Effectiveness of Stellate Ganglion Block in Pain Management of Complex Regional Pain Syndrome (CRPS) Type II of Upper Extremity
Complex Regional Pain Syndrome (CRPS) is a Neuropathic Pain (Neu-P) Syndrome that lacks clear comprehension and could potentially have diverse causal origins. The occurrence of this syndrome following trauma is frequent, as reported in the literature. We report a patient with a history of spinal cord injury at C6/7 & C7/T1 levels in RTA, who underwent cervical spine fixation surgery, and developed hyperalgesia, allodynia, edema, and color changes in the upper limb 3-4 weeks after surgery. A multimodal therapeutic technique was implemented in the present study, incorporating a stellate ganglion block intervention, which resulted in notable benefits. These benefits included a reduction in pain scores and an improvement in mobility of the affected limb.
Introduction
The condition known as Complex Regional Pain Syndrome (CRPS) presents a multifaceted and formidable Neuropathic Pain Syndrome that poses a significant challenge to Pain Management. The genesis of Complex Regional Pain Syndrome (CRPS) may be multifactorial, with this condition being categorized into three subtypes: Type I, Type II, and CRPS-NOS (not otherwise specified), depending on the extent of nerve damage involved [1]. The following report presents a case of CRPS type II / Causalgia detected at the four-month post-trauma, potentially linked to cervicothoracic spine resection and multiple spine surgeries at the levels of C6/7 & C7/T1.
Case Presentation
A male patient, aged 28 years, was referred to our pain clinic on account of a suspected case of Complex Regional Pain Syndrome (CRPS). The individual in question presented met a roadside accident and had previously experienced hemiplegia due to spinal cord resection at the level of C7/T1 and underwent spinal fixation surgery (C7-T5). Upon initial evaluation by our team four months after symptom onset, the patient presented with complaints of tactile hypersensitivity, allodynia, edema, and alterations in color and temperature affecting the left forearm, wrist, and hand. Additionally, the patient exhibited an inability to perform arm pronation or supination, a lack of wrist and hand mobility, and a restriction in left shoulder movement. A physical examination yielded findings consistent with erythematous swelling and increased temperature in the left hand, wrist, and forearm of the individual in question. The presence of allodynia and hyperesthesia was elicited in response to light touch, while hyperalgesia was observed following the application of a pinprick stimulus. The measurement of muscular strength in the right wrist and hand was prevented due to the presence of significant pain. The neuropathic pain presented with characteristics of both a persistent and pulsing nature, and was subjectively rated as having a maximum intensity of 10 on a visual analog scale (VAS) when referring to the left wrist and hand region. The ascertainable indications and outward manifestations were deemed to be following the Budapest clinical diagnostic criteria for Complex Regional Pain Syndrome (CRPS).
The patient’s leukocyte count was determined to be 11,200 cells/μL, of which 74.1% were identified as neutrophils. The erythrocyte sedimentation rate measured 37 mm/hr, while the C-reactive protein concentration registered a level of 18 mg/dL. The remaining blood parameters exhibited values within the normal range. The results of needle electromyography revealed the presence of anomalous spontaneous activities, specifically a positive sharp wave and fibrillation potential, in the musculature of the left cervical paraspinal region, as well as in the triceps, extensor digitorum communis, extensor carpi radialis longus, and flexor carpi radialis muscles. The present study observed an abnormally prolonged latency of the H-reflex in the right flexor carpi radialis, measured at 25.78 ms, in comparison to the normal H-reflex latency detected in the left muscle at 23.59 ms. The nerve conduction study results indicated normal findings for the median, ulnar, and radial nerves on the left side. Our interpretation of the electrophysiological data led us to conclude that the patient was experiencing C6/7 radiculopathies. Magnetic resonance imaging (MRI) revealed a slightly herniated disc located in the central region of the right side at the C6/7 level, as depicted in Figure 5. Figure 1 is presented as a visual aid to support the academic discourse.
