Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
Among critical illnesses with a mortality rate exceeding 50%, one of the prominent pathologies is acute respiratory distress syndrome (ARDS) of the lungs. The historical development of this pathology, its etiopathogenic characteristics, diagnostic criteria, and optimal modes of mechanical ventilation remain relevant topics. We decided to explore and illuminate modern perspectives on acute lung injury (ALI) and the progression to acute respiratory distress syndrome (ARDS) by reviewing local and international literature sources. Our study addresses the etiology, epidemiology, pathogenesis, diagnostic methods, prevention, and treatment of acute respiratory distress syndrome (ARDS). According to statistical data, the incidence of acute respiratory distress syndrome (ARDS) ranges from 1.5 to 88 cases per 100,000 people per year. Depending on etiology and diagnostic criteria, the global mortality rate from ARDS reaches 30-60%. Respiratory failure occurs in 3-15% of surgical patients, and in 25% of cases, sepsis is considered the cause of acute respiratory distress syndrome (ARDS). The measurement of the “Oxygenation or Carrico index” (PO2/FiO2) plays a significant diagnostic role in studying tissue hypoxia and choosing appropriate ventilation methods: when PO2/FiO2 is
Abbreviations
ARDS: Acute Respiratory Distress Syndrome; ALI: Acute Lung Injury; ASV: Requiring Artificial Ventilation.
Introduction
Acute Respiratory Distress Syndrome (ARDS) has become a focus of attention not only for clinicians but also for scientists of various specialties, including pathologists, pathophysiologists, morphologists, and those involved in clinical and experimental medicine. The relevance of this problem has been increasingly discussed worldwide, especially since the COVID-19 pandemic [1, 2].
ARDS is a severe complication of acute respiratory diseases. It is a non-specific response of the respiratory system triggered by various pro-inflammatory agents, resulting in hypoxemic respiratory failure in the absence of signs of cardiogenic pulmonary edema [1, 2, 3]. ARDS can develop due to both primary and secondary lung injuries. Its morphological manifestation is parenchymal edema caused by systemic inflammatory response and increased capillary permeability in the pulmonary circulation [2].
ARDS was first identified in 1967 in a 12-year-old patient, and mortality was recorded in 7 out of 10 cases presenting with ARDS [3]. The syndrome develops rapidly; within 12–48 hours, the inflammatory process affects the lung parenchyma, requiring artificial ventilation (ASV). During the early hours, patients experience shortness of breath, cough, chest pain, and it is characterized by a high mortality rate.
Historical review of the literature reveals that during the Vietnam War, American doctors encountered respiratory failure in some injured patients 2–3 days after recovering from severe traumatic shock. Since then, this clinical syndrome, accompanied by high mortality, has been a subject of research.
It was found that ARDS can develop not only after trauma but also as a result of sepsis, aspiration of gastric contents, massive blood transfusion, and other conditions. The syndrome has also been referred to as “shock lung” and “post-perfusion lung”. Starting in the 1960s and 1970s, authors from various countries provided information on acute respiratory failure syndrome and its clinical manifestations during critical conditions such as severe blood loss, mechanical trauma, sepsis, and cardiopulmonary resuscitation [3, 4].
