Ventilatory Support Used as the First Choice in Critically Ill Children in a Pediatric Intensive Care Unit
Objective: To evaluate the different types of ventilatory supports used in critically ill children with respiratory failure in relation to therapeutic success and length of stay in the intensive care unit (ICU). Hypothesis: Late orotracheal intubation is associated with prolonged ICU stay. Methods: Retrospective, single-center cohort study with patients between 1 month and 18 years old with respiratory failure admitted to the ICU of a reference hospital in Brazil during the period of 1 year. Patients from other hospitals were excluded. The sample was divided into 5 types of ventilatory support used in the admission. The main outcome is prolonged ICU stay. Results: One hundred and seventy-five children participated in the study, male = 53%, mean length of stay = 13, 7 days and overall mortality = 7,4%. In decreasing order of frequency, 52 children (30%) underwent orotracheal intubation; 49 patients (28%) used non-invasive mechanical ventilation; 33 patients (19%) used complementary oxygen; 31 children (18%) had tracheostomy; and 10 patients (5%) used a high-flow nasal cannula. Only 52,5% of the patients who used noninvasive ventilatory support showed therapeutic success. Late orotracheal intubation was associated with prolonged ICU stay (p = 0,05). Neurological disease was characterized as an independent marker of prolonged ICU stay (p= 0,03). Conclusion: Invasive ventilatory support via endotracheal tube was the most used ventilatory support in the sample studied and the delay in this procedure was statistically associated with prolonged ICU stay.
Introduction
Acute respiratory insufficiency is the inability to provide oxygen to tissues, eliminate carbon dioxide or both. It’s a common cause of admission to the intensive care unit (ICU) [1]. The etiology can be multifactorial and it may involve neurological dysfunction, impairment of the respiratory muscles, airways or lung parenchyma [2]. Depending on the severity, many respiratory support therapies can be used, from increased oxygen supply to invasive mechanical ventilation [3].
Several studies were performed in order to identify the best ventilatory support strategies in critically ill adult patients. Ferrer, et al. identified that patients undergoing non-invasive mechanical ventilation (NIV) had a lower risk of orotracheal intubation (OI) when compared to patients who used only complementary oxygen (p: 0,025) [4]. Sztrymf, et al. reported that the high-flow nasal cannula (HFNC) is associated with improvement in hemodynamic instability after a few minutes of using the device [5]. Other studies suggest that the failure of the non-invasive ventilatory support modality and the delay in or tracheal intubation are associated with increased mortality rates [6, 7].
In pediatrics, besides the results being controversial, there are few studies evaluating the different types of ventilatory supports used in the ICU admission, the rate of therapeutic success and its impact on the length of stay. Our hypothesis is that invasive mechanical ventilation via endotracheal cannula is the most widely used support for the admission of severe pediatric patients with respiratory failure and the delay in this procedure is associated with prolonged ICU stay.
The aim of this study is to evaluate the different ventilatory supports used in critically ill children with respiratory insufficiency in relation to the risk of therapeutic failure and length of stay in the pediatric intensive care unit.
Methodology
This is a retrospective, single-center cohort study with all patients admitted to the pediatric ICU of a pediatric referral hospital in Brazil in 2019. The data were extracted from the unit’s electronic medical records and the study was approved by the institution’s Research Ethics Committee.
Inclusion criteria were patients between 1 month and 18 years of age with respiratory failure due to upper, intermediate or lower respiratory tract involvement. All patients underwent chest radiography and the images were correlated with signs and symptoms. Respiratory insufficiency was defined as the need for inspiratory oxygen fraction ≥ 40% to maintain oxygenation saturation ≥ 92% and / or the presence of carbon dioxide blood pressure ≥ 50mmHg. Children from other hospitals or admitted to the ICU with respiratory failure of another etiology were excluded.
