Fat Embolism Presenting as Amaurosis Fugax: A Case Report
Amaurosis fugax refers to a transient sudden loss of vision in one or both eyes. We describe a patient of fracture shaft femur, who presented with history of 3-4 such episodes in the right eye, after sustaining a road traffic injury. On diagnostic workup, his visual acuity and fundoscopic examination was normal. He underwent an interlocking fixation procedure subsequently, which went uneventful. In the postoperative period, he developed similar recurring episodes followed by a generalized seizure. The repeat investigatory workup showed cerebral and retinal involvement with a presumptive diagnosis of fat embolism. Any intra-cardiac defects, pulmonary vascular shunts and systemic symptoms were however not evident. This case highlights the variations in the clinical presentation of fat embolism syndrome and discusses the differentiation with other look-alike conditions.
Introduction
Unilateral transient loss of vision is a rare initial presentation in fat embolism syndrome (FES). We present a 25-year-old male with shaft femur fracture, having a cerebral and retinal involvement suggesting fat embolism, in absence of any respiratory symptoms, cutaneous signs or a cardiopulmonary shunt.
The paramedics brought in a 25-year-old male 4 hours later, after sustaining a road traffic injury and complaining of excruciating pain in the right lower limb. The patient had 3-4 episodes of sudden, transient, and painless loss of vision in the right eye, an hour back. On physical examination, his right thigh was swollen and deformed, vitals were stable, and had no comorbidities. The visual acuity and the fundoscopic examination were normal. The radiological survey revealed a right mid-shaft femur fracture, while other investigations were within normal limits. To immobilize the fracture, we applied a long-leg splint-traction. The following day, patient underwent an uneventful interlocking fixation procedure under the regional anaesthesia.
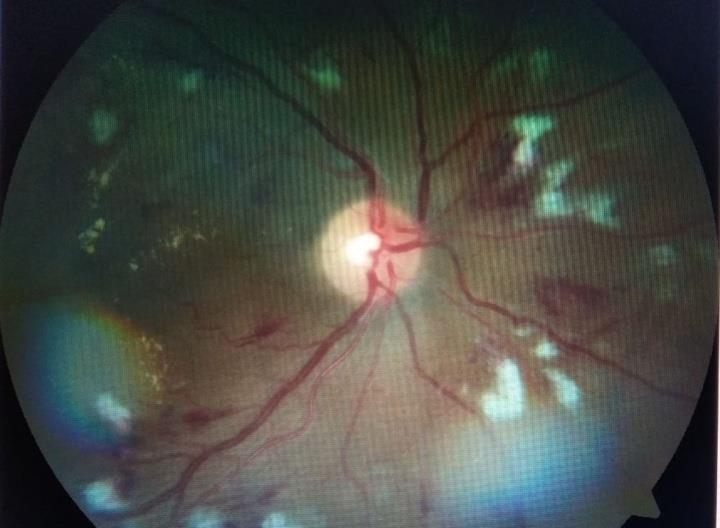
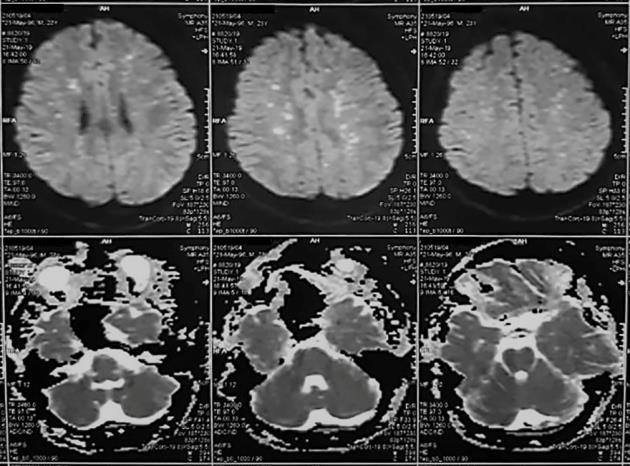
After a symptom-free period of 6 hours, the patient complained of sudden, transient blackout of vision in the right eye. There were 5-7 such episodes and felt like “on and off” movement of shades over the visual field. Each incident lasted for about 30-90 seconds, over a span of 15 minutes. The fundoscopy revealed some cotton wool spots (CWS) following the path of dilated retinal blood vessels in the right eye, suggestive of retinal ischemia (Figure 1). After an hour, the patient developed a sudden episode of generalized tonic-clonic seizure, reverted promptly by administering a bolus dose of Injection Midazolam 4mg intravenously (IV). His postictal Glasgow coma score (GCS) was six (E2V1M3), but had stable cardiorespiratory parameters. We started Injection Levetiracetam 500 mg IV twice a day and shifted the patient to the critical care unit for further management. Laboratory investigations showed increased erythrocyte sedimentation rate (42 mm/hr), decreased Haemoglobin (8mg/dl), and decreased platelets (1.2 lac/mm3). The Echocardiogram, Chest radiograph, and the Carotid/lower limb Doppler were normal. Due to persistently poor GCS and the blunt airway reflexes, we intubated the patient and placed him on invasive mechanical ventilation (pressure assisted controlled mode). We performed a CT pulmonary angiography, but it was within the normal limits. The Electroencephalogram showed a generalised slowing, with background activity suggestive of generalized cerebral dysfunction. To investigate the intracranial cause, we performed a non-contrast Computed tomography (CT) scan, which showed diffuse cerebral oedema. The Magnetic resonance (MR) imaging brain obtained the following day, revealed discrete white matter hyperintensities in the bilateral corona radiata and centrum semi ovale (Figure 2). The diffuse weighted images showed a “star field pattern”, with multiple hyper- intense foci against the white matter background. The patient had persistent tachycardia (130/minute), and mild pyrexia (100°F), but had normal arterial blood gas parameters and negative culture reports. The urinary examination was negative for fat globules. Based on clinical presentation and the radiological workup, we made a diagnosis of FES (based on Gurd’s Criteria) with amaurosis fugax and seizure, possibly due to systemic embolization. We managed the patient conservatively, and his sensorium improved gradually from the 8th postoperative day. The repeat fundoscopy showed few CWS in both eyes, and we extubated the patient on the 10th postoperative day. After extubation, he recognized relatives, was neurologically normal but had a visual acuity of 6/12 in both eyes. Subsequently, we shifted him and on follow up after 1 month, his visual acuity improved to 6/6 in both eyes, with persistent CWS on fundoscopy.