| Indicator | Value | Score | |
|---|---|---|---|
| Chest x-ray | Alveolar consolidation | No alveolar consolidation | 0 |
| Chest x-ray | Alveolar consolidation | Alveolar consolidation in one quadrant of the lungs | 1 |
| Chest x-ray | Alveolar consolidation | Alveolar consolidation in two squares of the lungs | 2 |
| Chest x-ray | Alveolar consolidation | Alveolar consolidation in three quadrants of the lungs | 3 |
| Chest x-ray | Alveolar consolidation | Alveolar consolidation in the four quadrants of the lungs | 4 |
| Hipoxemia | PaO2/FiO2 | ≥ 300 | 0 |
| Hipoxemia | PaO2/FiO2 | 225-299 | 1 |
| Hipoxemia | PaO2/FiO2 | 175-224 | 2 |
| Hipoxemia | PaO2/FiO2 | 100-174 | 3 |
| Hipoxemia | PaO2/FiO2 | < 100 | 4 |
| Compliance of the respiratory system (ml/cm H2O) (in mechanical ventilation) | Compliance | ≥ 80 | 0 |
| Compliance of the respiratory system (ml/cm H2O) (in mechanical ventilation) | Compliance | 60-79 | 1 |
| Compliance of the respiratory system (ml/cm H2O) (in mechanical ventilation) | Compliance | 40-59 | 2 |
| Compliance of the respiratory system (ml/cm H2O) (in mechanical ventilation) | Compliance | 20-39 | 3 |
| Compliance of the respiratory system (ml/cm H2O) (in mechanical ventilation) | Compliance | ≤ 19 | 4 |
| Positive expiratory pressure (cmH2O) (in mechanical ventilation) | Positive expiratory pressure | ≤ 5 | 0 |
| Positive expiratory pressure (cmH2O) (in mechanical ventilation) | Positive expiratory pressure | 06-Aug | 1 |
| Positive expiratory pressure (cmH2O) (in mechanical ventilation) | Positive expiratory pressure | 09-Nov | 2 |
| Positive expiratory pressure (cmH2O) (in mechanical ventilation) | Positive expiratory pressure | Dec-14 | 3 |
| Positive expiratory pressure (cmH2O) (in mechanical ventilation) | Positive expiratory pressure | ≥ 15 | 4 |
| Total points | The presence of lung damage | No lung damage | 0 |
| Total points | The presence of lung damage | Moderate lung damage | 0.1-2.5 |
| Total points | The presence of lung damage | Severe lung damage | >2.5 |
Table 1: The extent of lung damage.
In 1967, Ashbaugh DG, et al. [5] first described symptoms such as shortness of breath, diffuse alveolar infiltration, and edema as “stiff lung”; Hardaway RM and Norlander O referred to the pathological process as “shock lung”; Collins JA called it “septic lung”; and Shumer N along with Korolev BA and Shmerelson MB, termed it “post-perfusion lung syndrome” or “hypoventilation dyspnea.” According to statistical data, the incidence of ARDS varies from 1.5 to 88 cases per 100,000 population annually. In the United States, the prevalence is 78.9 cases per 100,000 population per year, with a high number of hospital bed-days attributed to these patients. Depending on etiology and diagnostics, global mortality from ARDS ranges from 30% to 60% [5]. Among patients treated in the Department of Anesthesiology and Intensive Care for various conditions, particularly surgical diseases, 3–15% develop respiratory failure, with ARDS being a primary cause. In 25% of cases, sepsis leads to ARDS [6, 7, 8, 9, 10].
In 1988, Murray JF and colleagues utilized expanded criteria for ARDS to assess the physiological severity of the lesion, distinguishing between the acute and chronic phases of the condition, and identifying the primary cause of lung injury, as outlined in Table 1. Based on etiopathogenetic factors, the American-European Consensus Conference (AECC) in 1992 proposed a unified perspective on ARDS. They defined it as an acute and persistent inflammatory process in the lungs, characterized by increased vascular permeability in the pulmonary circulation, leading to lung parenchymal damage and hypoxemia [11, 12].
According to the AECC, ARDS is an acute condition marked by bilateral infiltration and severe hypoxemia in the absence of signs of cardiogenic pulmonary edema. Researchers noted that a PaO2/FiO2 ratio of <300 mmHg indicates acute lung injury, a ratio of <200 mmHg signifies ARDS, and <18 mmHg reflects capillary obstruction in the lungs.
| Time interval | The onset of the syndrome (symptoms of lung damage) occurs one week after exposure to a known factor. | ||
|---|---|---|---|
| Visualization of chest organs | Bilateral opacities occur that cannot be explained by effusion, atelectasis, or nodules. | ||
| The mechanism of edema | Shortness of breath cannot be explained by heart failure or fluid overload. If there are no risk factors for heart failure, echocardiography should be done first. | ||
| Hipoxemia | Light | Medium | Heavy |
| 200 mm.Hg< PaO /FiO ≤300 2 2 mm.Hg; CPAP≥5 sm Н О 2 | 100mm.Hg<PaO /FiO ≤ 200 2 2 mm.Hg; CPAP ≥ 5 sm Н О 2 | PaO /FiO ≤ 100 mm.Hg 2 2 CPAP ≥ 5 sm Н О 2 |
- Directly affecting the lungs (pulmonary origin)
- Not directly affecting the lungs (extrapulmonary origin)
- More common
- • lung infection (non-aspiration pneumonia, cytomegalovirus infection)
- • aspiration pneumonia caused by aspiration with liquids
- (gastric juice, liquid hydrocarbons).