The patients were divided into 5 different types of ventilatory supports used in the first 24 hours of admission to the ICU: complementary oxygen (O2); noninvasive ventilatory support via high flow nasal cannula (HFNC) or noninvasive mechanical ventilation (NIV); and invasive ventilatory support via orotracheal intubation (IO) or tracheostomy cannula. Those who required only oxygen in the first 24 hours of admission were classified as O2. Children who were admitted using complementary oxygen, but needed HFNC, NIV or IO were included in their respective groups. Tracheostomized patients (TP) were connected to invasive ventilatory support. The type of ventilatory support and ventilatory parameters were decided by the intensive care physician through physical examination and laboratory tests.
Complementary oxygen was used via nasal catheter and Venturi mask. HFNC was from Vapotherm, with a flow emission, air humidification and gas mixture through blender, in addition to a temperature adjusted to 37º Celsius. NIV was used with nasal prongs or nasofacial mask interfaces through the modes continuous positive airway pressure (CPAP) or positive pressure at two levels (BIPAP). A nasogastric tube was used in patients using non-invasive ventilatory support and very agitated children received low-dose benzodiazepine sedative. The IO was performed with the aid of the institution’s rapid sequence intubation protocol with opioid analgesic, benzodiazepine sedative and depolarizing neuromuscular blocker. The ventilators used for invasive and non-invasive mechanical ventilation were Servo-s from Maquet or BennettTM 840 from Medtronic.
The main outcome of the study was prolonged ICU stay, defined as length of stay ≥ 15 days. Secondary outcomes were therapeutic failure of ventilatory support and death. Late orotracheal intubation was defined if the procedure was performed 24 hours after admission to the ICU.
Other variables included were age, genre, pediatric mortality risk score 2 (PRISM2), disease and comorbidities. Patients admitted for respiratory malformation included children diagnosed with laryngomalacia, tracheomalacia, tracheal stenosis, tracheoesophageal fistula or nasofacial deformity. Patients with chronic pneumopathy included those with a previous diagnosis of cystic fibrosis or bronchodysplasia. For statistical analysis, we used Epi InfoTM Windows 7.2 and Microsoft® Office Excel 2017. Frequencies and proportions of categorical variables were calculated. We evaluated the mean, standard deviation, median, quartiles (p25% - p75%), minimum and maximum values of quantitative variables. Bivariate analyzes were performed using the chi-square and Fisher’s exact tests, with Odds Ratio (OR) calculation, significance level of 5% (p ≤ 0,05) and 95% Confidence Interval (95% CI). Variables that were associated with the outcomes of interest (p ≤ 0,15) were used in the multivariate logistic regression analysis.
Results
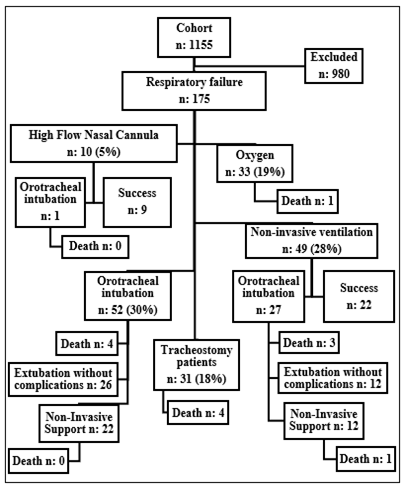
The cohort of patients admitted to the ICU during the analyzed period was 1155, with 175 children fulfilling the inclusion and exclusion criteria. In decreasing order of frequency, 52 children (30%) were submitted to IO; 49 patients (28%) used NIV; 33 patients (19%) needed complementary oxygen; 31 children (18%) had a tracheostomy; and 10 patients (5%) used HFNC (Figure 1). In general, 53% of the sample was male with a median age of 2 years and a mortality rate expectation of 1,9% by the PRISM2 score. In decreasing order of frequency, 47,4% of patients were admitted to the ICU for pneumonia, 17,1% asthmatic crisis, 13,7% viral bronchiolitis, 13,1% malformation of the respiratory tract, 5,1% acute edema of lung and 4% laryngitis. We noticed that three quarters of the sample had at least 1 associated comorbidity, with 50,8% of patients presenting neuropathy, 22,8% heart disease, 14,8% chronic lung disease, 11,4% nephropathy, 8% malformation of the gastrointestinal tract, 6,8% endocrinopathy, 4,5% hematological-oncological disease and 3,4% immunodeficiency.
