Clinical Characteristics of Patients with COVID-19 and Its Relation with Diabetes in ICU of Bangabandhu Sheikh Mujib Medical University, Bangladesh
Background: Coronaviruses are a group of RNA viruses that cause respiratory tract infections ranging from mild to critical illness in humans and animals. The prevalence of diabetes mellitus (DM) and raised blood glucose levels can act as independent factors of mortality and morbidity related to COVID-19. Objective: Aim of the study is to analyze detailed clinical data of patients with diabetes and confirmed COVID-19 and to compare the clinical outcome of Covid-19 cases between diabetic and non-diabetic patients. Method: A retrospective cohort study was conducted among 300 patients of confirmed COVID-19 admitted to ICU of Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh during July 2020 to December 2020. Results: In this study, maximum number (49%) of patients was in the age group of 61 to 75 years and minimum number (3%) of patients were 15 to 30 years of age group. There were (74.33%) male patients and (25.67%) female patients. Regarding co-morbidities, more than half of the patients were suffering from Diabetes (60.22%) and Hypertension (53.44%). Significant amount of patients were also suffering from chronic obstructive pulmonary disease (27%) and bronchial asthma (16.66%). Ischemic heart disease was (10.33.%), chronic kidney disease (10.89%) and hypothyroidism(9.78%) at the time of admission. Among the three group we found that mortality rate of diabetic patients is higher than non-diabetic patient’s. Mortality rate in non-diabetic case were 53.78% , diabetic patients without other co-morbidity were 75% and diabetic patients with other co-morbidity were 86.78%. In every group male mortality was higher than female mortality. Conclusion: In this study we compared the clinical features of COVID-19 patients with diabetes and non-diabetic ICU admitted cases. Diabetic patients with other co morbidities in ICU cases showed higher rates of mortality. The high mortality in severe COVID-19 patients with diabetes indicated that we need more supervision on these patients.
Introduction
The world is now facing Corona virus disease 2019 (COVID-19) which is rapidly spreading [1, 2] all over the world. Corona virus is an irresistible, infectious illness of the respiratory framework brought about by a shifting, novel strain of the severe intense respiratory disorder related COVID (SARS-CoV) known as the severe intense respiratory condition related to COVID 2 (SARSCoV-2) [3]. SARS-CoV-2 is an encompassed, beta Covid-19 comprising of a solitary abandoned positive-sense RNA (23e32 kb) as its center hereditary material [4]. SARS-CoV-2 for the most part spreads through Human to human transmission (HHT) by methods for respiratory drops through direct contact or fomite and mist concentrates [5, 6]. With expanding quantities of instances of COVID-19 universally, the World Health Organization (WHO) proclaimed the COVID-19 outbreak a pandemic on March 11, 2020. As of 3rd March, 2021, the world has already witnessed 2,560,638 deaths among 115,302,022 cases and Bangladesh has reported 547,316 confirmed cases among which 498,391 has recovered and 8,423 died [7]. Many studies have reported the epidemiologic and clinical characteristics of patients with COVID-19. Respiratory distress, persistent worsening cough, fever, fatigue, sore throat, rhinorrhea, diarrhea, chest pain, normal or reduced white blood cell count, and imaging evidence of viral pneumonia are the clinical features of COVID-19. Some patients had rapid organ dysfunction, including acute respiratory distress syndrome leading to death [8].
Diabetes mellitus is an chronic metabolic sickness described by the event of hyperglycemia for a drawn-out period. It is related to serious long-term complications, including cardiovascular disease and chronic kidney disease [9]. Diabetes is among the top 10 causes of adult deaths worldwide which affects 422 million people, has a major impact on global health and 1.6 million deaths are directly attributed to diabetes each year [10]. Two corona viruses have emerged in the past two decades that have caused widespread respiratory illness and deaths. In 2002, SARS coronavirus (SARS-CoV) was first emerged in China, causing severe acute respiratory syndrome (coronavirus). Another corona virus, MERS-coronavirus (MERS-CoV) causing Middle East respiratory syndrome emerged in Saudi Arabia in 2012. Diabetes was a risk factor for poor prognosis and mortality which was revealed by the experience with both of the syndromes [11, 12]. Similarly, the clinical characteristics of COVID-19 showed a similar trend of initial reports [13, 14]. Recent studies have advanced that the prevalence of diabetes mellitus (DM) and raised blood glucose levels can act as independent factors of mortality and morbidity related to COVID-19 in spite of having quite limited data; right off the bat since people with diabetes have a delayed recovery duration from viral illnesses due to having an undermined immune system and also for the infection’s capacity to support itself in a climate with high glucose levels putting people with diabetes mellitus in a weak situation from the part of setbacks because of COVID-19 [15]. Many studies have suggested that in patients the prevalence of diabetes with mild covid-19 may range from 5.7% to 5.9%, [16] while the prevalence of diabetes mellitus in patients with severe Covid-19 has seen a sharp rise from 22.2% to 26.9% [17]. These epidemiological confirmations demonstrate a basic part of diabetes in patients with extreme Corona virus. Diabetes and hyperglycemia are accounted for to intensify aggravation by expanding the arrival of tumor putrefaction factor α (TNFα) and interleukin (IL) 10 [18]. Moreover, diabetes may prompt to lung dysfunction, like diminished constrained expiratory volume and constrained crucial limit [19]. Therefore, diabetes could possibly be a risk factor for covid-19.