- • inhalation with toxic substances (high concentration of oxygen, smoke, nitrogen dioxide, ammonium compounds, cadmium, chlorine, phosgene)
- • pulmonary contusion
- • fat embolism
- • radiation pneumonitis
- • pulmonary embolism
- • suffocation
- • reperfusion syndrome
Table 3: Causes of acute lung injury and ARDS.
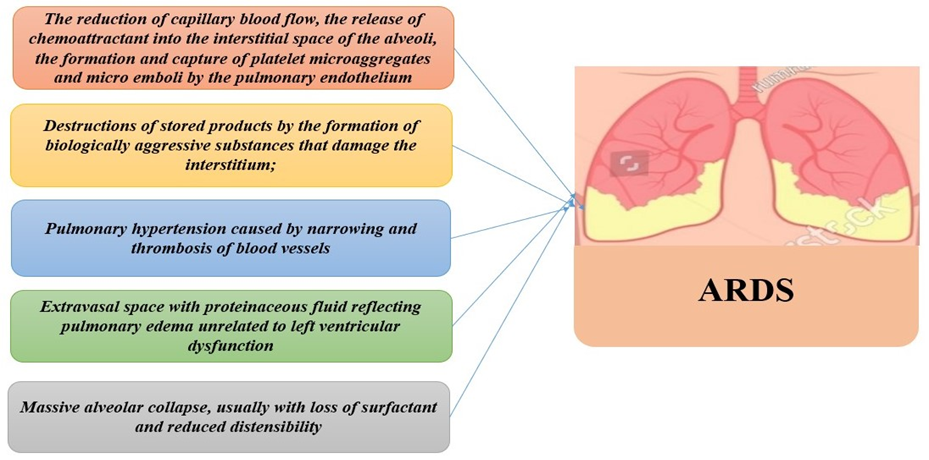
In 2012, a group of researchers from Berlin revised the definition of ARDS. The results of the ARDS Definition Task Force, which developed the new definition, were published on the JAMA website [13] (Table 2). The European Society of Intensive Care Medicine, the American Thoracic Society, and the Society of Critical Care Medicine adopted the Berlin criteria for ARDS. In 55% of cases, ARDS originates from pulmonary causes, 20% from extrapulmonary causes, 21% from mixed causes, and in 4% of cases, the etiology remains unidentified (Table 3) [14].Regardless of the cause, certain aspects of the pathogenesis of lung parenchymal lesions remain controversial, and the causes of ARDS development are illustrated in Figure 1.
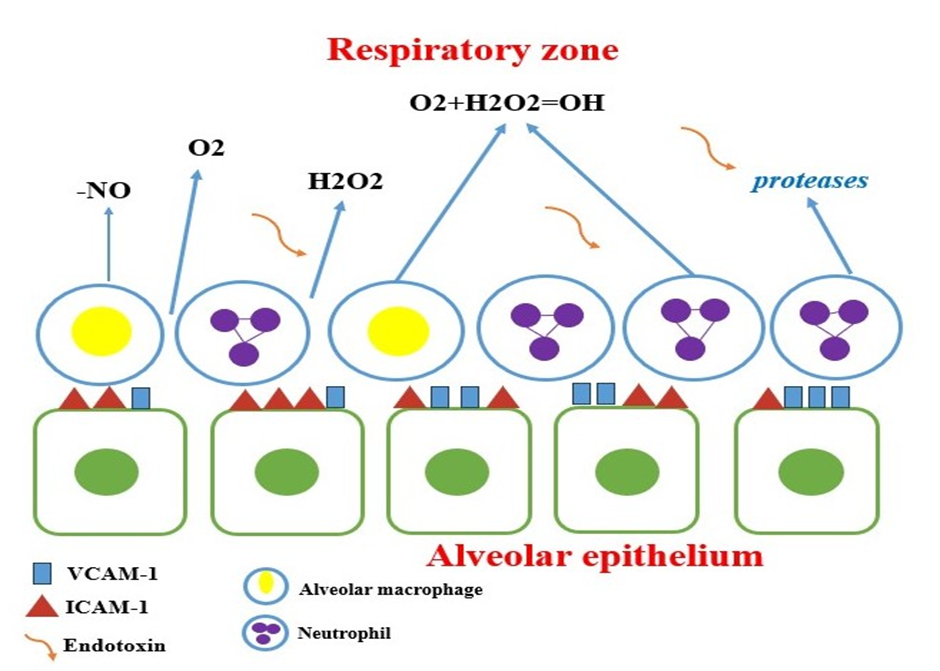
One of the key factors in the etiopathogenesis of ARDS is the accumulation of neutrophils in the lungs, leading to leukocyte activation and the production of pro- inflammatory mediators from various cellular sources. This causes both local and systemic tissue damage, while anti-inflammatory cytokines contribute to the development of pulmonary fibrosis. Pro-inflammatory substances, along with factors involved in the secretion of mediators, cytokines, immunoglobulins, and chemokines, initiate the inflammatory process in the lungs in response to exogenous and endogenous stress factors affecting the epithelial cells of the lower respiratory tract. Intracellular adhesion molecules (ICAM-1), which are