Indoor Air Quality, Cell Features and Lifestyle Characteristics: Implications on the Prevalence of Some Respiratory Tract Diseases and Symptoms among Inmates of Enugu Prison, Nigeria
The study assessed indoor air quality, cell features of Enugu prison and lifestyle characteristics of inmates to ascertain their possible contributions to the prevalence of some respiratory diseases and symptoms among the inmates. The prison cells recorded poor indoor air quality. Cells with 4 windows had highest concentration of the indoor air pollutants [formaldehyde (0.20±0.07 mg/m3), total volatile organic compounds (0.79±0.37 mg/m3), and particulate matter, PM1 (71.03±41.09 μg/m3), PM2.5 (89.00±49.66 μg/m3) and PM10 (107.40±61.86 μg/m3)], as well as highest incidence of the symptoms/infections [cough (62.5%), wheeze (37.5%), chest pain (41.7%), pneumonia (25.0%) and bronchitis (33.3%)] than the cells with < 4 windows and > 4 windows. All smokers had symptoms of respiratory tract infections. Cell features and lifestyle characteristics were contributing factors in the air pollution and the prevalence of some respiratory tract diseases/symptoms. The findings can be useful in non-medical intervention towards proper management of the inmates’ respiratory health.
Introduction
Rumchev, et al. reported that the World Health Organization (WHO) ranked indoor air quality as the eighth most important risk factors contributing to the global burden of disease and responsible for 2.7% of the global burden of disease [1]. Poor indoor air quality is implicated in many diseases and is recognized as a significant risk factor for respiratory health, especially in lower income countries and vulnerable population including prison inmates. Prison inmates spend substantial proportion of their time indoors and may become exposed to elevated levels of air pollutants. Multiple factors which may be described as macro- and micro-environmental determinants influence level of exposure to indoor air pollution. While housing characteristics are considered as micro-environmental determinants, demographic and socioeconomic factors constitute macro-environmental determinants [2]. Housing characteristics that may contribute to indoor air pollutants include structural features, fomites and occupants’ activities such as tobacco smoking, snuffing, and cooking. Smoking is considered as one of the most common indoor air pollutants which expose non-smokers to second-hand smoke.
Particulate matter (PM) is a complex mixture of extremely small particles and liquid droplets in which primary particles are emitted directly into the atmosphere such as diesel soot, while secondary particles are created through physicochemical transformation of gases such as nitrate and sulfate formation from gaseous nitric acid and sulfur dioxide, respectively. PM can be divided into coarse (10–2.5 μm; PM10–2.5), fine (<2.5 μm; PM2.5), and ultrafine (<0.1 μm; PM0.1) particles [3]. Of particular interest are PM2.5 and PM0.1 because they are the PMs that ultimately enter the lungs, although the chemical components from bigger PM could also be deposited in the alveolar cavities and penetrate into circulation [4]. PMs of aerodynamics diameter 10 μm and less, cause serious damage to tracheo-alveolar structure, often leading to hypoxia and metabolic defects.
Volatile organic compounds (VOCs) comprise of a wide spectrum of chemical compounds that may pose public health challenges. Assessment of health effects of individual volatile organic compounds is not always feasible because of the complexity of chemical compounds that are involved. Consequently, the sum of the concentrations of the individual compounds referred to as total volatile organic compounds (TOVCs) is used as an indicator for the concentration of VOCs. Anthropogenic activities such as tobacco smoking, cooking, burning of organic materials and use of personal care products contribute to indoor VOCs concentration.
Over the last two decades, indoor air quality (IAQ) has caused increasing concern due to the adverse effects that it may have on human health. Most inmates in the prisons spend up to 90% of their time in an indoor environment because of security reasons. Several effects on the respiratory system have been associated with exposure to indoor air pollution (IAP). These include acute and chronic alterations in pulmonary function, more incidence and prevalence of respiratory symptoms, exacerbation of pre-existing respiratory symptoms, and sensitization of the airways to allergens present in the indoor environment. The overcrowded prison cells create smaller indoor-air mixing volumes that allow infectious diseases to spread more easily from one person to the next. Despite the growing body of literature addressing the wide range of health impacts associated with poor indoor air quality, there is no study to our knowledge that investigated the health impact of indoor air quality and housing features on respiratory health of prison inmates in Nigerian prisons.
Materials and Methods
Study Population
One hundred and twenty one (121) inmates of Enugu prison consisting of 109 males, 11 females and 1 unspecified sex participated in the study. Protocol for the study was as previously reported [5].
