Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
Kyphosis, an excessive convex spinal curvature, complicates anaesthetic management due to respiratory and cardiovascular limitations. Severe cases increase the risk of difficult airway management and post-operative complications. A 77-year-old female with severe thoracic kyphosis and stage 5 CKD on hemodialysis presented with a swollen right brachiocephalic fistula. Her deformity prevented supine positioning, requiring anaesthetic modifications. Given the anticipated difficult airway, a comprehensive emergency plan was implemented. The patient was positioned in a semi-Fowler (30-degree head-up tilt) position, and a second-generation supraglottic airway device (ProSeal) was successfully inserted. She remained hemodynamically stable, with mild post-operative wheezing managed by nebulization. She was discharged on the second postoperative day without complications. Severe kyphosis distorts airway anatomy, limiting neck mobility and complicating intubation. Supraglottic airway devices offer a safe alternative in such cases. Comorbid conditions like COPD heighten the risk of post-operative respiratory issues, requiring close monitoring. Anaesthetic management of severe kyphosis demands early recognition, meticulous preparation, and alternative airway strategies. Supraglottic airway devices provide a safe and effective option, emphasizing the need for individualized perioperative planning and teamwork.
Abbreviations
BD: Twice Daily; CKD: Chronic Kidney Disease; COPD; Chronic Obstructive Pulmonary Disease; FEV: Forced Expiratory Volume In 1, FVC: Forced Vital Capacity.
Background
Kyphosis, an excessive convex curvature of the spine, primary affecting the thoracic and sacral regions, with a prevalence ranging from 0.3% to15.3% [1]. This musculoskeletal disorder presents significant challenges in anaesthetic management due to their limited respiratory and cardiovascular functions.
Severe kyphosis causes difficulty in both general and central neuraxial anaesthesia. It can create significant challenges for anaesthesiologists due to potential difficulties with airway management, cardiovascular and respiratory complications post operatively.
Case Report
A 77-year female with stage 5 chronic kidney disease (CKD) on two times a week maintenance hemodialysis presented with a two-week history of right brachiocephalic fistula swelling, associated with pain and restricted mobility.
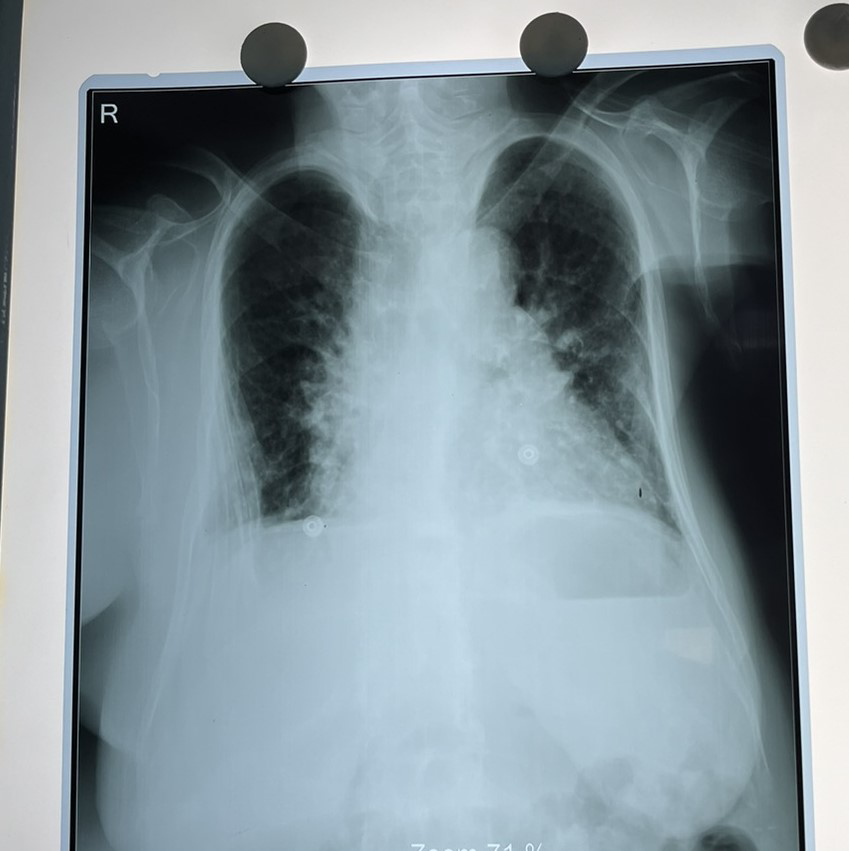
She had severe thoracic hyperkyphosis with a pronounced hunch back deformity progressing over the past 40 years, so she was unable to lie supine. The patient had a body mass index of 16.6 kg/m2 (height- 145cm, weight-35kg).