normally present in small amounts in endothelial cells, play a critical role in the accumulation and activation of polymorphonuclear leukocytes in the lungs and their subsequent extravasation with the involvement of β2 integrins. During ARDS, particularly in septic conditions, ICAM-1 concentrations increase. Proteases and oxidizing agents produced by activated leukocytes and macrophages play a significant role in the damage to the alveolar-capillary membrane (Figure 2).
ARDS arises as either primary, associated with direct lung injury, or secondary, caused by indirect injury. It progresses through three stages: • Exudative Phase (onset of inflammation): This phase is characterized by damage to the endothelial cells of the lungs and alveolar epithelial cells, leading to the formation of hyaline membranes and local thrombosis. These changes disrupt gas diffusion across the alveolar- capillary membrane, resulting in the development of hypoxemia.
• Proliferative Phase: Marked by hyperplasia of type II alveolar cells, fibroblasts, and myofibroblasts, this phase leads to the thickening of the alveolar septa and the transformation of alveolar hemorrhagic exudate into cellular granulation tissue. A pathognomonic feature of this phase is the differentiation of type II alveolar cells into type I alveolar cells.
• Fibrotic Phase: This stage involves lung remodelling with the development of diffuse and focal fibrosis.
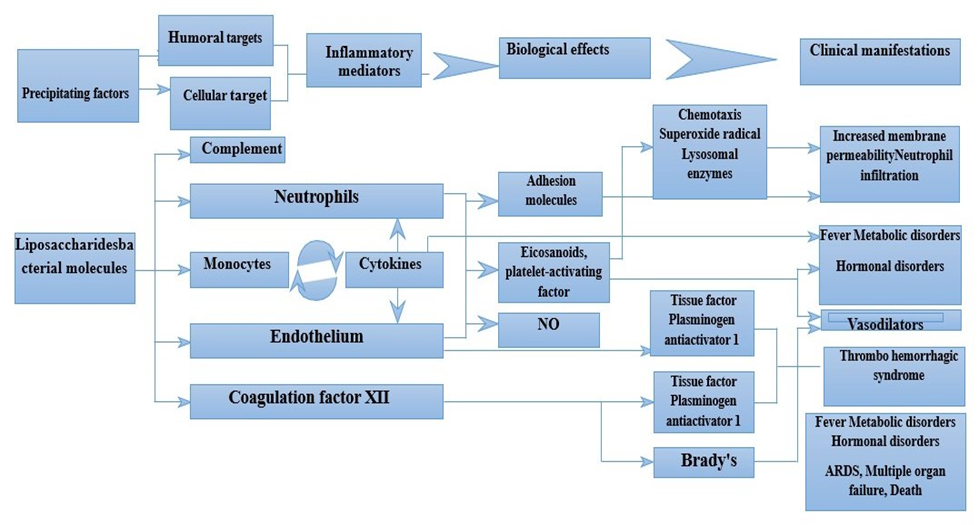
Results from experimental studies show that during the initial hours following the onset of injury, interstitial and alveolar edema and systemic inflammatory responses develop. According to A. Golubev and colleagues (2005), pulmonary edema and systemic inflammatory response form the pathogenetic basis of acute lung injury, as illustrated in Figure 3 [15, 16].