The mean length of stay in the ICU was 13,7 days and the overall mortality was 7,4% (Table 1). Among the 59 patients who used noninvasive ventilatory support (NIV + HFNC) in the first 24 hours of hospitalization, 28 (47,4%) children had therapeutic failure and underwent late OI, 27 patients from the NIV group and 1 patient from the HFNC group (p = 0,009). Among patients who failed NIV, the median time of use of the device was 1 day with a minimum of 1 day and a maximum of 15 days, while the only patient who failed HFNC used the device for 8 days. Patients undergoing late OI showed statistically significant association with the prolonged length of stay in the ICU when compared to patients who were intubated early (p = 0,05) (Table 2). Among the patients with tracheostomy, twenty-two children were responsible for the 31 admissions in this group, 5 children were readmitted once and 2 children were readmitted twice during the analyzed period. The main comorbidity identified in this group was neuropathy (83,8%) and the main cause of admission was pneumonia (71%). Use of complementary oxygen was identified as a protective factor for prolonged ICU stay (p = 0,008). When the other ventilatory supports were compared to NIV, there was no statistically significant association with prolonged ICU stay. Neurological / neuromuscular comorbidity was the only independent marker of prolonged ICU stay (p = 0,03) (Tables 3 and 4).
Among the patients who died, 1 patient was in the O2 group, however he was in “do-not-intubate-status” because he had cancer disease with poor prognosis; 4 patients had tracheostomy; 4 patients underwent orotracheal intubation at admission; and 4 children used non-invasive ventilation. There were no deaths in the HFNC group.
| O2 (%) | HFNC (%) | NIV (%) | OI (%) | TP (%) | General (%) | |
|---|---|---|---|---|---|---|
| Male | 16 (48,4) | 7 (70) | 22(44,9) | 30 (57,6) | 17 (54,8) | 93 (53,1) |
| Age (years)a | 4 (1-7,5) | 0 (0-1,5) | 1 (0-6) | 1 (0-6) | 3 (1-13) | 2 (0-6) |
| Comorbidities | ||||||
| Neuropathy | 7 (21,2) | 3 (30) | 23(46,9) | 30 (57,7) | 26 (83,8) | 89 (51,7) |
| Heart disease | 8 (24,2) | 3 (30) | 5 (10,2) | 12 (23) | 12 (38,7) | 40 (22,8) |
| Pneumopathy | 5 (15,1) | 1 (10) | 9 (18,3) | 6 (11,5) | 5 (16,1) | 26 (14,8) |
| Nephropathy / uropathy | 3 (9) | 0 (0) | 2 (4) | 8 (15,3) | 7 (22,5) | 20 (11,4) |
| GT malformation | 3 (9) | 0 (0) | 2 (4) | 5 (9,6) | 4 (12,9) | 14 (8) |
| Endocrinopathy | 2 (6) | 0 (0) | 1 (2) | 4 (7,7) | 5 (16,1) | 12 (6,8) |
| Hematologicaldisease | 2 (6) | 0 (0) | 4 (8,1) | 2 (3,8) | 0 (0) | 8 (4,5) |
| Immunodeficiency | 1 (3) | 0 (0) | 1 (2) | 3 (5,7) | 1 (3,2) | 6 (3,4) |
| 16 (48,4) | 4 (40) | 15(30,6) | 13 (25) | 1 (3,2) | 49 (28) | |
| ≥1 comorbidity | 17 (51,5) | 6 (60) | 34(69,3) | 39 (75) | 30 (96,7) | 126 (72) |
| ≥2 comorbidities | 10 (30,3) | 1 (10) | 12(24,5) | 21 (40,3) | 18 (58) | 62 (35,4) |
| Reason for admission | ||||||
| Asthma / bronchospasm | 7 (21,2) | 1 (10) | 12(24,4) | 7 (13,4) | 3 (9,6) | 30 (17,1) |
| Bronchiolitis | 8 (24,2) | 3 (30) | 8 (16,3) | 3 (5,7) | 2 (6,4) | 24 (13,7) |
| Pneumonia | 13 (39,4) | 6 (60) | 21(42,8) | 20 (38,4) | 22 (71) | 82 (46,8) |
| Acute lung edema | 2 (6) | 0 (0) | 1 (2) | 6(11,5) | 0 (0) | 9 (5,1) |
| Laryngitis | 1 (3) | 0 (0) | 3 (6,1) | 3 (5,7) | 0 (0) | 7 (4) |
| Respiratory malformation | 2 (6) | 0 (0) | 4 (8,1) | 13 (25) | 4 (12,9) | 23(13,1) |
| PRISM2a | 1,5 (1,4-3,1) | 1,5 (1,3-2,6) | 2,3(1,34,2) | 2 (1,3-4,9) | 2,3 (1,9-4,2) | 1,9 (1,5-4,2) |
| ICU stay (days)a | 3 (2,5-4,5) | 8 (6,5-12) | 10,5(617,5) | 11 (6-21) | 11 (6-22) | 9 (4-17) |
| Death | 1 (3) | 0 (0) | 4 (8,1) | 4 (7,6) | 4 (12,9) | 13 (7,4) |
| Total | 33 | 10 | 49 | 52 | 31 | 175 |
Table 1: ** Demographic profile, clinical characteristics and outcomes in the studied sample (n:175).
