Extracorporeal Support in a Child with Severe Carbon Monoxide Poisoning and Shock: A Case Report
A 12-year-old girl who developed profound respiratory and cardiac failure following smoke inhalation and severe carbon monoxide poisoning that required extracorporeal membrane oxygenation (ECMO) for 5 days after which time the patient was extubated and discharged home with no signs of neurological sequelae. Although rarely described, the early use of ECMO support improved gas exchange from severe hypoxemia and shock while preserving end-organ function.
Introduction
Carbon monoxide poisoning is the leading cause of morbidity and mortality following house fires [1]. Carbon monoxide poisoning is common in the modern world and United States, accounting for an estimated 15,000 emergency department visits annually. It is also one of the leading causes of poisoning deaths, it was responsible for approximately 450 deaths each year during 1999--2004 and an estimated 15,200 emergency department visits each year during 2001--2003, according to the Centers for Disease Control and Prevention [2]. The toxicity of carbon monoxide appears to result from a combination of tissue hypoxia [3, 4, 5] and direct carbon monoxide–mediated damage at the cellular level [5, 6, 7]. Carbon monoxide competes with oxygen for binding to affinity of hemoglobin for carbon monoxide is 200 to 250 times as great as its affinity for oxygen [3, 5]. The consequences of this competitive binding are a shift of the oxyhemoglobin dissociation curve to the left [4] resulting in impaired release of oxygen at the tissue level and causing cellular hypoxia. Carbon monoxide binds to heme proteins [5, 8] interrupting cellular respiration and causing production of reactive oxygen species [7, 9] which in turns cause neuronal loss [9], Apoptosis [10] and cardiac injury [11]. Respiratory failure following inhalational smoke results from direct mucosal injury and from the activation of inflammatory mechanisms. Cardiovascular instability occurs as a result of decreased oxygen delivery and myocardial hypoxia which also can result in cardiac injury [12, 13]. We report the successful treatment of a child with severe carbon monoxide poisoning with acute respiratory distress syndrome and cardiovascular collapse supported with extracorporeal membrane oxygenation.
Case Report
A 12-year-old girl was found in a house fire by medical personnel unresponsive with agonal respirations. She was successfully intubated in the emergency department and admitted to the Pediatric Intensive Care Unit. Her initial carboxyhemoglobin level of 35% was associated with metabolic acidosis (lactate level 5.6mmol/L, bicarbonate level 15 mmol/L) and severe hypoxemia (arterial PaO2 39mmHg, on FiO2 100%). Anteroposterior chest radiography (Figure 1A) revealed bilateral diffuse airspace opacities. A nasogastric tube was placed which showed charcoal in her gastric contents. Fiberoptic bronchoscopy revealed copious pulmonary edema but no evidence of thermal injury or to the level of the fourth generation bronchi. Attempts were made to place her both on conventional ventilation (Servoi 300, Bridgewater, NJ, USA) with positive end expiratory pressure as high as 16 cm H2O. Continued, progressive desaturation prompted an attempt at high frequency oscillatory ventilation with mean airway pressures as high as 50 mmHg without increase in the arterial oxygen tension. She was volume resuscitated with 40ml/kg normal saline and placed on dopamine and epinephrine infusions to support her blood pressure. Despite these interventions, she remained hypotensive with evidence of cardiac injury with an elevated troponin to 3.87 ng/ml.
Given the degree of profound hypoxemia (oxygenation index 107), she was placed on extracorporeal membrane oxygenation (ECMO, Bio Medicus centrifugal Bio pump P50) support five hours following the initial injury. Vascular cannulation was achieved by cutdown introduction of wire-reinforced cannula into the right atrium through the right internal jugular vein (drain cannula- BioMedicus 30 French, Eden Prairie, MN ) and right common carotid artery (return cannula- BioMedicus 20 French, Eden Prairie, MN). Her arterial PaO2 before she was placed on ECMO was 39 mmHg and after being placed on ECMO was 220mmHg. After cannulation, she was placed on rest settings on the conventional ventilator (Servoi 300Bridgewater, NJ, USA) with positive end- expiratory pressure of 5 cmH2O, rate of 10 breaths /min and pressure control of 25 cmH2O to provide a tidal volume of 150-200 mL. She was maintained on full ECMO flow support of 3.5L/minute and carbon dioxide removal was achieved through the circuit by regulating the rate of sweep gas flow in the range of 4-5:1. She was maintained adequate activated clotting time (ACT) in the range of 180-220 seconds under the heparin infusion in the range of 20-35units/kg/hour.

Figure 1A: Posteroanterior chest radiography before ECMO cannulation demonstrated bilateral diffuse airspace opacities, left greater than right.