Data Collection
Data collection involved two stages. In stage one a standardized health and life style survey was conducted through face-to-face interviews between researchers and inmates according to the method of the American Thoracic Society with some questions modified to reflect the local lifestyle and settings of the prison environment. Questions were structured to include demographic data, life style characteristics, and symptoms (recurrent cough, chest pain, wheeze, and breathlessness) associated with respiratory diseases, experienced in the last six months. Stage two involved indoor air quality monitoring of the prison cells.
Indoor Air Quality Assessment of the Prison Cells
Otuu FC, et al. Indoor Air Quality, Cell Features and Lifestyle Characteristics: Implications on the Prevalence of Some Respiratory Tract Diseases and Symptoms among Inmates of Enugu Prison, Nigeria. Adv Clin Toxicol 2019, 4(3): 000163.
A quantitative assessment of indoor concentrations of particulate matters (PM1, PM2.5, PM10), total volatile organic compounds (TOVCs) and formaldehyde (HCHO) was made. Measurements were conducted in the cells for approximately 8 hrs according to the method as reported by Otuu, et al. with slight modifications [6]. The monitoring equipment was positioned at about 1 m above the ground. An air quality and pollution monitor (EGVOC- 180, was used for monitoring of fine particles (PM1, PM2.5, PM10), total volatile organic compounds (TOVCs) and formaldehyde (HCHO). The monitor was calibrated following manufacturer’s instructions prior to measurements.
Statistical Analysis
Statistical analysis was performed using the IBM SPSS Version 21.0 for windows (IBM SPSS Statistics for Windows, Version 21.0 IBM Corp. Armonk, NY, USA). The critical level of significance of 5% for all statistical tests (two-tailed) was used in this study. Since the study focused on respiratory symptoms for the inmates, binary variables (0 = had no symptoms, 1 = had symptoms) were used in the assessment of respiratory disease symptoms (a runny nose and coughs, wheeze, shortness of breath, asthma, chest pain, and bronchitis).
Independent/exposure variables, including demographic factors, life style characteristics, cell environment conditions (number of windows) and indoor air pollution variables were recorded into binary or categorical variables with more than two levels.
Descriptive statistics were generated for the outcome and independent variables. Bivariate analyses, including cross-tabulations and chi-squares tests, were performed for assessing unadjusted associations between the independent/exposure variables and respiratory symptoms as outcome variables. The study was cross- sectional with common occurred health outcomes, we therefore considered a multivariable Poisson regression (MPR) analysis with robust variance estimation as ideal to examine the adjusted association (1) between respiratory symptoms and life style characteristics, and cell environment conditions, controlling for confounders (demographic factors and smoking), and (2) between respiratory symptoms and indoor air pollution as depicted by PM1, PM2.5, PM10, TOVCs and HCHO controlling for here to fore mentioned confounders. The multivariable modelling was carried out at two stages, namely a complete and reduced modelling. In the complete modelling, all variables describing life style characteristics, and cell environment conditions were included. In the supplementary reduced modelling, only those variables found to be significantly associated with the health outcomes in the univariate analysis with p < 0.1 were included. Backward elimination approach was applied to get the parsimonious final model. Crude and adjusted prevalence ratios and their 95% confidence interval (CI) are reported. Crude prevalence ratio (CPR) is reported when associations are significant but not adjusted for confounders. Only variables still significantly associated (p < 0.05 or p < 0.1) with inmates’ respiratory symptoms after controlling for confounders in the final model are reported as adjusted prevalence ratios (APR).
In addition, the association between cell characteristics, life style and indoor air quality was examined. Independent t-test or one-way ANOVA were used to investigate the difference between cells. Multivariable linear regression (MLR) analysis with a backward elimination approach was conducted to examine the effect of life style characteristics, and cell environment conditions on indoor air pollution concentrations.
Results
The study population was dominated by male (90.1%)
and their ages ranged between 18 and 81yrs
(35.01±14.09). Cells with 4 windows had highest
concentration of the parameters: HCHO (0.20±0.07
mg/m3), TVOC (0.79±0.37 mg/m3), PM1 (71.03±41.09
$$ \mu \mathrm {g} / \mathrm {m} ^ {3}), \mathrm {P M} _ {2. 5} (8 9. 0 0 \pm 4 9. 6 6 \mu \mathrm {g} / \mathrm {m} ^ {3}) \mathrm {a n d} \mathrm {P M} _ {1 0} $$
(107.40±61.86 μg/m3) (Table 1). Least concentrations
were recorded in cells with < 4 windows: HCHO
(0.10±0.05 mg/m3), TVOC (0.30±0.25 mg/m3), PM1
(27.42±4.58 μg/m3), PM2.5 (37.56±6.98 μg/m3) and PM10
(40.86±9.7 μg/m3). Comparison of the concentrations
between cells with different number of windows revealed
significant differences (p < 0.001 for each) for all the
parameters. A post-hoc test revealed the significant
difference to have existed between each pair wise
comparison in the parameters except between cells with >
4 windows and 4 windows for the concentration of PM1.