O2: complementary oxygen; HFNC: high flow nasal cannula; NIV: non-invasive ventilation; OI: orotracheal intubation; TP: tracheostomy patient; GT: gastrointestinal tract; PRISM2: pediatric risk of mortality 2; ICU: intensive care unit. a Numerical variables expressed as median (p25% -p75%). Table 1: Demographic profile, clinical characteristics and outcomes in the studied sample (n:175).
| Late OI (%) | Early OI (%) | Geral | p | |
|---|---|---|---|---|
| Male | 11 (39,3) | 30 (57,7) | 41 | 0,11 |
| Age | ||||
| Infant | 15 (53,6) | 28 (53,8) | 43 | - |
| Preschool | 5 (17,9) | 6 (11,5) | 11 | 0,51 |
| School | 3 (10,7) | 8 (15,4) | 11 | 0,63 |
| Teenager | 5 (17,9) | 10 (19,2) | 15 | 0,91 |
| Neuropathy | 15 (53,6) | 30 (57,7) | 45 | 0,72 |
| Heart disease | 4 (14,3) | 12 (23,1) | 16 | 0,34 |
| Pneumopathy | 7 (25) | 6 (11,5) | 13 | 0,11 |
| Nephropathy / uropathy | 0 (0) | 8 (15,4) | 8 | 0,028 |
| GT malformation | 2 (7,1) | 5 (9,6) | 7 | 0,7 |
| Endocrinopathy | 1 (3,6) | 4 (7,7) | 5 | 0,46 |
| Hematologicaldisease | 2 (7,1) | 2 (3,8) | 4 | 0,51 |
| Immunodeficiency | 1 (3,6) | 3 (5,8) | 4 | 0,66 |
| ≥1 comorbidity | 23 (82,1) | 39 (75) | 62 | 0,46 |
| ≥2 comorbidities | 10 (35,7) | 21 (40,4) | 31 | 0,68 |
| Reason for admission | ||||
| Asthma / Bronchospasm | 5 (17,9) | 7 (13,5) | 12 | - |
| Bronchiolitis | 5 (17,9) | 3 (5,8) | 8 | 0,64 |
| Pneumonia | 14 (50) | 20 (38,5) | 34 | 0,97 |
| Acutelung edema | 1 (3,6) | 6 (11,5) | 7 | 0,33 |
| Laryngitis | 1 (3,6) | 3 (5,8) | 4 | 1 |
| Respiratory malformation | 2 (7,1) | 13 (25) | 15 | 0,18 |
| PRISM2 ≥ 5% | 8 (28,6) | 20 (38,5) | 28 | 0,37 |
| Length of stay ≥ 15 days | 16 (57,1) | 18 (34,6) | 34 | 0,05 |
| Death | 4 (14,3) | 4 (7,7) | 8 | 0,34 |
| Total | 28 | 52 | 80 |
Table 2: Association between late and early orotracheal intubation with clinical-demographic variables (n: 80).