The utilization of Tc 99m-labeled bisphosphonates for a 3-phase bone scan revealed escalated periarticular uptake in the right wrist throughout the flow, blood pool, and delayed phases. These results were indicative of the typical features of Complex Regional Pain Syndrome (CRPS). The conclusive diagnosis arrived at was Complex Regional Pain Syndrome type II as per Budapest Criteria. The patient received physical rehabilitation alongside a pharmacological regimen consisting of gabapentin 100 mg twice daily, amitriptyline 10 mg, tramadol 37.5 mg with acetaminophen 500 mg every six hours, prednisolone 40 mg every 12 hours, and ibuprofen 600 mg as a rescue medication. However, this treatment approach resulted in no discernible analgesic effect.
The present study conducted an optimization of analgesic therapy, which included the escalation of gabapentin 300 mg (every eight hours), prolonged release tramadol 100 mg (every 12 hours), maintenance of amitriptyline 10 mg during nighttime, as well as supplementary administration of magnesium and tramadol 37.5 mg with acetaminophen 325 mg as rescue medication. The suspension of non- steroidal anti-inflammatory drugs was followed by a gradual weaning off of prednisolone. Concurrently, the proposition of a blockade of the left cervicothoracic ganglion was put forth utilizing academic prose.
On the day of the procedure, there was a substantial overlap between the reported complaints and the physical examination findings.

During the day of the intervention, the patient exhibited noteworthy wrist stiffness and consequentially reduced mobility. Specifically, the individual assumed a flexed position of the left-hand fingers, with pronounced limitation noted in the thumb flexion, as depicted by the black arrow.
The present observation reveals alterations in the coloration of the left forearm, wrist, and hand, as indicated by the blue arrow.
A left cervicothoracic Stellate Ganglion Block was executed following the guidelines set forth by the NYSORA, using a hybrid technique i.e. ultrasound guidance using IQ Butterfly Probe and fluoroscopy, while being monitored for standards compliance. The procedure was accompanied by sedation, utilizing a total quantity of 3 mg of midazolam. After cleaning the skin with cloraprep, the local Anaesthesia was administered through a 25G Hypodermic needle under the facilitation of fluoroscopy and anatomic landmarks at the C6 level.
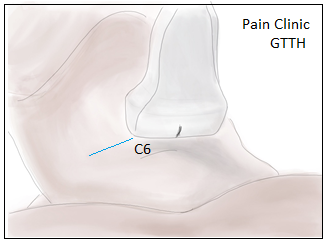
Figure 2: This study employs ultrasound imaging probe- placement play a critical role in the successful execu- tion of an ultrasound-guided stellate ganglion block.
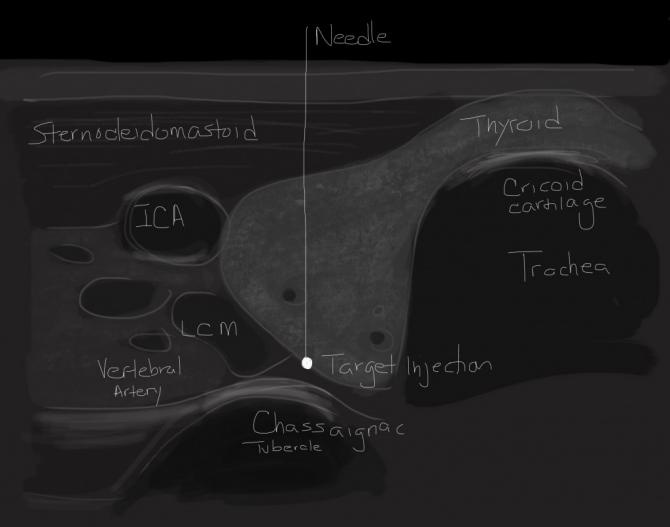
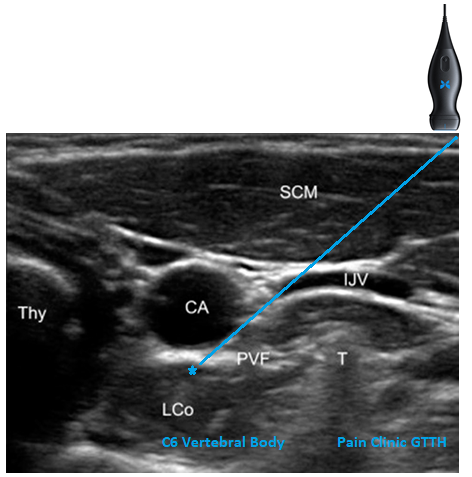
Figure 4: Ultrasound image indicating the C6 level.