Clinical Presentation of ARDS
ARDS can be divided into four clinical stages
Stage I (1-2 days): Depending on the clinical features, the primary cause, and severity, this is referred to as the “light interval” period, covering the time from the onset of the disease to the development of hypoxemia. Symptoms of ARDS begin approximately 12 hours after onset and are accompanied by respiratory failure, tachypnea, tachycardia, and hypertension.
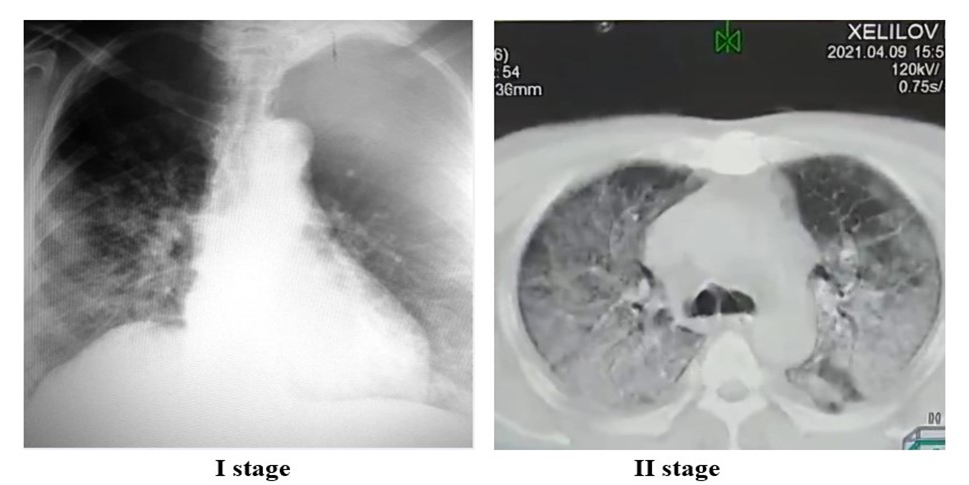
Radiologically, deformation of the pulmonary pattern may be observed against a background of increased pulmonary markings. Fine focal shadows can be noted in the peripheral regions (Figure 4).
Stage II (2-3 days): The patient’s condition progressively worsens. Depressed consciousness, up to drowsiness, and inspiratory dyspnea involving accessory respiratory muscles develop. Auscultation reveals harsh breathing and dry rales in the lungs. Oxygen inhalation helps manage hypoxemia. Radiologically, the deformation of the pulmonary pattern increases against a background of reduced pulmonary transparency (Figure 4).
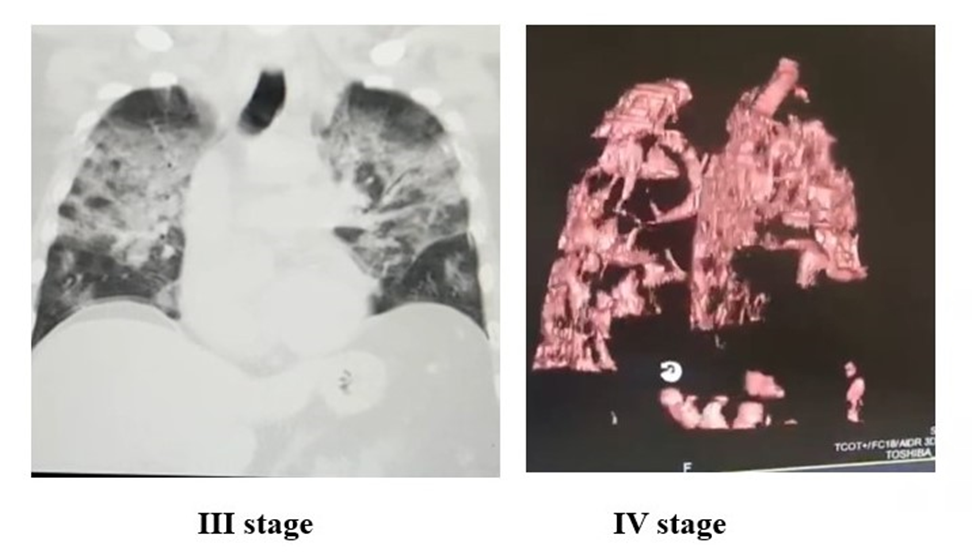
Stage III (4-5 days): Symptoms of severe respiratory failure dominate at this stage, requiring respiratory support. Auscultation reveals wet rales, and hypoxemia develops. The PaO2/FiO2 ratio drops to <200 mmHg. Radiologically, reduced lung transparency with “lobe-shaped” opacities is detected (Figure 5). Stage IV: Consciousness is depressed to the level of coma, and multiple organ failure develops. The PaO2/FiO2 ratio falls to <100 mmHg. Radiologically, “snowstorm” opacities are observed (Figure 5).