The L cells recorded the highest number of inmates with
symptoms of respiratory infections (90.0%) followed by
N ward (83.3%), H ward (66.7%), G ward (58.3%) and P
cells (56.5%).
Otuu FC, et al. Indoor Air Quality, Cell Features and Lifestyle Characteristics: Implications on the Prevalence of Some Respiratory Tract Diseases and Symptoms among Inmates of Enugu Prison, Nigeria. Adv Clin Toxicol 2019, 4(3): 000163.
| HCHO mg/m3 | TVOC mg/m3 | PM1μg/m3 | PM2.5μg/m3 | PM10μg/m3 | |
| >4 windows | 0.13±0.07 | 0.50±0.28 | 56.95±37.46 | 65.60±33.30 | 79.97±49.22 |
| 4 windows | 0.20±0.07 | 0.79±0.37 | 71.03±41.09 | 89.00±49.66 | 107.40±61.86 |
| <4 windows | 0.10±0.05 | 0.30±0.25 | 27.42±4.58 | 37.56±6.98 | 40.86±9.70 |
| Kruskal-Wallis H | 48.428 | 49.915 | 66.871 | 44.155 | 56.677 |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
Table 1: Prison cell features and air quality profile.
Inferential Statistics Used: Kruskal Wallis H Test; Post Hoc Test: Mann-Whitney Test with Bonferroni’s Correction. Table 1: Prison cell features and air quality profile.
| Cell | N | Cough | Wheeze | Chest pain | Pneumonia | Bronchitis | |
|---|---|---|---|---|---|---|---|
| >4 windows | 71 | 28(39.4) | 16(22.2) | 27(37.5) | 8(11.1) | 9(12.5) | |
| 4 windows | 24 | 15(62.5) | 9(37.5) | 10(41.7) | 6(25.0) | 8(33.3) | |
| <4 windows | 24 | 10(41.7) | 4(16.7) | 6(25.0) | 1(4.2) | 3(12.5) | |
| Statistic | 3.963+ | s | 1.667+ | 4.519* | 5.325* | ||
| p-value | 0.138 | 0.201 | 0.434 | 0.109 | 0.066 |
Table 2: Cell Features and Respiratory Health of the Inmates.
Inferential Statistics Used: Chi-Square Test for Homogeneity of Proportion (+); Fishers Exact Test (*) Table 2: Cell Features and Respiratory Health of the Inmates.
| Respiratory Tract Infection | Fishers Exact | RR | |||
|---|---|---|---|---|---|
| Smoking | No | Yes | Total | p-value | 95% C.I |
| No | 54(49.1) | 56(50.9) | 110 | 0.001 | 1.96 |
| Yes | 0(0.0) | 11(100.0) | 11 | 1.63-2.36 |
Table 3: Respiratory Tract Infection and Lifestyle Characteristics (Tobacco Smoking).
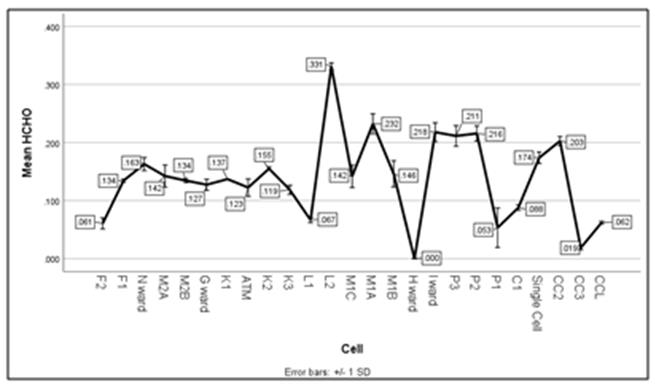
1A: HCHO concentration (mg/m3) across the cells. 1B: Concentration of TVOCs across the cells.
