Effect of Alkalinization on the Onset Action of Lignocaine in Epidural Anaesthesia
Lumbar epidural anaesthesia is one among the commonly performed regional anaesthesia especially for lower abdominal, lower limb surgeries and also for post-operative pain relief. Its ability to produce neuraxial blockade without dural puncture is an attractive option for spinal anaesthesia. To study the effect of alkalinization on the onset action of lignocaine in epidural anaesthesia. This study was done in Shaheed Ziaur Rahman Medical College & Hospital, Bogura, Bangladesh in the year of 2018-19. After the institutional ethical committee approval and informed consent from the patient, 100 patients posted for lower abdominal surgery were selected after inclusion and exclusion criteria. The inclusion criteria were ASA I&II of both gender with an age group of 20-60 years and the exclusion criteria were age below 20 years and above 60 years, weight 45 to 85 kgs, spinal deformities, local sepsis, bleeding disorder and patient refusal. After the institutional ethical committee approval and informed consent from the patient, 100 patients posted for lower abdominal surgery were selected after inclusion and exclusion criteria and they were divided into two groups. Group S received Lignocaine with adrenaline added with Saline and Group A received alkalized Lignocaine (with Sodium bicarbonate) with adrenaline. It was concluded that alkalinization shortens the onset of action of Lignocaine.
Introduction
Lumbar epidural anaesthesia is one among the commonly performed regional anaesthesia especially for lower abdominal, lower limb surgeries and also for post-operative pain relief. Its ability to produce neuraxial blockade without dural puncture is an attractive option for spinal anaesthesia [1, 2, 3, 4, 5]. Neural blockade follows when a local anesthetic is deposited in the vicinity of a nerve fiber.
The onset of blockade occurs when the local anesthetic molecules reach the interior of the axoplasm in sufficient quantity. The drug molecule to reach the site of action, it has to travel many barriers especially in epidural anesthesia and so, the onset of action is delayed [6]. By modifying the physicochemical properties, we can quicken the onset of action of local anesthetic. Sodium bicarbonate is one such adjuvant that alters the same.
Aim of the study
To compare the effect of alkalinization on the onset of action of alkalized and non-alkalized Lignocaine.
Materials And Methods
This study was done in Shaheed Ziaur Rahman Medical College & Hospital, Bogura, Bangladesh in the year of 2018- 19. After the institutional ethical committee approval and informed consent from the patient, 100 patients posted for lower abdominal surgery were selected after inclusion and exclusion criteria. The inclusion criteria were ASA I&II of both gender with an age group of 20-60 years and the exclusion criteria were age below 20years and above 60years, weight 45 to 85 kgs, spinal deformities, local sepsis, bleeding disorder and patient refusal. The patients were divided into two groups. Group(S) received Lignocaine with adrenaline added with Saline and Group (A) received alkalized Lignocaine (with Sodium bicarbonate) with adrenaline. Epidural block performed with 18-G Tuohy’s epidural needle in L3–L4 interspace by loss of resistance technique. Test dose of 3 ml of 2% lignocaine with adrenaline was injected followed by study drug 3 min later. Immediately after the injection, patients were placed in supine position.
All patients were monitored for the onset of anesthesia, effects on cardiovascular and respiratory parameters, and intra- and post-operative complications. Pulse rate, mean blood pressure, and SPO2 recorded after injection of local anesthetic at interval of 5, 15, 30, 60, 90, 120, and 150 min and more than 20% change as compared to preoperative values was considered significant.
Onset of sensory analgesia
Time from administration of drug to the time required for loss of touch sensation for an alcohol swab and loss of pinprick sensation at L2 level, which was judged at 1 min interval.
Method of alkalinization
0.8 ml of 8.4% Sodium bicarbonate was added with each 10 ml of 2% Lignocaine with the total of 20 ml. After the epidural space identification, the patients received the following drugs according to the group. All cases completed in stipulated time. Data were collected, compiled, and tabulated. All results were expressed as mean ± standard deviation. Two according to the drug received. The observations in the study are given as follows. Demographic Data; There was not much significant variance in the each group.