Medical History
- Hypertenion - Tablet Amlodipine 5 mg BD, Tablet Torsemide 100 mg BD
- Chronic obstructive pulmonary disease (COPD)- Regular Rotahaler therapy (Budesonide/ formoterol and Tiotropium bromide) BD
Pre-operative assessment
• Functional Status: METS<4 • Vitals: Heart rate 80 beats per minute, respiratory rate of 16 breaths per minute and blood pressure was 160/100 and oxygen saturation of 94% in room air. • On Respiratory Examination: Bilateral equal air entry with normal vesicular breath sound heard. • Cardiovascular examination was normal.
Airway examination
- Modified Mallampati grade was III with normal mouth opening.
- Temporomandibular joint distance :5 cm.
- Restricted neck extension (20 degrees) with normal neck flexion. **
- Upper lip bite test:** Grade 2.
Investigations
• Pulmonary Functional Status: forced expiratory volume in 1 s (FEV1) of 1.64 L (65% of normal), forced vital capacity (FVC) of 1.9L (66 % of normal) and an FEV1/FVC ratio of 86 %. • Echocardiograph: Moderate mitral regurgitation with mild tricuspid regurgitation with left ventricle ejection fraction of 60%.
Anaesthetic Management
• Fasting status of patient was confirmed. Patient and patient family were counselled about the anaesthetic considerations and a written informed consent was obtained. Given the high risk of the difficult airway management, an emergency airway cart with and fibre optic bronchoscope and front-of-neck access was prepared. In preoperative period, nebulisation was done with salbutamol and ipratropium bromide. After taking the patient to operating room, all the ASA 2 monitors were attached. • Position: Semi-Fowler (30-degree head -up-tilt) due to inability to lie supine. • Vascular Access: 7 Fr 3 lumen central venous catheter in right internal juglar vein under ultrasound guidance following a cervical plexus block. • Induction: Fentanyl and titrated propofol . • Airway Management: A second-generation laryngeal mask airway (ProSeal size 3) was successfully inserted on the first attempt. • Surgical Duration: 1 hour, hemodynamically stable throughout, trachea was exubated once the extubation criteria was fulfilled. • Post-Operative Complication: Bilateral wheezing, managed with nebulisation (salbutamol and ipratropium bromide). • Outcome: Discharged on the second post-operative day with no further complications.
Discussion
Severe kyphosis complicates airway management due to anatomical distortion, restricted neck mobility, and potential tracheal devation [2]. Supraglottic airway devices provide an effective alternative to endotracheal intubation, particularly in a resource limited setting. It serves as a great challenge for both securing airway and central nueuraxial block.
Difficult Airway
**
- Face-To-Face Intubation: Viable option in kyphotic patients who cannot lie supine. Light and is a lighted stylet that uses the principle of transillumination of the soft tissues of the anterior neck to guide the tracheal tube into the trachea [3].
- Supraglottic Airway Devices: Offers a high success rate (65%-100%) in anticipated difficult airway patients [4].** Laryngeal mask airway increases the speed of placement by the surgeon, improves haemodynamic stability, and presents a lower incidence of sudden cough and postoperative sore throat compared to the endotracheal intubation [4].
- Coexisting respiratory infections and comorbidities like COPD make extubation challenging and more susceptible to need of post-operative mechanical ventilation and respiratory infections.
- Post-operative respiratory challenges were anticipated, emphasizing the need for vigilant monitoring and prompt intervention.
Conclusion
Severe kyphosis presents significant airway and anaesthetic challenges. Successful management requires early recognition, meticulous preparation, alternative airway strategies and team work. Supraglottic airway devices offer a safe and effective solution, particularly in patients unable to tolerate supine position.
Declaration of Patient Consent
The author confirms that informed consent was obtained from the patient for publication of clinical details and images. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
-
Saracoglu KT, Baygın O, Kafali IH (2015) Kyphoscoliosis and difficult airway management. Istanbul Bilim Universitesi Florence Nightingale Tıp Derg 1(1): 43-47.
-
M DK, Joshi DA, Sathe DV, Gogna DR (2021) Anaesthetic management of a patient with severe kyphoscoliosis with left psoas abscess. Int J Med Anesthesiol 4(3): 54- 56.
-
Jeong H, Chae M, Seo H, Yi JW, Kang JM, et al (2018) Face-to-face intubation using a lightwand in a patient with severe thoracolumbar kyphosis: a case report. BMC Anesthesiol 18(1): 92.
-
Zhang K, Zhou M, Zou Z, Zhu C, Jiang R (2024) Supraglottic airway devices: a powerful strategy in airway management. Am J Cancer Res 14(1): 16-32.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index
- The Diverse Roles of Anaesthesiologists and Ambulance Services