OI: orotracheal intubation; GT: gastrointestinal tract; PRISM2: pediatric risk of mortality 2. Table 2: Association between late and early orotracheal intubation with clinical-demographic variables (n: 80).
| Variables | ≥ 15 days(%) | < 15days (%) | Total | p |
|---|---|---|---|---|
| Male | 25 (26,9) | 67 (73,1) | 92 | 0,66 |
| Age | ||||
| Infant | 23 (26,4) | 64 (73,6) | 88 | - |
| Preschool | 8 (28,6) | 20 (71,4) | 28 | 0,82 |
| School | 7 (24,1) | 22 (75,9) | 28 | 0,8 |
| Teenager | 12 (38,7) | 19 (61,3) | 31 | 0,19 |
| Neuropathy | 36 (40,4) | 53 (59,6) | 89 | <0,001 |
| Heart disease | 9 (22,5) | 31 (77,5) | 40 | 0,33 |
| Pneumopathy | 10 (38,5) | 16 (61,5) | 26 | 0,22 |
| Nephropathy / uropathy | 6 (30) | 14 (70) | 20 | 0,88 |
| GT malformation | 7 (50) | 7 (50) | 14 | 0,06 |
| Endocrinopathy | 4 (33,3) | 8 (66,7) | 12 | 0,7 |
| Hematologicaldisease | 3 (37,5) | 5 (62,5) | 8 | 0,56 |
| Immunodeficiency | 3 (50) | 3 (50) | 6 | 0,23 |
| ≥1 comorbidity | 44 (34,9) | 82 (65,1) | 126 | 0,002 |
| ≥2 comorbidities | 27 (43,5) | 35 (56,5) | 62 | 0,001 |
| Reason for admission | ||||
| Asthma / Bronchospasm | 12 (40) | 18 (60) | 30 | - |
| Bronchiolitis | 4 (16,7) | 20 (83,3) | 24 | 0,06 |
| Pneumonia | 21 (25,6) | 61 (74,4) | 82 | 0,14 |
| Acutelung edema | 4 (44,4) | 5 (55,6) | 9 | 1 |
| Laryngitis | 0 (0) | 7 (100) | 7 | 0,11 |
| Respiratory malformation | 9 (39,1) | 14 (60,9) | 23 | 0,94 |
| PRISM2≥5% | 13 (28,9) | 32 (71,1) | 45 | 0,95 |
| Ventilatory Support | ||||
| NIV | 17 (34,7) | 32 (65,3) | 49 | - |
| O2 | 2 (6) | 31 (94) | 33 | 0,002 |
| HFNC | 1 (10) | 9 (90) | 10 | 0,12 |
| OI | 18 (34,6) | 34 (65,4) | 52 | 0,99 |
| TP | 12 (38,7) | 19 (61,3) | 31 | 0,71 |
| Total | 50 | 125 | 175 |
Table 3: Association between clinical-demographic variables and prolonged ICU stay (n: 175).
ICU: intensive care unit; GT: gastrointestinal tract; PRISM2: pediatric risk of mortality 2; NIV: non-invasive ventilation; O2: complementary oxygen; HFNC: high flow nasal cannula; OI: orotracheal intubation; TP: tracheostomy patient. Table 3: Association between clinical-demographic variables and prolonged ICU stay (n: 175).
| Variables | OR (95%CI) | p | Coefficient |
|---|---|---|---|
| Neuropathy | 4,5 (1,13 – 18,1) | 0,03 | 15,135 |
| GT malformation | 5,15 (0,92 – 28,7) | 0,06 | 16,398 |
| ≥1 comorbidity | 0,84 (0,16 – 4,22) | 0,83 | - 0,1738 |
| ≥2 comorbidities | 1,54 (0,64 – 3,72) | 0,32 | 0,4362 |
| Bronchiolitis | 0,7 (0,15 – 3,13) | 0,64 | - 0,3566 |
| Pneumonia | 0,53 (0,23 – 1,21) | 0,13 | - 0,5268 |
| Laryngitis | 0 (0, >1.0E12) | 0,96 | -1,36,022 |
| O2 | 0,1 (0,02- 0,56) | 0,008 | -18,309 |
| HFNC | 0,27 (0,04 – 2,55) | 0,25 | -12,906 |
Table 4: Multivariate logistic regression to rule out possible confounding factors in relation to prolonged ICU stay (n: 175).