Her carboxyhemoglobin level rapidly returned to normal range within 24 hours after admission. Her lactate levels peaked at 5.6 mmol/L on hour 7 after admission and returned to normal level (1.4mmol/L) 24 hours after admission. Her troponin I levels peaked at 4.94 ng/ml on hour 15 after admission and returned to normal range 0.24 ng/ml by ICU day 4. Despite her initial hypotension and early evidence of acute tubular necrosis (transient anuria, fractional extraction of sodium 3.9%, fractional excretion of urea 57%), her urine output improved to at least 2 mL/kg/hr during ECMO support. She showed significant improvement of her cardiovascular system as evidenced by normal pulse pressures during ECMO circuit support, good urine output, and tolerating ECMO flow weaning at 90 hours post cannulation. Echocardiogram on ECMO day 1 and day 2 showed normal ventricular size and normal fractional shortening of 33% (normal 28- 40%). Follow up chest radiography revealed near complete resolution of the alveolar process on ECMO day 5 (Figure 1B). She was able to generate 4-5ml/kg tidal volume with moderate ventilator settings of a rate of 10/min, positive end expiratory pressure of 10 cmH2O, pressure control 30 cmH2O at 120 hours of ECMO support. She developed Enterobacter cloacae bacteremia on admission day 5 which was treated with broad spectrum antibiotics as well as right femoral intravenous catheter removal.
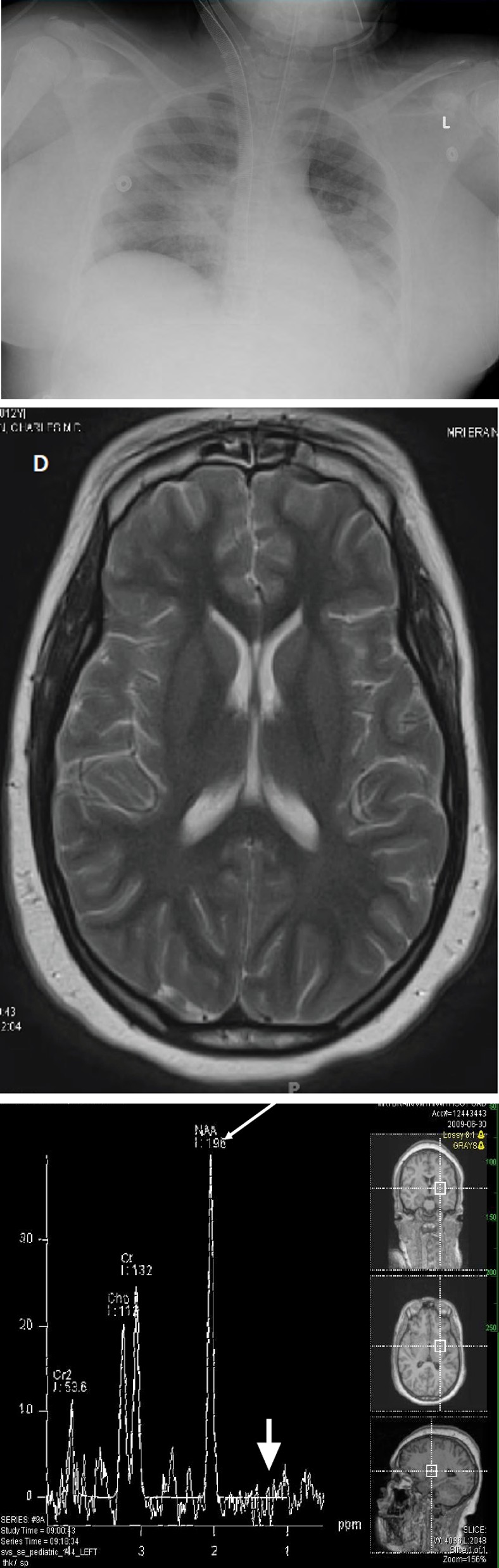
Figure 1B: Posteroanterior chest radiography right before decannulation demonstrated improved aeration of both lungs and improved patchy perihilar consolidation.
The patient was successfully decannulated on ICU day 5 (ECMO hour 127). She was extubated on ICU day 8 and transitioned to room air on ICU day 10. She underwent brain magnetic resonance imaging and magnetic resonance spectroscopy on ICU day 9 that revealed no abnormalities (Figure 1C,D).
Figure 1C: The magnetic resonance spectroscopy shows normal spectrum. There is no decrease in N-acetyl aspartate (white arrow) or increase in lactate (white arrowhead) to suggest brain injury related to carbon monoxide poisoning.
Her neurologic exam was non-focal and neuropsychiatry evaluation showed mild hoarse and slurred speech with good coordination during swallowing. She had weakness due to deconditioning and was transitioned out of the intensive care unit to the neurorehabilitation service. She became much more capable of working independently in her activities of daily living and starting on some early school work. Her endurance also improved and her gait had returned to normal. She was discharged home without evidence of neurologic sequelae on hospital day 16 after her initial injury.