Discussion
FES refers to the constellation of symptoms after migration of the fat emboli via blood circulation into the systemic capillary beds [1]. The fat blocks usually stuck- up in the pulmonary arteries, but they may gain systemic entry in presence of a cardiac shunt or pulmonary arteriovenous fistula. Rarely, the smaller fat droplets (less than 10 micron diameter) may even traverse unaffected through the pulmonary capillaries, leading to systemic embolization [2]. The fat droplets contained within the microcirculation induce direct tissue damage, capillary blockade, and an inflammatory reaction. The diagnosis is always clinical with major complications being a respiratory compromise (95% cases), neurological symptoms (60% cases) and cutaneous changes (50% cases) [1, 3]. The respiratory symptoms range from mild hypoxia to frank respiratory failure, secondary to adult respiratory distress syndrome. The cutaneous manifestations include a generalized petechial rash affecting the torso predominantly, but disappear completely within one week [3]. The cerebral manifestations include diffuse oedema, ischemic stroke or haemorrhage, which presents as altered sensorium or the lateralizing signs, and usually follows respiratory symptoms. The generalized tonic-clonic seizures with subsequent unconsciousness in this patient was likely due to cerebral oedema and the ischemic changes secondary to FES, without any pulmonary or dermal involvement [1, 4]. We could not perform CT or MR angiography (head- neck) for confirmation of cerebral fat embolism, as initial CT pulmonary angiography scan prohibited the repetition of contrast in this patient.
The retinal changes include haemorrhage, exudates (CWS), dilated blood vessels, visible fat emboli, and diffuse oedema in the macular area leading to temporary or rarely permanent loss of vision [5]. This patient presented clinically as the recurring episodes of unilateral transient painless loss of vision, signifying the diagnosis of Amaurosis fugax. The underlying pathology could be fat embolization to the retinal vessels leading to a temporary reduction in the retinal blood supply, which in turn caused retinal ischemia [6]. We excluded the other possible pathologies like intracranial tumour, compressive neuropathy, and optic neuritis by a radiological scan [6]. The optic neuritis causes ocular pain and generally has a rapid, but not sudden loss of vision [6]. A visual aura associated with seizure or migraine, can also cause transient visual loss but it is usually bilateral [6, 7]. The possibility of Purtscher’s retinopathy was ruled out in absence of retinal whitening, atrophic changes around optic disc, retinal pigment epithelium involvement, and early resolution of visual acuity of this patient [5]. Negative echocardiographic findings, absence of hypotension, coagulopathy and papilledema also eliminated the other possible causes of transient monocular vision loss like cardiogenic embolism, cardiac failure, giant cell arteritis, and coagulation disorders, respectively. In conclusion, considering a varying clinical presentation in this patient, we emphasize that FES should be a differential diagnosis for any patient, with initial presentation as Amaurosis fugax after the long bone fractures.
References
-
Kwiatt ME, Seamon MJ (2013) Fat embolism syndrome. Int J Crit Illn Inj Sci 3(1): 64-68.
-
Eriksson EA, Schultz SE, Cohle SD, Post KW (2011) Cerebral fat embolism without intracardiac shunt: A novel presentation. J Emerg Trauma Shock 4(2): 309- 312.
-
Saigal R, Mittal M, Kansal A, Singh Y, Kolar PR, et al. (2008) Fat Embolism Syndrome. J Assoc Physicians India 56: 245-249.
-
Font MO, Nadal P, Bertran A (1989) Fat embolism syndrome with no evidence of pulmonary involvement. Crit Care Med 17(1): 108-109.
-
Nentwich MM, Remy M, Schaller UC (2011) Ocular fat embolism syndrome. Int Ophthalmol 31(1): 15-16.
-
Awad AM, Estephan B, Warnack W, Stuve O (2009) Optic neuritis presenting with amaurosis fugax. J Neurol 256(12): 2100-2103.
-
Pula JH, Kwan K, Yuen CA, Kattah JC (2016) Update on the evaluation of transient vision loss. Clin Ophthalmol 10: 297-303.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index