Approaches to ARDS Treatment
The primary goals in the treatment of ARDS are to support respiration, reduce hypoxemia, and suppress inflammatory processes. The cornerstone of ARDS intensive therapy is respiratory support. Additionally, infusion therapy, nutritional support, sedation, and muscle relaxation must be carefully managed. Treatment of comorbidities is also crucial [17].
• Mechanical Ventilation: Low tidal volume ventilation strategies help prevents alveolar over distension. This method is significant in reducing hypoxemia and hypercapnia. • Prone Positioning: Prone positioning enhances oxygen delivery to larger lung areas, improving oxygenation.
**
- Extracorporeal Membrane Oxygenation (ECMO): Used in severe cases to support lung function.
- Respiratory Support**
- The choice of oxygen therapy depends primarily on the presence of spontaneous ventilation and arterial oxygen concentration. **
- Non-invasive Ventilation: For patients at high risk of developing hypoxemic respiratory failure but not requiring invasive ventilation, non-invasive methods such as CPAP or BiPAP are used via nasal cannula or face mask. These methods are most effective in the early stages of ARDS, with CPAP being preferred [18].
- Invasive Mechanical Ventilation:** Tracheal intubation and invasive mechanical ventilation are required if ARDS progresses or respiratory failure becomes decompensated.
- Indications for Tracheal Intubation and Mechanical Ventilation In cases of progressive or decompensated respiratory failure, invasive mechanical ventilation is the only effective method of respiratory support. Key parameters for safe mechanical ventilation include: peak airway pressure ≤ 35 cm H2O; tidal volume 6-8 ml/kg; respiratory rate and minute ventilation to maintain PaCO2 between 30-40 mmHg; peak inspiratory flow rate 40-90 L/min; Inspiration/expiration ratio of 1.5:1; minimum required FiO2 to ensure adequate arterial oxygenation; optimal PEEP to maximize oxygen delivery to tissues while minimizing FiO2 [19, 20]. Prone positioning of patients in bed during ARDS management has been shown to improve the oxygenation index by 30-40%. However, studies suggest this method may lead to central hemodynamic disturbances, increased intracranial pressure, and tracheobronchial obstruction. While randomized studies indicate that kinetic therapy improves oxygenation, it does not enhance survival rates [21, 22, 23].
Conclusion
ARDS is associated with an inflammatory reaction that damages the alveolar-capillary membrane, leading to non- cardiogenic pulmonary edema, reduced lung compliance, increased shunting in the pulmonary circulation, and severe respiratory failure. Regardless of its etiology, the morphological changes in the lungs, clinical course, and treatment strategies are similar. Respiratory support remains the cornerstone of therapy, allowing the body to survive the acute phase of inflammation and facilitating the recovery of lung parenchyma with favourable outcomes. In recent years, protective ventilation with pressure-limited strategies has significantly improved the prognosis of ARDS patients. ARDS, characterized by a high mortality rate, is a complex and multifactorial syndrome requiring timely and effective treatment. Current treatment options are aimed at alleviating symptoms but are limited in addressing underlying causes. Therefore, a deeper understanding of ARDS pathophysiology and the development of new therapeutic approaches are needed. While the literature provides extensive information on ARDS pathophysiology and treatment, further research could open new perspectives for more effective management and prevention of this syndrome.
References
-
Akalaev RN, Sabirov DM, Rosstalnaya AL, Dadaev HH (2013) Effect of different modes of artificial ventilation on the development of acute lung injury in patients with severe combined trauma. Bulletin of emergency medicine 3: 10.