ICU: intensive care unit; OR: odds ratio; 95%CI: 95% confidence interval; GT: gastrointestinal tract; O2: complementary oxygen; HFNC: high flow nasal cannula. Table 4: Multivariate logistic regression to rule out possible confounding factors in relation to prolonged ICU stay (n: 175).
Discussion
Airway diseases are a frequent cause of hospitalization of pediatric patients, due to the characteristic aspects of this population, when compared to adults, which involves nasal breathing, smaller alveolar surface and small airway caliber. These factors predispose to the development of early acute respiratory insufficiency. Thus, it is necessary to know the different types of ventilatory supports and their complications [2].
Invasive mechanical ventilation via endotracheal tube was the most used ventilatory support in the first 24 hours of the studied sample. It is a fundamental support in the treatment of critical patients and its delay is related to worse outcomes in some studies. Kangelaris, et al. evaluated 457 patients with respiratory failure and those who underwent late intubation had a higher mortality rate [8]. Carroll, et al. reported that children who underwent late orotracheal intubation had an increased risk of complications related to the procedure, including decreased oxygen saturation, hypotension and bradycardia [9]. Crulli, et al. and Payen, et al. found an increase in the time of use of invasive mechanical ventilation and ICU stay in patients who had failed NIV when compared to those who underwent early OI (p < 0,05) [10, 11].
We also identified an association between late orotracheal intubation and prolonged ICU stay.
We noticed that only 44,9% (22/49) of the children who used NIV presented therapeutic success. Lins, et al. in their study evaluating the therapeutic efficacy of NIV in critically ill children, identified that 95% of patients who used this device had therapeutic success [12]. Nizarali, et al., Morris, et al. & Cavari, et al. identified similar results, with 80%, 75% e 64% effectiveness, respectively [13, 14, 15]. Our main hypothesis for the low effectiveness of NIV in our population was the high frequency of comorbidities, especially cerebral palsy with severe dysfunction [16].
Murphy, et al. identified that patients with neurological impairment have a higher risk of prolonged hospitalization and increased hospital costs compared to patients without this comorbidity [17]. Some anatomical and physiological characteristics may justify these data, partly due to the presence of kyphoscoliosis and chest deformity; respiratory muscle weakness; presence of chronic uncontrolled lung diseases, such as asthma and bronchodysplasia; greater difficulty in adjusting to the interface of non-invasive mechanical ventilation; increased bronchial secretion; and weak cough reflex [18, 19]. Neurological comorbidity was the only variable characterized as an independent marker of prolonged ICU stay in our sample. Dohna Schwake, et al. also identified that patients with comorbidities are at higher risk of NIV failure [20]. Other studies indicate that the main predictors of NIV failure are high inspiratory pressure, inspiratory oxygen fraction ≥ 80% and high PRISM score [21, 22, 23]. Further studies are needed to assess the impact of clinical comorbidities on the risk of NIV failure.
The high-flow nasal cannula group had a higher rate of therapeutic success when compared to patients who used NIV (90% versus 44,9%). However, the two groups showed heterogeneous clinical and demographic characteristics, with an increased risk of bias in the result found. Other studies have already compared the two devices, mainly in the treatment of infants with viral bronchiolitis, with divergent results in the medical literature [24, 25, 26, 27, 28, 29].
The isolated use of oxygen therapy in the first 24 hours of admission was characterized as an independent protection marker for prolonged hospitalization in the pediatric ICU. Probably, patients who require only complementary oxygen have less clinical severity, with early discharge. Tracheostomized patients have chronic and complex clinical conditions and pneumonia was the main reason for admission to our ICU. The tracheostomy cannula does not allow the natural process of heating, filtering and humidifying the air that normally occurs in the nasal cavity of children, with an increase in bronchial secretion and risk of infection [29]. Kun, et al. described that the main cause of hospital readmission in tracheostomized patients dependent on mechanical ventilation was pneumonia [30]. Tan, et al. identified that patients with tracheostomy had a 3-fold increase in the risk of bacterial infection of the respiratory tract when compared to control, mainly by gram-negative bacteria [31].
