics using epidural catheter considering possible side effects caused by decreased anesthetic efficacy.
Low-dose sequential combined-epidural blockade extends the local anaesthetics through the dural puncture site, thecal compression and atmospheric pressure in the epidural space. Skillful technique should be required because the epidural extension is unpredictable and there is a risk of high spinal block when hyperbaric bupivacaine is used. Compared with conventional spinal anesthesia, low-dose sequential combined-epidural blockade has advantages that reduce the incidence of hypotension, motor block, and pain. In summary, WPW syndrome is a cause of supraventricular tachycardia in pregnancy. When a patient with WPW syndrome requires caesarean section, low-dose sequential combined spinal-epidural blockade can be considered as an effective method of anesthesia.
Acknowledgment
This case report was supported by funds from the Biomedical Research Institute of Chonbuk National University Hospital, Jeonju, South Korea.
References
-
Siu SC, Sermer M, Colman JM, Alvarez AN, Mercier LA, et al. (2001) Prospective Multicenter Study of Pregnancy Outcomes in Women with Heart Disease. Circulation 104(5): 515-521.
-
Enriquez AD, Economy KE, Tedrow UB (2014) Contemporary Management of Arrhythmias During Pregnancy. Circulation: Arrhythmia and Electrophysiology 7(5): 961-967.
-
Burkart TA, Conti JB (2010) Cardiac arrhythmias during pregnancy. Curr Treat Options Cardiovasc Med 12(5): 457-471.
-
Vaidya VR, Arora S, Patel N, Badheka AO, Patel N, et al. (2017) Burden of Arrhythmia in Pregnancy. Circulation 135(6): 619-621. Jun Ho Lee, et al. An Anesthetic Management of Emergency Caesarean Section through Low-Dose Sequential Combined Spinal-Epidural Blockade with Maternal Wolff-Parkinson-White Syndrome. Anaesth Critic Care Med J 2019, 4(3): 000156.
-
Butterworth JF, Mackey DC, Wasnick JD, Morgan GE, Mikhail MS (2018) Morgan & Mikhail's clinical anaesthesiology.
-
Kabade S, Sheikh S, Periyadka B (2011) Anaesthetic management of a case of Wolff-Parkinson-White syndrome. Indian Journal of Anaesthesia 55(4): 381- 383.
-
Tan HL, Lie KI (2001) Treatment of tachyarrhythmias during pregnancy and lactation. European Heart Journal 22(6): 458-464.
-
Norris MC (1988) Height, weight, and the spread of subarachnoid hyperbaric bupivacaine in the term parturient. Anaesth Analg 67(6): 555-558.
-
Deviseti P, Pujari VS (2016) Spinal Anaesthesia is Safe in a Patient with Wolff-Parkinson-White Syndrome Undergoing Evacuation of Molar Pregnancy. J Clin Diagn 10(2): 1-2.
-
Palaria U, Rasheed MA, Jain G, Sinha AK (2013) Anaesthetic management of Wolff-Parkinson-White syndrome in a pregnant patient posted for emergency caesarean section. Anaesth Essays Res 7(3): 408-410.
-
Arzola C, Wieczorek PM (2011) Efficacy of low-dose bupivacaine in spinal anaesthesia for Caesarean delivery: systematic review and meta-analysis. Br J Anaesth 107(3): 308-318.
-
Bengali R, Wellens HJ, Jiang Y (2014) Perioperative management of the Wolff-Parkinson-White syndrome. J Cardiothorac Vasc Anaesth 28(5): 1375- 1386.
-
Okamoto T, Minami K, Shiraishi M, Ogata J, Shigematsu A(2003) Repeated supraventricular tachycardia in an asymptomatic patient with Wolff- Parkinson-White syndrome during Cesarean delivery. Can J Anaesth 50(7): 752-753.
-
McNaught AF, Stocks GM (2007) Epidural volume extension and low-dose sequential combined spinal- epidural blockade: two ways to reduce spinal dose requirement for caesarean section. Int J Obstet Anaesth 16(4): 346-353. Copyright© Jun Ho Lee, et al.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index