Results
This study was a randomized double blind study, conducted on a total of 100 patients grouped into two according to the drug received. The observations in the study are given as follows. In group N, the lowest onset time was 5 minutes and longest onset was 14 minutes with a mean of 7.87±1.834 (standard deviation). In group A, the, lowest onset of time was 1 minute and longest onset of time was 5 minutes with a mean of 2.665± 0.994(standard deviation).
| Group (S) | Group (A) |
|---|---|
| 2% Lignocaine-18.4 ml | 2% Lignocaine -18.4 ml |
| Adrenaline -05mcg/ml | Adrenaline-05mcg/ml |
| Normal saline -1.6 ml | 8.4% Sodium bicarbonate -1.6 ml |
Table 1: Chart with weight distribution (kgs).
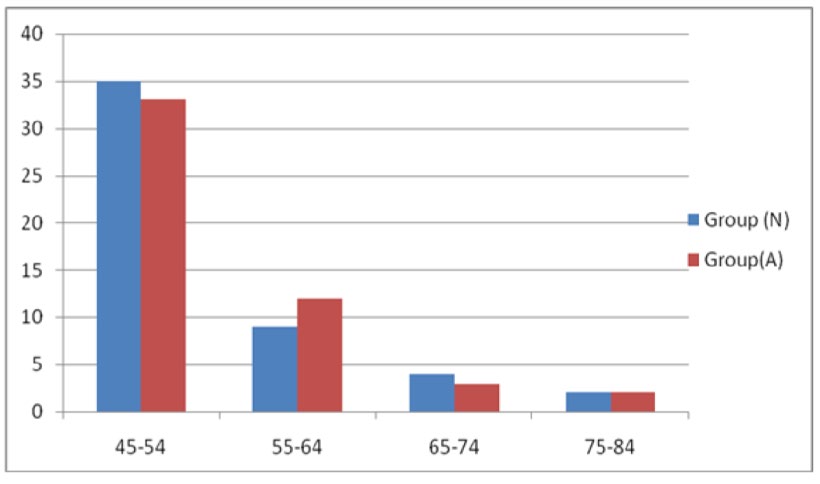
Figure1: Number of patients in left axis and weight in kg in right axis.
| Minutes | Group(N) | Group(A) |
|---|---|---|
| 0-2 | - | 24 |
| 02-Apr | - | 24 |
| 04-Jun | 13 | 2 |
| 06-Aug | 24 | - |
| 08-Oct | 9 | - |
| 10-Dec | 2 | - |
| Total number | 50 | 50 |
Table 2: The Onset of Action in Minutes (N=100).
Discussion
The pH of the local anesthetic solutionimmediately before injection to raise the pH. This is called alkalinization of the solution. Anesthetic activity is dependent on having both the ionized and nonionized forms of the drug present after injection. Alkalinization increases the proportion of non- ionized drug and this could be advantageous. Care must be taken, because if too much alkali is added and mixing of any other drug, the local anesthetic will get precipitated. Local anesthetics are the basic drugs which have a pKa close to the normal extracellular pH of 7.4, for example lignocaine has a pKa of 7.8. The drugs exist in two forms in the solution – the uncharged basic form (B) and the charged form (BH). B + H+ ↔ BH. The importance of the pKa-pH relationship is that this knowledge allows the calculation of the relative amounts of these two forms. When the pH is equal to the drug’s pKa, 50% of the drug is in the uncharged form, and 50% is in the charged form. In acidic solutions, most of the drug will be in the charged form. When injected, the local anesthetic solution must be present in the tissues in both forms.
The reason is that the drug has to diffuse to the site of action across several tissue barriers. The uncharged lipid- soluble form will diffuse across lipid barriers, for example, perineural sheath, or cell membrane. The charged water soluble form will diffuse across tissue fluid barriers, for example interstitial fluid. The site of action of the local anesthetic molecule is the inner (or cytoplasmic) end of the sodium channel in the cell membrane. The final pathway for all injected local anesthetics is to diffuse to the cell membrane (in the charged form) then equilibrate to form both charged and uncharged forms adjacent to the outside of the nerve cell membrane. The molecules diffuse across the nerve cell membrane in the uncharged form then re-equilibrate in the cytoplasm to have both forms present again. Next the charged form diffuses to and binds to its receptor on the inside of the Trans membrane sodium channel.