Under the guidance of Ultrasound, the Locoplex 25 mm x 23G 30° bevel plexus needle manufactured by Vygon was employed to administer an injection of ropivacaine 0.2% and dexamethasone, totaling 2 mL in volume. This volume was injected into the ganglion after negative aspiration of blood and CSF, confirmation of contrast non-ionized dye spread along the ganglion, under the direct surveillance of IQ Butterfly Probe. The procedure was conducted without any notable complications. The aforementioned procedure had a collective duration of 35 minutes.
In the post-anesthesia care unit, following a lapse of thirty minutes after the procedure, a substantial reduction in the incidence of flushing as is evident from Figure 3 as well as allodynia of the forearm was discerned. Additionally, the patient demonstrated improved motor function and was observed to mobilize his hand and wrist.

Figure 6: Physical examination findings after the procedure.
After duration of thirty minutes following the implementation of the aforementioned procedure, a noteworthy decrease in the occurrence of flushness within the left forearm was observed. Concurrently, there is an observed alteration in the positioning of the left hand, characterized by decreased flexion and diminished capacity for finger abduction.
Following the intervention, a statistically significant decrease in allodynia was observed, and the patient exhibited regained ability to mobilize his left hand and wrist, which was previously unattainable.
Two hours post-procedure. The patient was released from the hospital and returned to his place of residence. After a period of 24 hours, the individual in question was re-engaged for a reevaluation, during which the treatment involving oral analgesic medication was gradually withdrawn employing a reduction of 300mg of gabapentin every 12 hours, cessation of tramadol, and continuation of amitriptyline at a dosage of 10 mg in adjunct to the implementation of a rescue medication. Following this course of action, notable improvement was observed.
After the procedure, the patient was subjected to a follow- up contact after a period of five days, wherein he was directed towards the preservance of the mobility of his left hand and regression of edema while emphasizing the requirement to raise his left arm to a level equivalent to the mouth. The sole grievance reported was a localized discomfort spanning from the elbow region to the shoulder area, albeit without necessitating analgesia or further medical intervention to alleviate the aforementioned distress.
The patient underwent observation at our pain management department three weeks following the intervention. The physical assessment was analogous to the previously delineated evaluation, and the patient expressed high satisfaction with the outcomes, leading to a favorable influence on his everyday functionality, self-governance, and general state of health. Concurrently, the individual was under the care and supervision of a physiotherapist.
Discussion
Complex Regional Pain Syndrome (CRPS) is a pathological condition that manifests as either an acute or chronic pain state. It is characterized by spontaneous or evoked regional pain which typically commences in a distal part of an extremity. The condition is distinguished by the intensity or duration of the pain, which is disproportionate compared to the expected course of pain following comparable tissue trauma [2]. The International Association for the Study of Pain put forth the suggestion of categorizing Complex Regional Pain Syndrome (CRPS) into two distinct types, namely CRPS-I and CRPS-II, based on nerve damage as per the Budapest clinical diagnostic criteria. Studies have reported the incidence rates of CRPS-I and CRPS-II to be 5.46 and 0.82 cases per 100,000 person-years in the United States, respectively. However, the proposed distinction between CRPS-I and CRPS-II based on the presence of nerve injury has faced contentions. It is generally agreed upon that despite their pathophysiological differences, clinical symptoms of CRPS-I and CRPS-II remain indistinguishable [3].