-
Akalaev RN, Sabirov DM, Sharipova V, Rosstalnaya AL (2013) High-frequency ventilation of the lungs: new is a well-forgotten old. Bulletin of emergency med 4: 100- 106.
-
Akalaev RN, Savilov PN, Stopnitsky AA, Rosstalnaya AL (2014) Controversial issues of hyperbaric medicine. Bulletin of emergency medicine 4: 84-87.
-
Arulkumaran N, Green J, Khan A, Bonnici T, Longobardo A, et al. (2021) Influence of respiratory and inflammatory parameters preceding intubation on survival of patients with COVID-19 ARDS-A single center retrospective analysis. J Crit Care 62: 289-291.
-
Ashbaugh DG, Bigelow DB, Petty TL, Levine BE (1967) Acute respiratory distress in adults. Lancet 2: 319-323.
-
Belice T, Demir I (2020) The gender differences as a risk factor in diabetic patients with COVID-19. Iran J Microbiol 12: 625-628.
-
Bi Q, Wu Y, Mei S, Ye C, Zou X, et al. (2020) Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: a retrospective cohort study. Lancet Infect Dis 20: 911-919.
-
Burki TK (2020) Coronavirus in China. Lancet Respir Med 8: 238.
-
Glumcher FS (2004) Acute respiratory distress syndrome: definition, pathogenesis, therapy. Art of treatment 9(15): 12-17.
-
Golubev AM, Moroz VV, Lysenko DV (2005) Acute lung injury caused by microvascular thrombosis. General reanimatology 1(3): 17-20.
-
Hajjar LA, Costa IBSDS, Rizk SI, Biselli B, Gomes BR, et al. (2021) Intensive care management of patients with COVID-19: a practical approach. Ann Intensive Care 11: 36.
-
Kassil VL, Zolotokrylina ES (2003) Acute respiratory distress syndrome. Moscow: Med, pp: 224.
-
Kirov MY, Kuzkov VV, Nedashkovsky EV (2004) Acute lung injury in sepsis: pathogenesis and intensive care. Arkhangelsk, pp: 96.
-
Krylov VV, Talypov AE, Puras V (2014) Decompressive craniotomy in severe traumatic brain injury. Novoye Vremya, pp: 272.
-
Li X, Ma X (2020) Acute respiratory failure in COVID-19: is it “typical” ARDS? Crit Care 24: 198.
-
Magrupov BA, Vervekina TA, Ubaydullaeva VU, Yuldashev FA (2014) Morphological aspects of adult respiratory distress syndrome. Bulletin of emergency medicine 4: 96-99.
-
Pfortmueller CA, Spinetti T, Urman RD, Luedi MM, Schefold JC (2021) COVID-19-associated acute respiratory distress syndrome (CARDS): current knowledge on pathophysiology and ICU treatment - a narrative review. Best Pract Res Clin Anaesthesiol 35: 351-368.
-
Ranieri VM, Rubenfeld GD, Thompson BT, Caldwell E, Fan E, et al. (2012) Acute respiratory distress syndrome: the Berlin Definition. JAMA 307(23): 2526-2533.
-
Roshanshad A, Kamalipour A, Ashraf MA, Roshanshad R, Jafari S, et al. (2020) The efficacy of remdesivir in coronavirus disease 2019 (COVID-19): a systematic review. Iran J Microbiol 12: 376-387.
-
Sabirov DM, Khodzhaev R, Akalaev RN (2014) Mechanical ventilation-induced lung injury. General reanimatology 10(6): 24-31.
-
Vlasenko AV (2005) Acute parenchymal lung injury in patients with traumatic brain injury after blood transfusions and aspiration syndrome. Fundamental problems of resuscitation 4: 4-30.
-
Voitkovskaya KS, Chernyaev AL (2012) Acute lung injury syndrome: definition, pathogenesis, experimental models and the role of mesenchymal stem cells in the treatment of animals. Bulletin of modern clinical medicine 5(2): 60-67.
-
Wu C, Chen X, Cai Y, Xia J, Zhou X, et al. (2020) Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med 180: 934- 943.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index
- The Diverse Roles of Anaesthesiologists and Ambulance Services