It has been reported that ICU patients have a higher proportion of diabetes compared with non-intensive care unit (ICU) patients [16]. It is recommended that diabetes may influence the clinical appearances and illness movement of patients. To explain the clinical attributes of diabetes joined with COVID-19, we reflectively gathered and examined point-by-point clinical information of patients with diabetes and affirmed COVID-19, portrayed their clinical qualities, and contrasted clinical attributes of patients with diabetes of ICU patients.
Objective
General Objective
• The objective of this study is to analyze detailed clinical data and outcome of COVID-19 positive patients with diabetes.
Specific Objective
• To compare the clinical outcome of Covid-19 cases between diabetic and non-diabetic patients.
• To compare the mortality rate of confirmed COVID-19 patients between diabetic, non diabetic and diabetic with other co morbidities.
Method
This retrospective-observational study was conducted on 300 confirmed COVID-19 patients admitted in intensive care unit of Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh during July 2020 to December 2020.
Inclusion criteria
- Adults (over 18 years old).
- Laboratory confirmation of covid-19 by real- time PCR.
- Chest CT findings meeting the standard for diagnosis of covid-19.
Exclusion criteria
- Missing data on clinical characteristics.
- Missing data on laboratory characteristics.
Data collection
From patients’ electronic medical records epidemiologic, demographic, clinical, laboratory, radiologic, treatment, and outcome data were obtained. All information was collected and managed with a data collection form. To ensure the accuracy of the data, 2 researchers (YYL and ZSJ) checked the data independently.
Statistical analysis
All data were analyzed by SPSS (V.22.0) statistical tools
Result
Table 1 shows the age distribution of the patients. Here maximum number (49%) of patients were in the age group of 61 – 75 years and minimum number (3%) were in the 15 – 30 year’s age group. The mean age was 62.8 years.
Shows the gender distribution of the patients. Among the 300 patients, 223 (74.3%) were male and 77 (25.6%) were female.
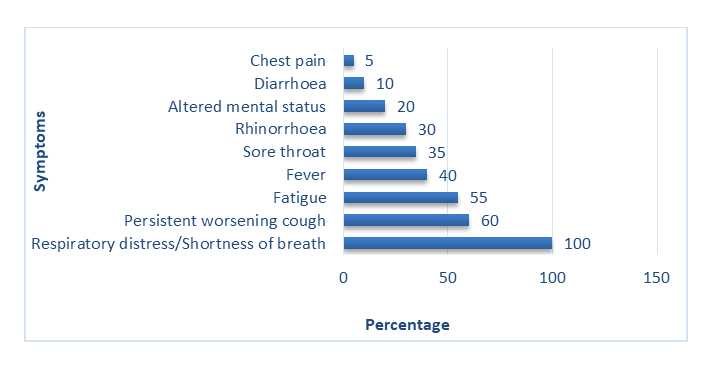
Patients were admitted with symptoms like, respiratory distress/shortness of breath (100%), persistent worsening cough (60%), fatigue (55%), and fever (40%). Patients were also present with sore throat (35%), rhinorrhea (30%), altered mental status (20%), diarrhea (10%) and chest pain (5%) as shown in figure 2.
| Frequency | Percentage (%) | |
|---|---|---|
| Diabetes mellitus | 181 | 60.22% |
| Hypertension | 160 | 53.44% |
| Chronic obstructive pulmonary disease | 81 | 27.00% |
| Ischemic heart disease | 31 | 10.33% |
| Chronic kidney disease | 33 | 10.89% |
| Bronchial asthma | 50 | 16.66% |
| Hypothyroidism | 29 | 9.78% |
Table 1: Co-morbidities of the patients.