The diagnosis and management of Complex Regional Pain Syndrome (CRPS) present multifarious complexities and pose challenging difficulties in the treatment course. Both peripheral and central sensitization are implicated. The aforementioned condition can be classified as a form of chronic neuropathic pain syndrome, distinguished by discernible instances of intense to extreme pain, heightened susceptibility to pain, hypersensitivity to non-painful stimuli, abnormal swelling, unusual sensations of tingling or numbness, and irregularities in both autonomic and trophic functions. The level of pain experienced is often unrelated to the specific stimulus and typically does not conform to a particular dermatome distribution. According to the Budapest Criteria, Complex Regional Pain Syndrome (CRPS) is classified as a diagnosis of exclusion [4].
Complex regional pain syndrome (CRPS) has also been identified as a potential complication following trauma and spinal cord injuries. The precise pathophysiological mechanisms underlying the development of complex regional pain syndrome (CRPS) remain indeterminate [5]. The pathophysiological mechanisms underlying Complex Regional Pain Syndrome (CRPS) are complex and multifactorial in nature [6].
Since the underlying mechanism of CRPS type II remains indeterminate from a pathological perspective. A study previously put forth the hypothesis that a peripheral nerve injury triggers a complex array of responses involving both Wallerian degeneration and alterations in the phenotype of remaining neurons in CRPS type II [7]. These alterations result in an increased synthesis of nociceptive neurotransmitters, including substance P and calcitonin gene-related peptides, which contribute to the symptoms and signs of CRPS. In our particular case, the injury occurred at the preganglionic region of the cervical root and did not involve any instances of Wallerian degeneration.
Complex Regional Pain Syndrome (CRPS) can be distinguished from other types of chronic pain conditions due to the salient modifications observed in the autonomic and inflammatory functions within the affected region. Patients with Complex Regional Pain Syndrome (CRPS) commonly exhibit hyperalgesia and allodynia, accompanied by changes in skin color and temperature, sweating, edema, and altered hair patterns of hair, skin, or nail growth. Additionally, patients may experience reduced muscle strength, as well as tremors and dystonia of the affected limb. The diagnosis of CRPS relies on the Budapest criteria, which encompasses clinical symptoms and signs. In the present case, our patient was diagnosed with CRPS according to the Budapest criteria, based on the continuous left wrist and hand pain that was disproportionate to injury, as well as sensory (hyperesthesia, hyperalgesia, and allodynia), vasomotor (heating and erythematous skin color change), edema (swelling), and motor (weakness and decreased range of motion of the wrist) symptoms and signs observed during evaluation. Furthermore, it can be asserted that no alternative diagnosis more aptly exemplifies the aforementioned manifestations.
While there is currently no singular definitive method of diagnosis for Complex Regional Pain Syndrome (CRPS), various imaging modalities, such as radiography, thermography, computed tomography, 3-phase bone scan, and magnetic resonance imaging (MRI), have been employed to corroborate a clinical diagnosis and aid in differential diagnosis. The utilization of technetium Tc 99m-labeled bisphosphonates in a three-phasic bone scan has demonstrated notable sensitivity in detecting complex regional pain syndrome (CRPS). However, it is not entirely specific and serves a supplementary role in confirming the occurrence of CRPS [8]. A distinctive feature of three- phasic bone scans in the diagnosis of CRPS is the notable augmentation of periarticular radiotracer uptake in the affected region throughout the flow, blood pool, and delayed phases. Nonetheless, a negative result on such scans does not entirely rule out the diagnosis of CRPS. In the present study, the triphasic bone scan displayed elevated periarticular uptake in the right wrist across all three phases, which was deemed beneficial in verifying the clinical diagnosis. Following are the various techniques for effective SGB.
