A Rare Case of Factor V Deficiency Presenting as Recurrent Hemorrhagic Ovarian Mass and Hemoperitoneum
Factor V (FV) deficiency is an extremely rare bleeding disorder due to genetic or acquired causes, presenting as mucosal or unexpected postoperative bleeding. The following case narrates a woman with FV deficiency presenting with recurrent hemorrhagic ovarian mass and hemoperitoneum. She presented as an acute abdomen with deranged coagulation parameters. The bleeding in her case was probably because of ruptured corpus luteum due to ovulation. She was successfully managed conservatively with RBC / FFP transfusions, tranexamic acid along with COC - combined oral contraceptive pills with an advice to continue COC without stopping.
Introduction
Factor V deficiency is an extremely rare bleeding disorder with around 200 cases reported so far. The condition commonly presents as recurrent mucosal bleeding or post-operative bleeding. Severe or life threatening bleeding manifestations are relatively rare (in contrast to Hemophilia). In our case, we had a patient who presented with hemorrhagic ovarian mass, hemoperitoneum for second time. She was conservatively managed with RBC/ FFP transfusions. The peculiarity in our case is the severity of presentation, which responded well to transfusions and conservative treatment. The whole episode was precipitated by inadvertent stopping of COC pills by the patient, return of ovulation and probable corpus luteum rupture.
Case Description
An Indian female of 30+ age was admitted to ICU with H/O of giddiness, abdominal pain of 1 day duration. She was a proven case of FV deficiency (Owrens disease). She was born to healthy, non-consanguineous parents with no known bleeding complications in the family. She attained menarche at 13 years of age with previous regular cycles. She was a nulligravida. She was diagnosed to have FV deficiency at 22 years age, when she had recurrent mucosal bleedings. She developed hemorrhagic ovarian mass, hemoperitoneum, 5 years ago which was managed conservatively elsewhere, with supportive care and transfusions. She was started on oral contraceptive pills. However, the patient has poor compliance history with COC and she discontinued the drugs by herself. On admission, patient weighed 54 kg. Clinical examination revealed severe pallor with no cyanosis, icterus, lymphadenopathy, pedal edema or fever. She had a HR – 120/ min, BP – 110/70 (both arms), oxygen saturation – 98% (RA), RR – 20/min, with unremarkable cardiac, respiratory and neurological examination. Abdomen was soft with diffuse tenderness, without rigidity or rebound.
Investigations
Hb – 4.6 g/dl PCV – 19 % TC – 11,300 / mm3 Platelets – 3,12,000 / mm3 RBS – 151 mg/dl Urea – 28 mg/dl Creatinine – 0.6 mg/dl Na – 135; K – 4.4 mEq/L T.Bilirubin – 1.2 ; DB – 0.3 ; IDB – 0.9 mg/dl T. protein – 6.9 g/dl, Albumin – 4.2 g/dl GGTP – 17, SAP – 127 IU/L PT > 100s, INR > 10. aPTT – T – 30.7, C – 25 CXR had clear lung fields and ECG showed Sinus rhythm, No ST-T changes, ECHO – EF -67%, No RWMA.
Iron studies showed low serum iron, ferritin and increased TIBC levels, suggestive of iron deficiency anemia (Figure 1).
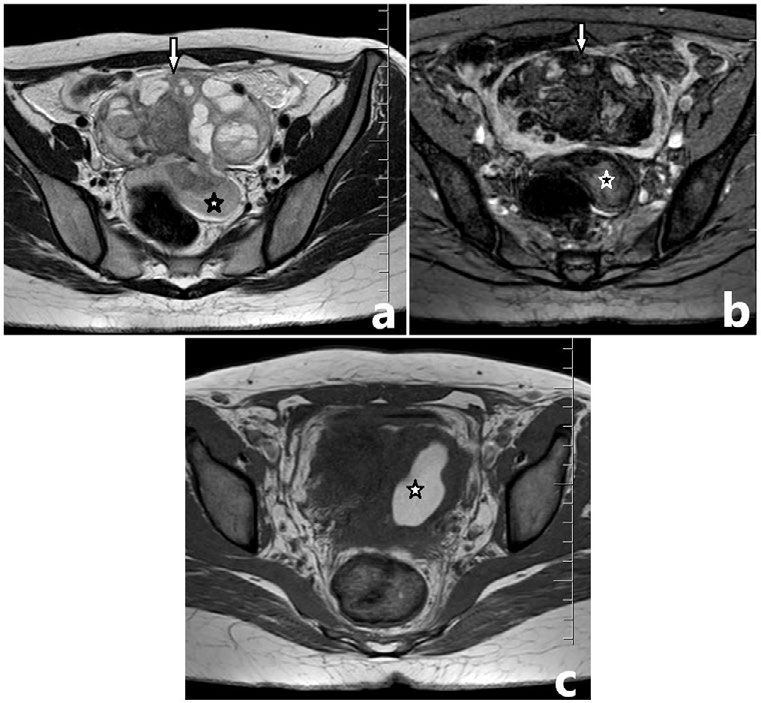
MRI abdomen / Pelvis showed complex cystic, intraperitoneal SOL in pelvis (6x9.6x6 cm); both the ovaries were involved in the lesion and could not be seen separately. The fluid component of the cyst was profoundly hypointense in GRE images suggesting blood degradation products.