We divided the 300 patients into two separate groups. Total 181(60.22%) patients with diabetes were included in group A and 119(39.78%) patients without diabetes were included in group B.
| Frequency | Percentage | Male | Percentage | Female | Percentage | |
|---|---|---|---|---|---|---|
| Group A (Diabetic) | 181 | 60.22% | 144 | 48% | 37 | 12% |
| Group B (Non-diabetic) | 119 | 39.78% | 95 | 32% | 24 | 8% |
| Total | 300 | 100% | 239 | 80% | 61 | 20% |
Table 2: Groups of ICU patients.
The group of 181 diabetic patients (Group A) were sub- divided into two other groups. Group A1 total 121 patients were diabetic with other co-morbidities and group A2 total 60 patients were diabetic without other co-morbidities.
| Frequency | Male | Male Percentage | Female | Female Percentage | Total Percentage | |
|---|---|---|---|---|---|---|
| Group A1: Diabetic patients with other co-morbidities | 121 | 77 | 63.64% | 44 | 36.36% | 100% |
| Group A2: Diabetic patients without other co-morbidities | 60 | 45 | 75.00% | 15 | 25.00% | 100% |
| Total | 181 | 122 | 67.4 | 59 | 32.60% | 100% |
Table 3: Sub-groups according co-morbidities of diabetic patients.
Among the three groups of patients, In Group A1: among 121 diabetic patients with other co-morbidities total 105 patients were dead where male mortality was highest 77.14% and female mortality were (22.86%). In Group A2: among 60 diabetic patients without other co-morbidities total 45 patients were dead where male mortality was highest 75.56% and female mortality were (24.44%). In Group A3: among 119 non-diabetic patients total 45 patients were dead where male mortality was highest 65.6% and female mortality were (34.4%). Mortality rate was found to be higher in ICU male patients (Table 5).
| Frequency | Total Death | Male Death | Male Mortality (%) | Female Death | Female Mortality (%) | Total Mortality Percentage | |
|---|---|---|---|---|---|---|---|
| Group A1: Diabetic patients with other co-morbidities | 121 | 105 | 81 | 77.14 | 24 | 22.86 | 86.78 |
| Group A2: Diabetic patients without other co-morbidities | 60 | 45 | 34 | 75.56 | 11 | 24.44 | 75.00% |
| Non-diabetic | 119 | 64 | 42 | 65.6 | 22 | 34.4 | 53.78 |
| Total | 300 | 214 | 159 | 55 |
Table 4: Mortality rate of different groups of patients.
Discussion
This retrospective-observational study provides information on the clinical characteristics of patients with diabetes and COVID-19 in Dhaka, Bangladesh. We acquired the definite clinical information of the patients included. The 2019 CoV is the seventh known COVID that can taint people, and the other 6 are human COVID (HCoV)- 229E, HCoV- OC43, HCoV-NL63, HCoV-HKU1, extreme intense respiratory condition related COVID (SARS-CoV), and Middle East respiratory disorder related COVID (MERS-CoV) [20]. The 2 profoundly pathogenic infections, SARSCoV and MERSCoV, cause extreme respiratory disorder in people and the other 4 human Covids prompt gentle upper respiratory sickness. Like SARS-CoV and MERS-CoV, the progressing episode of COVID-19 has been proclaimed by the WHO as a worldwide public health crisis. A very few studies have exposed the clinical qualities of COVID-19 [1, 21, 22]. In our study we have studied 300 covid-19 patients and their mean age was 62.8 years. In another study [23] from our country showed mean age was 42.59±14.43 years. Mean age of patients were more in this study because this study was done on ICU patients where the patients were elderly and multiple co-morbid. We found a greater percentage of male (74.33%) than female (25.67%) affected with COVID-19. Similar male preponderance was found in other studies, 73% of the first reported study of China [24] or 63% of a study in DMCH, Bangladesh [25]. Based on our study, the symptoms of COVID- 19 patients with diabetes were similar to the general population as previously reported; the most common symptoms were fever, cough, and fatigue, respiratory distress [1].