Ultrasound Technique
The individual is reclined in a supine position, with the neck extending slightly and the head rotating in a contralateral direction to the approached side. The preparation of the site includes cleaning and draping, followed by placement of the transducer in a perpendicular manner concerning the tracheal axis at the level of the cricoid cartilage. The transducer is then moved in a downward direction until visualization of the superior aspect of the thyroid gland is achieved. Subsequently, it is necessary to laterally reposition the transducer to acquire visual access to the anterior aspect of the Chassaignac’s tubercle located on the C6 transverse process. The structures of the carotid artery, internal jugular vein, thyroid gland, trachea, Longus colli, and Longus capitis muscle, prevertebral fascia, the root of C6 spinal nerve, and transverse process of C6 can be discerned and located, as demonstrated in Figure 1. The utilization of the Color Doppler methodology is recommended for the identification and monitoring of the anatomical location of blood vessels. Using an in-plane technique, the needle is positioned adjacent to the trachea, directed laterally towards the medial aspect. To effectively target the prevertebral fascia of the Longus colli muscle, the tip should be directed towards the region located between the posterior aspect of the carotid artery and the C6 anterior tubercle tip. It is imperative to prevent any harm inflicted on the vessels and nerves. A requisite aspiration examination is necessary to prevent the occurrence of blood or cerebrospinal fluid aspiration. This is followed by the administration of a local anesthetic, after which real-time monitoring of the spread of the injectate is undertaken.
Fluoroscopic-Guided Technique
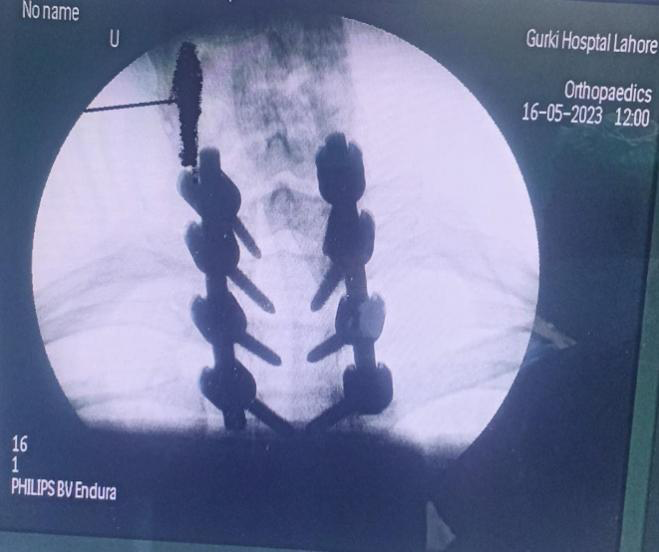
The patient is positioned supine to obtain an anteroposterior view to identify C6, which involves counting up from T1 using the C-arm. The C-arm is angled such that the superior portion of the C6 vertebral body is in alignment, following which it is rotated obliquely at an angle between 25 to 30 degrees towards the same side to capture a view of the intervertebral foramen. The objective is to identify the location at which the vertebral body and uncinate process of C6 converge. From an angled perspective, the needle is introduced in a laterally-oriented manner with a trajectory that proceeds from lateral to medial and is maintained above the vertebral body or slightly medial to prevent potential harm to spinal nerves, blood vessels, and intervertebral discs. The position must be verified utilizing both anteroposterior and lateral views. To facilitate needle localization, a minute quantity of contrast media (ranging from 0. 5 to 1 ml) may be administered initially. To further mitigate the possibility of intravascular injection, a minimal dosage of local anesthetic is initially administered. Subsequently, a volume of 10 milliliters of a regional anesthetic agent, namely lidocaine 1%, is administered via injection. The aforementioned procedure may also be executed at the cervical 7 (C7) level, however, it must be noted by physicians that there are heightened risks associated with a vascular puncture at this location.
The present case report posits a plausible correlation between the emergence of complex regional pain syndrome (CRPS) and traumatic spinal cord injury, reminiscent of similar associations documented in cervical radiculopathy [9]. Currently, there is no reported occurrence of Complex Regional Pain Syndrome (CRPS) after the administration of Transforaminal cervical epidural steroid injection [5]. Nevertheless, there is a potential correlation between the manifestation or sudden exacerbation of Complex Regional Pain Syndrome (CRPS) symptoms based on a single case report and a singular case series [10].