Associated hematometra and hemoperitoneum seen. There was an interval decrease in size of the lesion when compared with prior CT done 5 years ago. These features were suggestive of a benign hemorrhagic cyst.
Treatment
She was transfused with 4 units each of packed red blood cells and fresh frozen plasma. Intravenous tranexamic acid 500 mg 8 hourly was given along with other supportive care. Fluid and electrolyte balance maintained. Her Hb improved to 8.8 g/dl and coagulation parameters normalized. She was discharged in a stable state with advice to continue iron supplements, iron rich food along with oral contraceptive pills and review instructions after 1 month.
Discussion
Factor V (Proaccelerin / labile factor) is a plasma cofactor for prothrombinase complex that activates prothrombin to thrombin. FV deficiency can be caused by FV gene mutation (AR) or acquired causes (malignancy, rheumatological disorders, antibiotic use – beta lactams, topical bovine thrombin etc) [1]. Since FV is present in platelet alpha granules as well as plasma, low FV levels are found in disorders of platelet granules also [2, 3]. Generally, FV deficient patients express less severe phenotype than Hemophilia A or B. The most common presenting symptoms are bleeding from mucosal surfaces and post-operative hemorrhage. Rarely, intra-muscular, intra-cranial bleeds happen. Patients can also present with severe menorrhagia [4, 5, 6].
FV deficiency commonly presents before 5-6 years of age with minor mucosal bleedings. However, a case report of 62 years old patient presenting with ICH has been reported [6]. Labs show prolonged PT, PTT and low FV levels. Differentials include consumptive Coagulopathy, liver disease, and combined FV and FVIII deficiencies. Treatment of FV deficiency involves FFP (mainstay treatment) and anti- fibrinolytics, as isolated FV replacement is not available. Refractory cases or patients with acquired inhibitors require prothrombin complex concentrates, activated Factor VIIa, platelet transfusions along with steroids or immunosuppressives in severe cases [6].
In our case, the cause for this presentation is most likely from a ruptured, bleeding corpus luteum following ovulation. This is her second admission with a similar presentation of acute abdomen. While the patient was put on COC (combined oral contraceptive pill), she was not made aware of the importance of being on the pill continually, cessation of which brought back ovulatory cycles and hence the presentation. The patient’s poor compliance with COC
is the probable cause of recurrent hemoperitoneum. The patient has been put on the COC with strict advice as not to stop without medical input
Conclusion
FV deficiency is a rare bleeding disorder which is suspected in patients with prolonged PT, PTT with mild, recurrent mucosal bleedings, when other causes are ruled out. The diagnosis is clinched by demonstrating low factor V levels. This case is published in view of rarity of diagnosis as well as atypical presentation of bleeding complication. The patient discontinued COC pills inadvertently, which resulted in menorrhagia, iron deficiency anemia, return of ovulation and probable corpus luteum rupture. This highlights the need for educating a patient about their own condition, importance of drug compliance, so as to not to land up recurrently in life threatening situation as was in our case.
References
-
Huang JN, Koerper MA (2008) Factor V deficiency: a concise review. Haemophilia 14(6): 1164-1169.
-
Kalafatis M (2005) Coagulation factor V: a plethora of anticoagulant molecules. Curr Opin Hematol 12(2): 141- 148.
-
Asselta R, Tenchini ML, Duga S (2006) Inherited defects of coagulation factor V: the hemorrhagic side. J Thromb Haemost 4(1): 26-34
-
Lak M, Sharifan R, Peyvandi F, Mannucci PM (1998) Symptoms of inherited factor V deficiency in 35 Iranian patients. Br J Haematol 103(4): 1067-1069.
-
Mannuci PM, Duga S, Peyvandi F (204) Recessively inherited coagulation disorders. Blood 104(5): 1243- 1252.
-
Acharya SS, Coughlin A, DiMichele DM (2004) Rare Bleeding Disorder Registry: deficiencies of factors II, V, VII, X, XIII, fibrinogen and dysfibrinogenemias. J Thromb Haemost 2(2): 248-256.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index