Previous studies proposed that patients with severe COVID-19 had a high prevalence of diabetes, [16, 17] which was nearly 20% compared with 11.6% [26] in Chinese adults. We observed that the prevalence of diabetes in patients with severe Covid-19 was up to 60.22%. Percentage of diabetes was more in our study because most of our patients were aged and critically ill. Patients with diabetes were more likely to develop COVID-19, which may be due to the fact that patients with diabetes had low pulmonary function. Animal studies suggested that alveolar capillary micro-angiopathy and interstitial fibrosis were induced by glycosylation of the lung tissue collagen in the diabetes model, and this process was mediated by nicotinamideadenine dinucleotide phosphate (NADPH) oxidase and angiotensin II [27].
Post-mortem likewise distinguished that patients with diabetes had thickening lung basal lamina, [28] which may impact pneumonic dispersion work. Late investigations demonstrate that the 2019-nCoV is bound to contaminate more established grown-up guys with on-going co morbidities [1, 8]. The rates of diabetes in ICU cases were 22.2% [16]. According to a recent study, the estimated mortality rate of COVID-19 would be 5.6% for China and 15.2% outside of China [29].In-hospital mortality was even much higher (28%), as reported by Fei Zhou, et al. [30]. According to our study, patients with severe covid-19 with diabetes had a similar pattern of clinical characteristics. In our study we found that mortality rate of diabetic patients is higher than non-diabetic patient’s. In diabetic patients with other co-morbidities male mortality was highest 77.14% and female mortality were (22.86%), diabetic patients without other co-morbidities male mortality was 75.56 % and female mortality were (24.44%) and non-diabetic patient’s male mortality was 65.6% and female mortality were (34.4%). Developing country like Bangladesh, the mortality rate is comparable to that reported by Richardson, et al. from New York (75.6%) [31], Arentz, et al. from Washington (67%) [32], and Yang, et al. (61.5%) from China [33].
Several study shown that people with diabetes are more vulnerable to the severe effects of the virus. In Bangladesh, the number of people infected is increasing rapidly in a population that already has a high prevalence of diabetes. Over 8 million people are estimated to be living with diabetes in the country and a similar number are at high risk of developing type 2 diabetes. Bangladesh has reported over 547,316 cases of COVID-19 and recorded 8423 confirmed deaths in hospital from the virus. The numbers emphasize the importance for people living with diabetes to take all the recommended precautions to avoid the virus and to have access to the health care required to manage their condition [34]. In our study, average mortality of patients is comparatively high because we studied on the ICU patients which were in critical condition and aged person with server complexity. The outcome of mechanically ventilated were poor. Oxygen therapy was provided through Non-invasive devices both in cabin and ward. So, the critically ill patients were arriving late to the ICU.
Conclusion
In this study we compared the demographic and clinical features and mortality rate of COVID-19 patients of non-diabetic and diabetic patients with or without other comorbidities in ICU. Diabetic patients with other co- morbidities in ICU cases showed higher rates of mortality than non-diabetic ICU patients and diabetic patients without other co-morbidities. Male diabetic ICU patient’s mortality was higher than female diabetic ICU patient’s mortality. The high mortality in severe COVID-19 patients with diabetes and other comorbidities indicate that we need more supervision on these cases.
References
-
Huang C, Wang Y, Li X, Lili Ren , Jianping Zhao, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuha, China. 395(10223): 497- 506.
-
Zhu N, Zhang D, Wang W, Xingwang Li , Bo Yang, et al. (2020) A novel coronavirus from patients with pneumonia in China, 2019. 382(8): 727-733.
-
Jin Y, Yang H, Ji W, Wu W, Chen S, et al. (2020) Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses 12(4): 372.
-
Perrotta F, Matera MG, Cazzola M, Bianco A (2020) severe respiratory SARS-CoV2 infection: does ACE2 receptor matter? Respir Med 168: 105996.
-
Adhikari SP, Sha Meng, Yu-Ju Wu, Yu-Ping Mao, Rui-Xue Ye, et al. (2020) Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infectious diseases of poverty 9(1): 29.
-
Jalava K (2020) First respiratory transmitted food borne outbreak? Int J Hyg Environ Health 226: 113490.
-
WHO (2021) Bangladesh. Situation report coronavirus (COVID- 19).
-
Chen N, Zhou M, Dong X, Qu J, Gong F, et al. (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. 395(10223): 507-513.
-
Forbes JM, Cooper ME (2013) Mechanisms of diabetic complications. Physiol Rev 93(1): 137-188.
-
Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, et al. (2019) Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res ClinPract 157: 107843.
-
Badawi A, Ryoo SG (2016) Prevalence of comorbidities in the Middle East respiratory syndrome coronavirus (MERS-CoV): a systematic review and meta-analysis. Int J Infect Dis 49: 129-133.