This scholarly case report details the manifestation of Complex Regional Pain Syndrome (CRPS) after brachial plexus injury in a patient having a predisposition for this condition owing to a former spinal cord resection at C7/T1 and having cervical spine fixation surgery post-trauma. The patient did not report experiencing central neuropathic pain after the trauma, and manifestations indicative of Complex Regional Pain Syndrome (CRPS) were only onset on the same limb, four months post-surgery.
Complex regional pain syndrome (CRPS) is characterized by a state of pro-inflammatory activity resulting from dysregulation of the immune system. The presence of autoantibodies has been identified among individuals affected by SDRC, according to recent research [11]. It has been established that the activation of alpha 1 adrenergic receptors has the potential to induce Complex Regional Pain Syndrome (CRPS) pain and dysautonomia symptoms. Conversely, the activation of beta-2 receptors and M2 anticholinergic receptors exhibit capabilities to modulate pain and inflammation response, as reported in the Peterson, et al. [12].
The development of CRPS can be attributed to a confluence of risk factors that includes nervous system sensitization, autonomic system dysregulation, and changes related to inflammatory mediators [13]. The patient exhibited manifestations of CRPS, which appears to have been triggered by the surgery, albeit being predisposed due to an earlier spinal cord resection post-trauma.
The intricate nature of Complex Regional Pain Syndrome necessitates an individualized and multimodal treatment strategy incorporating various therapeutic interventions, including pharmacological, functional, and psychological modalities. One of the treatment strategies for Complex Regional Pain Syndrome (CRPS) involves the interruption of the sympathetic innervation to the afflicted region. This intervention is based on the assumption that, in select cases, the pathophysiology of CRPS entails the involvement of the sympathetic nervous system [14].
A Stellate Ganglion Block is a technique involving the inhibition of sympathetic ganglia situated in the upper thoracic and lower cervical region. This approach is widely employed in individuals suffering from complex regional pain syndrome (CRPS). Nonetheless, there are currently no standardized protocols for patient selection or treatment.
The present case report highlights the significance of meticulous clinical medical history documentation alongside chronological events for optimal patient care. Whilst the morbidity and mortality associated with spinal cord injury have been established, the precise effects of spinal cord injury and fixation have not been conclusively established, despite its recommendation. The present case lends credence to extant literature postulating a plausible correlation between spinal fixation surgery and the onset or resurgence of Complex Regional Pain Syndrome (CRPS) symptoms.
In light of the patient’s lack of clinical progress following the adjustment of pharmacological therapy, a proposal was made for a stellate ganglion block. The procedure was successful in yielding significant improvements in pain and mobility, which were sustained and had a substantial impact on the individual’s daily activities. Stellate Ganglion Block simple injection in the neck can not only manage Causalgia but save patients’ life and misery as there are cases reported of reversal of suicidal tendency, and PTSD (combat related) by this block but this is not devoid of complications should be done by expert hand under fluoroscopy and/or ultrasound surveillance to avoid post block complications which include transient Horner Syndrome, RLN block, Phrenic Nerve Block, Brachial Plexus’s Block. Some more serious complications are Pneumothorax, Vertebral Artery or Vein puncture, Carotid Artery Puncture, Epidural or Dural puncture, Cardiac events like arrhythmias and hypotension, and some rare para tracheal hematoma, esophagus puncture, osteitis of transverse process.