Our study had some limitations inherent to retrospective observational studies. The population had a high frequency of comorbidities due to the fact that the research took place in a reference center for rare diseases. In addition, due to the complexity of the cases, some patients were under investigation, so that they were classified only with syndromic diagnosis. Finally, variables that could interfere with clinical status and research outcomes such as hemodynamic shock, catheter-related infection and pneumothorax were not collected in the present study.
Conclusion
The main ventilatory support used in the admission of severe pediatric patients with respiratory insufficiency was invasive mechanical ventilation via endotracheal tube. Non- invasive ventilation had a high failure rate and late orotracheal intubation was statistically associated with increased length of stay in the intensive care unit. Neurological impairment was characterized as an independent marker of prolonged hospitalization. Further studies are needed to assess the association between clinical comorbidity and failure of non- invasive ventilation.
References
-
Teague WG (2003) Noninvasive ventilation in the pediatric intensive care unit for children with acute respiratory failure. Pediatric Pulmonology 35(6): 418- 426.
-
Friedman ML, Nitu ME (2018) Acute respiratory failure in Children. Pediatr Ann 47(7): e268-e273.
-
Yanez LJ, Yunge M, Emilfork M, Lapadula M, Alcantera A, et al. (2008) A prospective, randomized, controlled trial of noninvasive ventilation in pediatric acute respiratory failure. Pediatr Crit Care Med 9(5): 484-489.
-
Ferrer M, Esquinas A, Leon M, Gonzalez G, Alarcon A, et al. (2003) Noninvasive ventilation in severe hypoxemic respiratory failure: a randomized clinical trial. Am J Respir Crit Care Med 168(12): 1438-1444.
-
Sztrymf B, Messika J, Bertrand F, Hurel D, Leon R, et al. (2011) Beneficial effects of humidified high flow nasal oxygen in critical care patients: a prospective pilot study. Intensive Care Med 37(11): 1780-1786.
-
Kang BJ, Koh Y, Lim CM, Huh JW, Beak S, et al. (2015) Failure of high-flow nasal cannula therapy may delay intubation and increase mortality. Intensive Care Med 41(4): 623-632.
-
Moretti M, Cilione C, Tampieri A, Fracchia C, Marchioni A, et al. (2000) Incidence and causes of non-invasive mechanical ventilation failure after initial success. Thorax 55(10): 819-825.
-
Kangelaris KN, Ware LB, Wang CY Janz DR (2016) Time of Intubation and Clinical Outcomes in Adults with Acute Respiratory Distress Syndrome. Crit Care Med 44(1): 120-129.
-
Carroll CL, Spinella PC, Corsi JM, Stolz P, Zucker AR (2010) Emergent endotracheal intubations in children: be careful if it’s late when you intubate. Pediatr Crit Care Med 11(3): 343-348.
-
Crulli B, Loron G, Nishisaki A, Harrington K, Essouri S, et al. (2016) Safety of paediatric tracheal intubation after non-invasive ventilation failure. Pediatr Pulmonol 51(2): 165-172.
-
Payen V, Jouvet P, Lacroix J, Ducruet T, Gauvin F (2012) Risk factors associated with increased length of mechanical ventilation in children. Pediatr Critical Care Med 13(20): 152-157.
-
Lins ARBS, Duarte MCM, Andrade LB (2019) Noninvasive ventilation as the first choice of ventilatory support in children. Rev Bras Ter Intensiva 31(3): 333-339.
-
Nizarali Z, Cabral M, Silvestre C, Abadesso C, Nunes P, et al. (2012) Noninvasive ventilation in acute respiratory failure from respiratory syncytial virus bronchiolitis. Rev Bras Ter Intensiva 24(4): 375-380.