-
Yang JK, Feng Y, Yuan MY, Yuan SY, Fu HJ, et al. (2006) Plasma glucose levels and diabetes are independent predictors for mortality and morbidity in patients with SARS. Diabet Med 23(6): 623-628.
-
Alshukry A, Ali H, Ali Y, Al-Taweel T, Abu-Farha M, et al. (2020) Clinical characteristics of Coronavirus Disease 2019 (COVID-19) patients in Kuwait. medRxiv 11: 33.
-
Petrosillo N, Viceconte G, Ergonul O, Ippolito G, Petersen E (2020) COVID-19, SARS and MERS: are they closely related? ClinMicrobiol Infect 26(6): 729-734.
-
Guo W, Mingyue Li, Yalan Dong, Haifeng Zhou, Zili Zhang, et al. ()Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes/metabolism research and reviews 31: e3319.
-
Wang D, Hu B, Hu C, Zhu F,Liu X, et al. (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 323(11): 1061-1069.
-
W-j G, Z-y N, Hu Y , Liang W, Ou Jc, et al . (2020) Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 382: 1708-1720.
-
Ouchi N, Parker JL, Lugus JJ, Kenneth Walsh (2011) Adipokines in inflammation and metabolic disease. Nat Rev Immunol 11: 85-97.
-
Klein OL , Aviles-Santa L , Cai J , Collard HR, Kanaya AM, et al. (2016) Hispanics/Latinos with type 2 diabetes have functional and symptomatic pulmonary impairment Mirroring kidney microangiopathy: findings from the Hispanic community health Study/Study of Latinos (HCHS/SOL). Diabetes Care 39(11): 2051-2057.
-
Su S, Wong G, Shi W, Jun Liu, Alexander C K Lai, et al. (2016) Epidemiology, genetic recombination, and pathogenesis of coronaviruses. Trends Microbiol 24(6): 490-502.
-
Chen H, Guo J, Wang C, Fan Luo, Xuechen Yu, et al. (2020) Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet 395(10226): 809-815.
-
Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, et al. (2020) First case of 2019 novel coronavirus in the United States. N Engl J Med 382(10): 929-936.
-
Hasan JM, Khan MAS, Rahman M, Islam MS, Debnath S, et al. (2020) Sociodemographic profile, clinical characteristics, anxiety, and depression of 74 patients infected with COVID-19: first report from Bangladesh.
-
N Chen, M Zhou, X Dong, J Qu, F, et al. (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395(10223): 507-513.
-
SGM Mowla, KAK Azad, A Kabir et al, Clinical and Epidemiological Profile of 100 Confirmed COVID-19 Patients Admitted in Dhaka Medical College Hospital, Dhaka, Bangladesh, Journal of BCPS 38: 29-36.
-
Xu Y, Wang L, He J, Yufang Bi, Mian Li, et al. (2013) Prevalence and control of diabetes in Chinese adults. JAMA 310(9): 948-959.
-
Yang J, Tan Y, Zhao F, Zhongsen Ma, Yuehui Wang, et al. (2011) Angiotensin II plays a critical role in diabetic pulmonary fibrosis most likely via activation of NADPH oxidase-mediated nitrosative damage. Am J Physiol Endocrinol Metab 301(1): E132-144.
-
Weynand B, Jonckheere A, Frans A, (1999) Diabetes mellitus induces a thickening of the pulmonary basal lamina. Respiration 66(1): 14-19.
-
Baud D, Qi X, Nielsen-Saines K, Musso D, Pomar L, et al. (2020) Real estimates of mortality following COVID-19 infection. Lancet Infect Dis 20(7): 773.
-
Zhou F, Yu T, Du R, Fan G, Liu Y, et al. (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 395(10229): 1054-1062.
-
Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, et al. (2020) Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 323(2020): 2052-2059.
-
Arentz M, Yim E, Klaff L, Lokhandwala S, Riedo FX, et al. (2020) Characteristics and outcomes of 21 critically ill Patients with COVID-19 in Washington State. JAMA 323(16): 1612-1614.
-
Yang X, Yu Y, Xu J, Shu H, Xia J, et al. (2020) Clinical course and outcomes of critically ill patients with SARS- CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 8(5): 475-481.
-
Bishwajit Bhowmik, Akhtar Hussain, AK Azad Khan (2020) Diabetes Voice: Caring for people with diabetes in Bangladesh during COVID-19.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index