Conclusions
The present case report serves to demonstrate the potential coexistence of multiple etiological factors contributing to the onset of complex regional pain syndrome in a single patient. For the assessment of etiology and the guidance of treatment, a comprehensive and chronologically arranged medical history is imperative. The present study identified a potential correlation between cervical spine fixation surgery and the onset of Complex Regional Pain Syndrome (CRPS). Stellate ganglion blockade must be exclusively carried out by Interventional Pain physicians who possess expertise in the relevant anatomical structures and possess the skill set necessary to handle any potential complications. To reduce the likelihood of complications, it is recommended to perform the procedure under ultrasound and fluoroscopic guidance. Continuous monitoring of the vital signs of patients should be a primary commitment on the part of nursing professionals. Upon the completion of the intervention, it is recommended that a thoracic radiograph and an extensive neurological evaluation be conducted. A multidisciplinary approach is requisite due to the intricacy of the subject matter and above all Interventional Pain Physicians should be capable to notify and handle all complications efficiently and timely of a block before practicing it. Dual Sympathetic Reset (DSR) is a modified form of Stellate Ganglion Block that needs randomized control trials and could be a treatment modality in the future for the treatment of Complex Regional Pain Syndrome. In conclusion, this author finds SGB very effective for CRPS II.
Conflict of Interest
None.
Funding
None.
References
-
Boas RA (1998) Sympathetic nerve blocks: in search of a role. Reg Anesth Pain Med 23(3): 292-305.
-
Cepeda MS, Lau J, Carr DB (2002) Defining the therapeutic role of a local anesthetic sympathetic blockade in complex regional pain syndrome: a narrative and systematic review. Clinical Journal of Pain 18(4): 216-233.
-
Wang JK, Johnson KA, Ilstrup DM (1985) Sympathetic blocks for reflex sympathetic dystrophy. Pain 23(1): 13- 17.
-
Kozin F (1992) Reflex sympathetic dystrophy: a review. Clinical and Experimental Rheumatology 10(4): 401- 409.
-
Price DD, Long S, Wilsey B, Rafii A (1998) Analysis of peak magnitude and duration of analgesia produced by local anesthetics injected into sympathetic ganglia of complex regional pain syndrome patients. Clin J Pain 14(3): 216-226.
-
Datta R, Agrawal J, Sharma A, Rathore VS, Datta S, et al. (2017) A study of the efficacy of stellate ganglion blocks in complex regional pain syndromes of the upper body. J Anaesthesiol Clin Pharmacol 33(4): 534-540.
-
Narouze S (2014) Ultrasound-guided stellate ganglion block: safety and efficacy. Curr Pain Headache Rep 18(6): 424.
-
Imani F, Hemati K, Rahimzadeh P, Kazemi MR, Hejazian K, et al. (2016) Effectiveness of Stellate Ganglion Block Under Fluoroscopy or Ultrasound Guidance in Upper Extremity CRPS. J Clin Diagn Res 10(1): 9-12.
-
Chang KV, Lin CP, Hung CY, Özçakar L, Wang TG, et al. (2016) Sonographic Nerve Tracking in the Cervical Region: A Pictorial Essay and Video Demonstration. Am J Phys Med Rehabil 95(11): 862-870.
-
Bhatia A, Flamer D, Peng PW (2012) Evaluation of sonoanatomy relevant to performing stellate ganglion blocks using anterior and lateral simulated approaches: an observational study. Can J Anaesth 59(11): 1040- 1047.
-
Chang KV, Wu WT, Özçakar L (2018) Ultrasound-Guided Interventions of the Cervical Spine and Nerves. Phys Med Rehabil Clin N Am 29(1): 93-103.
-
Peterson K, Bourne D, Anderson J, Mackey K, Helfand M, et al. (2017) Evidence Brief: Effectiveness of Stellate Ganglion Block for Treatment of Posttraumatic Stress Disorder (PTSD). Department of Veterans Affairs, Washington DC, USA, pp: 199.
-
Wei K, Feldmann RE, Brascher AK, Benrath J (2014) Ultrasound-guided stellate ganglion blocks combined with pharmacological and occupational therapy in Complex Regional Pain Syndrome (CRPS): a pilot case series ad interim. Pain Med 15(12): 2120-2127.
-
Mulvaney SW, Lynch JH, Hickey MJ, Rahman-Rawlins T, Schroeder M, et al. (2014) Stellate ganglion block used to treat symptoms associated with combat-related post- traumatic stress disorder: a case series of 166 patients. Mil Med 179(10): 1133-1140.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index