Figure 1D: The susceptibility sensitive (T2*) sequence reveals no areas of signal loss to suggest hemorrhage. The T2-weighted images are normal. There are no areas of abnormal contrast enhancement.
Discussion
Carbon monoxide causes hypoxemia through the formation of high affinity carboxyhemoglobin [4] and a leftward shift of the oxyhemoglobin dissociation curve, which results in tissue hypoxia. Carbon monoxide binds to heme proteins cytochrome c oxidase and platelet heme protein) resulting in mitochondrial dysfunction and asphyxiation at the cellular level [5, 7, 9]. Brain hypoxia causes oxidative stress, necrosis, and apoptosis from a rat model10, contributing inflammation. The half-life of carbon monoxide is rapidly reduced from 320 minutes at 21%FiO2 (room air) to 31.5 to 149.7 minutes in normobaric 100% FiO2 [14]. Respiratory failure following smoke inhalation results from direct injury to the tracheobronchial tree manifested by loss of cilia, sloughing of bronchoepithelium, pseudomembrane formation, and hypoxia from carbon monoxide replacing oxygen on the heme protein [15]. Carbon monoxide and noxious chemical asphyxiants from combustion cause a release of chemotactic factors that ctivate leukocytes, leading to inflammation, oxidative stress and apoptosis [16].
Myocardial stunning from carbon monoxide toxicity is a result of impairment of oxygen utilization and inflammation reaction independent of the pathways to hypoxia [12, 13, 17]. In addition to cardiovascular and pulmonary injuries caused by carbon monoxide, patients commonly have neuropsychological sequelae after carbon monoxide poisoning [8, 18, 19]. Weaver, et al. reported 46% of poisoned patients treated with normobaric oxygen had cognitive sequelae 6 weeks after poisoning [19], and 45% had affective sequelae reported by Jasper, et al. [20]. Non- specific imagine findings such as basal-ganglia lesions [21], atrophy of the hippocampi [22], as well as abnormal results on MRI diffusion imaging have also been associated with carbon monoxide poisoning [23].
However, our patient has thus far had normal neuroimaging studies including magnetic resonance spectrometry as well as normal neurologic exams which may indicate preserved end-organ function especially in neurological outcome after early usage of ECMO support during the acute phase of carbon monoxide toxicity. There are no reported cases of ECMO support to treat carbon monoxide toxicity related hypoxemia and shock in a child to our knowledge. There are three case reports about adult extracorporeal support for carbon monoxide poisoning in the literature. Patton reported a 26-year-old male who suffered from thermal burns and inhalational injury developed acute respiratory distress syndrome and was treated successfully with veno-venous extracorporeal membrane oxygenation and was discharged 6 weeks later [24]. McCunn, et al. reported successful resuscitation a 34-year old male with severe smoke inhalation with concurrent cardiovascular collapse and acute respiratory distress syndrome supported with extracorporeal lung assist for 7 days and was decannulated and discharged to a transitional care facility neurologically intact [25]. Kornberger, et al. reported a 38-year-old male who developed respiratory failure 54 hours after admission, in whom CO2 could not be eliminated, was treated with extracorporeal CO2 removal for 30 days. This patient was able to wean from extracorporeal CO2 removal support but died of sepsis with multiple organ failure [26].
Although ECMO is a high-risk procedure in critically ill patients and both technical and patient-related complications frequently occur, our report provides evidence that early use of extracorporeal membrane oxygenation support for severe carbon monoxide poisoning with severe respiratory failure may preserve end-organ function and improve overall outcomes. This case report is waived from the report of Institutional Review Board of Washington University.
Conclusion
The ability of extracorporeal membrane oxygenation to provide cardiopulmonary support in patients with severe carbon monoxide poisoning with respiratory and circulatory failure may preserve end-organ function and improve outcomes.
Acknowledgement
Dr Lin JH was under the support of NIH T32 HL7272-29 grant.
References
-
Daniel Mathieu (1985) Carbon Monoxide Poisoning. Can Med Assoc J 133: 392-399.
-
Centers for Disease Control and Prevention (CDC)(2008) Nonfatal, Unintentional, Non--Fire-Related Carbon Monoxide Exposures --- United States, 2004--2006. MMWR 57(33): 896-899.
-
Haldane J (1895) the relation of the action of carbonic oxide to oxygen tension. J Physiol 18(3) 201-217.
-
Roughton FJW, Darling.RC (1994) the effect of carbon monoxide on the oxyhemoglobin dissociation curve. Am J Physiol 141(1): 17-31.