-
Morris JV, Ramnarayan P, Parslow RC, Fleming SJ (2017) Outcomes for Children Receiving Noninvasive Ventilation as The First -Line Mode of Mechanical Ventilation at Intensive Care Admission: A Propensity Score-Matched Cohort Study. Ped Crit Care Med 45(6): 1045-1053.
-
Cavari Y, Sofer S, Rozovski U, Lazar I (2012) Non invasive positive pressure ventilation in infants with respiratory failure. Pediatr Pulmonol 47(10): 1019-1025.
-
Himmelmann K, Beckung E, Hagberg G, Uvebrant P (2006) Gross and fine motor function and accompanying impairments in cerebral palsy. Dev Med Child Neurol 48(6): 417-423.
-
Murphy NA, Hoff C, Jorgensen T, Norlin C, Young PC (2016) Cost and Complications of Hospitalizations for Children with Cerebral Palsy. Pediatric Rehabilitation 9(1): 47-52.
-
Boel L, Pernet K, Toussaint M, Ides K, Leemans G, et al. (2019) Respiratory morbidity in children with cerebral palsy: an overview. Dev Med Child Neurol 61(6): 646- 653.
-
Proesmans M, Vreys M, Huenaerts E, Haest E (2015) Respiratory morbidity in children with profound intellectual and multiple disability. Pediatr Pulmonol 50(10): 1033-1038.
-
Dohna Schwake C, Stehling F, Tschiedel E, Wallot M, Millies U (2011) Non-invasive ventilation on a pediatric intensive care unit: feasibility, efficacy, and predictors of success. Pediatr Pulmonol 46(11): 1114-1120.
-
Munoz Bonet JI, Flor Macian EM, Brines J, Rosello Millet PM, Cruz Llopis M, et al. (2010) Predictive factors for the outcome of noninvasive ventilation in pediatric acute respiratory failure. Pediatr Crit Care Med 11(6): 675- 680.
-
Mayordomo Colunga J, Medina A, Rey C, Daz JJ, Concha A, et al. (2009) Predictive factors of non invasive ventilation failure in critically ill children: A prospective epidemiological study. Intensive Care Med 35(5): 527- 536.
-
Bernet V, Hug MI, Frey B (2005) Predictive factors for the success of noninvasive mask ventilation in infants and children with acute respiratory failure. Pediatr Crit Care Med 6(6): 660-664.
-
Clayton JA, McKee B, Slain KN, Rotta AT, Shein SL (2019) Outcomes of Children With Bronchiolitis Treated With High-Flow Nasal Cannula or Noninvasive Positive Pressure Ventilation. Pediatr Crit Care Med 20(2): 128- 135.
-
Milési C, Essouri S, Pouyau R, Liet JM, Afanetti M, et al. (2019) High flow nasal cannula (HFNC) versus nasal continuous positive airway pressure (nCPAP) for the initial respiratory management of acute viral bronchiolitis in young infants: A multicenter randomized controlled trial (TRAMONTANE study). Intensive Care Med 43(2): 209–216.
-
Habra B, Janahi IA, Dauleh H, Chandra P, Veten A (2020) A comparison between high-flow nasal cannula and noninvasive ventilation in the management of infants and young children with acute bronchiolitis in the PICU. Pediatr Pulmonol 55(2): 455-461.
-
Modesto I Alapont V, Pons Òdena M, Medina A (2019) High-flow nasal cannula versus noninvasive ventilation: a matter of confusion. Pediatr Crit Care Med 20(12): 1210-1211.
-
Bem RA (2019) Noninvasive high flow versus noninvasive positive pressure in children with severe bronchiolitis: the battle of the PICU continues. Pediatr Crit Care Med 20(2): 192-193.
-
Watters KF (217) Tracheostomy in infants and children. Respir Care 62(6): 799-825.
-
Kun SS, Edwars JD, Ward SLD, Keens TG (2012) Hospital Readmissions for Newly Discharged Pediatric Home Mechanical Ventilation Patients. Pediatr Pulmonol 47(4): 409-414.
-
Tan CT, Chiu NC, Lee KS, Chi H, Huang FY, et al. (2020) Respiratory tract infections in children with tracheostomy. J Immunol infect 53(2): 315-320.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index