This binding results in a conformational change in the channel protein to block the passage of sodium ions into the cell in response to a subsequent action potential. Onset of sensory block was significantly quicker in alkalized group. Our observation was similar to observation by many authors [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12]. Addition of bicarbonate for increasing pH of local anesthetic in epidural blockade hastens the onset of action by increasing the pH of the solution and thereby it increases the uncharged base form available for penetration. Our result is similar to Aparna Abhijit Bagle, et al. [1]. For epidural anaesthesia, time to achieve surgical anaesthesia is important. Onset of epidural anaesthesia was quicker with alkalized local anaesthetic solutions, but only by a few minutes. Dr.P.Chalapathy, et al. concluded alkalinized lignocaine hydrochloride solution provides a significant advantage over non alkalinized lignocaine hydrochloride in terms of quicker onset, duration and quality of block [12]. Cardiovascular stability was found in all groups which is the feature of epidural analgesia and there was no incidence of postoperative complications in any of the group in our study.
Conclusion
It was concluded that alkalinization shortens the onset of action of Lignocaine. We conclude that pH-adjusted 1% lidocaine offers the advantage of a more rapid onset of sensory blockade, while motor blockade and the distribution of anesthesia are unaffected by pH change in epidural anesthesia.
References
-
Aparna Abhijit Bagle, Satish Deshpande, Nagnath L Garthe (2016) Effect of increase in pH of local anaesthetics on quality of epidural anesthesia 2(2).
-
Capogna G, Celleno D, Costantino P, Muratori F, Sebastiani M, et al. (1993) Alkalinization improves the quality of lidocaine-fentanyl epidural anaesthesia for Caesarean section. Can J of Anaesth 40(5): 425-430.
-
Gosteli P, Van Gessel E, Gamulin Z (1995) Effects of pH adjustment and carbonation of lidocaine during epidural anesthesia for foot or ankle surgery. Anesth Analg 81(1): 104-109.
-
Milner QJ, Guard BC, Allen JG (2000) Alkalinization of amide local anaesthetics by addition of 1% sodium bicarbonate solution. Eur J Anaesthesiol 17(1): 38-42.
-
Fulling PD, Peterfreund RA (2000) Alkalinization and precipitation characteristics of 0.2% ropivacaine. Reg Anesth 25(5): 518-521.
-
Robinson J, Fernando R, Sun Wai WY, Reynolds F (2000) Chemical stability of bupivacaine, lidocaine and epinephrine in pH-adjusted solutions. Anaesthesia 55(9): 853-858.
-
Tackley RM, Coe AJ (1988) Alkalinised bupivacaine and adrenaline for epidural Caesarean section: A comparison with 0.5% bupivacaine. Anaesthesia 43(12): 1019-1021.
-
Kaufman JJ, Semo NM, Koski WS (1975) Microelectrometric titration measurement of the pKa’s and partition and drug distribution coefficients of narcotics and narcotic antagonists and their pH and temperature dependence. J Med Chem 18(7): 647-655.
-
Benhamou D, Perrachon N, Labaille T, Bonhomme L (1989) Alkalinization of epidural 0.5% bupivacaine for cesarean section. Reg Anesth 14(5): 240-243.
-
Parnass SM, Curran MJ, Becker GL (1987) Incidence of hypotension associated with epidural anesthesia using alkalinized and nonalkalinized lidocaine for cesarean section. Anesth analg 66(11): 1148-1150.
-
Chalapathy P, Sangeetha Rao D (2016) Comparitive Study of The Effect of Lignocaine Hydrochloride With Adrenaline And It’s Combination With Alkali Solution on Supraclavicular Brachial Plexus Block.
-
Mehta R (2014) Effect of alkalinization of lignocaine hydrochloride on brachial plexus block.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index