-
Thom S (2008) Carbon monoxide pathophysiology and treatment. In: Neuman TS, et al. (Eds.), Physiology and medicine of hyperbaric oxygen therapy. Philadelphia: Saunders Elsevier, 321-347.
-
Cronje FJ, Carraway MS, Freiberger JJ, Suliman HB, Piantadosi CA (2004) Carbon monoxide actuates O(2)- limited heme degradation in the rat brain. . Free Radic Biol Med 37(1): 1802-1812.
-
Alonso JR, Cardellach F, López S, Casademont J, Miró O (2003) Carbon monoxide specifically inhibits cytochrome c oxidase of human mitochondrial respiratory chain. Pharmacol Toxicol 93(3): 142-146.
-
Weaver L (2009) Clinical practice. Carbon monoxide poisoning. N Engl J Med 360(12): 1217-1225.
-
Thom SR, Bhopale V, Han ST, Clark JM, Hardy KR (2006) Intravascular neutrophil activation due to carbon monoxide poisoning. . Am J Respir Crit Care Med 174(11): 1239-1248.
-
Piantadosi CA, Zhang J, Levin ED, Folz RJ, Schmechel DE (1997) Apoptosis and delayed neuronal damage after carbon monoxide poisoning in the rat. Exp Neurol 147(1): 103-114.
-
Mannaioni PF, Vannacci A, Masini E (2006) Carbon monoxide: the bad and the good side of the coin, from neuronal death to anti-inflammatory activity. Inflamm Res 55(7): 261-273.
-
Satran D, Henry CR, Adkinson C, Nicholson CI, Bracha Y, et al. (2005) Cardiovascular manifestations of moderate to severe carbon monoxide poisoning. J Am Coll Cardiol 45(9): 1513-1516.
-
Balzan MV, Cacciottolo JM, Mifsud S (1994) Unstable angina and exposure to carbon monoxide. Postgrad Med J 70(828): 699-702.
-
Myers R (1987) Hyperbaric oxygen therapy for gas gangrene and carbon monoxide poisonings. In: Siegel JH (Eds.), Trauma: emergency surgery and critical care. New York: Churchill Livingstone, 1133-1169.
-
Hubbard GB, Langlinais P, Shimazu T, Okerberg C V, Mason AD, et al.(1991) The morphology of smoke inhalation injury in sheep J Trauma 31(11): 1477-1486.
-
Basadre JO, Sugi K, Traber DL, L D Traber, G D Niehaus, et al. (1998) The effect of leukocyte depletion on smoke inhalational injury in sheep .1988; 104: 208-215 Surgery 104(2): 208-215.
-
Kalay N, Ozdogru I, Cetinkaya Y, Namik Kemal Eryol, Ali Dogan, et al. (2007) Cardiovascular effects of carbon monoxide poisoning. Am J Cardiol 99(3): 322-324.
-
Ernst A, Zibrak J (1998) Carbon monoxide poisoning. N Engl J Med 339(22): 1603-1608.
-
Weaver LK, Hopkins RO, Chan KJ, Churchill S, Elliott CG, et al. (2002) Hyperbaric oxygen for acute carbon monoxide poisoning. N Engl J Med 347(14): 1057-1067.
-
Jasper BW, Hopkins R, Duker HV, Weaver LK (2005) Affective outcome following carbon monoxide poisoning: a prospective longitudinal study. Cogn Behav Neurol 18(2): 127-134.
-
Pulsipher DT, Hopkins R, Weaver LK (2006) Basal ganglia volumes following CO poisoning: a prospective longitudinal study. Undersea Hyperb Med 33(4): 245- 256.
-
Gale SD, Hopkins R, Weaver LK, Bigler ED, Booth EJ, et al. (1999) MRI, quantitative MRI, SPECT, and neuropsychological findings following carbon monoxide poisoning. . Brain Inj 13(4): 229-243.
-
Terajima K, Igarashi H, Hirose M, Matsuzawa H, Nishizawa M, et al. (2008) Serial assessments of delayed encephalopathy after carbon monoxide poisoning using magnetic resonance spectroscopy and diffusion tensor imaging on 3.0T system. Eur Neurol 59(1-2): 55-61.
-
Patton ML, Simone M, Anderson HL (1998) Successful utilization of ECMO to treat an adult burn patient with ARDS. Burns 24(6): 562-565.
-
McCunn M, Rynolds H, Cottingham CA, Scalea TM, Habashi NM (2000) Extracorporeal support in an adult with severe carbon monoxide poisoning and shock following smoke inhalation: a case report Perfusion 15(2): 169-173.
-
Kornberger E, Mair P, Oswald E, Hörmann C, Ohler K, et al. (1997) Inhalational injury treated with extracorporeal CO2 elimination . Burns 23(4): 354-359.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index