Otuu FC, et al. Indoor Air Quality, Cell Features and Lifestyle Characteristics: Implications on the Prevalence of Some Respiratory Tract Diseases and Symptoms among Inmates of Enugu Prison, Nigeria. Adv Clin Toxicol 2019, 4(3): 000163.
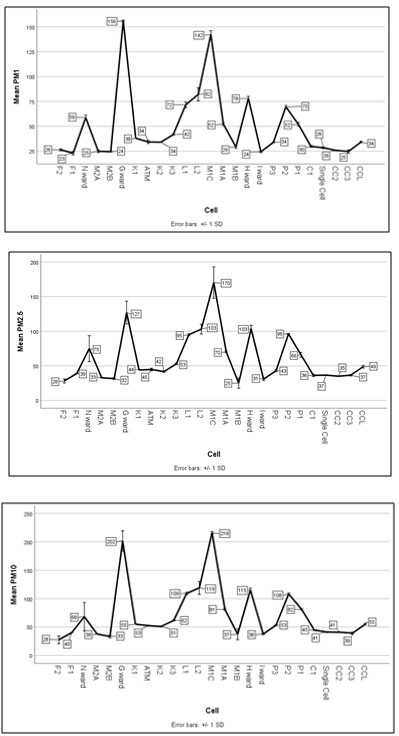
2A: PM1 concentration (μg/m3) across the cells. 2B:PM2.5 concentration (μg/m3) across the cells.
2C: PM10 concentration in (μg/m3) across the cells. Figures 1 & 2: Air Quality Profile of the prison cells P2 (108.14±1.68 μg/m3). The least concentration was recorded in cell F2 (27.67±6.75 μg/m3) (figure 1d).
Discussion
In this study we quantitatively assessed the indoor concentrations of particulate matters (PM1, PM2.5, and PM10), total volatile organic compounds (TOVCs) and formaldehyde (HCHO) by direct reading instrumentation method using hand held Air Quality Detector (EGVOC- 180). We collected information on health status and life style using a modified standardized questionnaire according to the methods in American Thoracic Society and logistic regression was used to relate IAQ to respiratory health among the inmates. Differences in the number of windows were used to assess cell features and cells were classified as 4 window cells, <4 widow cells and > 4 window cells.
Otuu FC, et al. Indoor Air Quality, Cell Features and Lifestyle Characteristics: Implications on the Prevalence of Some Respiratory Tract Diseases and Symptoms among Inmates of Enugu Prison, Nigeria. Adv Clin Toxicol 2019, 4(3): 000163.
Most of the cells recorded poor indoor air quality, especially with respect to particulate matters where the values exceeded the WHO regulatory standard values (25 μg/m3 for PM2.5 and 50 μg/m3 for PM10). L2 cell recorded the highest values of HCHO and TOVCs (0.33±0.01 mg/m3 and 1.51±0.03 mg/m3 respectively) and was associated with the more incidences of respiratory disease symptoms. This could be explained from the fact that the cell was highly congested with some inmates staying at the corridors. Demography and indoor anthropogenic activities affect indoor air quality [7]. The study of Lee, et al. implicated indoor sources as principle environmental factors affecting VOCs and HCHO levels at the elderly care centers in Korea [8]. In our study the cells (L2, M1A, and CC2) that recorded higher values of HCHO and TVOCs have contrasting features. While L2 and M1A have 4 and 6 windows respectively, and were fairly overcrowded, CC2 has only one (1) window, a female cell housing few inmates at the time of the study. The overcrowding in cells L2 and M1A could explain the high values recorded in them while the lack of cross ventilation could be the reason for the case of CC2. Overcrowding and inadequate ventilation enhance smaller indoor mixing volumes, allowing re-suspension of particulate matters, low dissipation of volatile organic compounds, more inter molecular collision of micro particles and formation of secondary compounds as well as increasing the spread of infectious diseases more easily from one person to the next.
The cells (G ward and M1C) recorded the highest concentrations of all classes of particulate matter than the other cells, followed by N and H wards. These were classified as > 4 window cells in our study and they were also overcrowded at the time of the study. Overcrowding and lifestyle characteristics seemed to be more responsible for the poor indoor quality than the cell features in our study. The cells with relatively more pollution parameters were also associated with more prevalence of the respiratory tract infection symptoms, implicating indoor air quality in the disease prevalence.
Health effects of indoor air pollutants have been addressed in several studies but only a few studies have investigated such effects with respect to environmental tobacco smoke (ETS) and structural features in the prisons, especially in the developing countries, including Nigeria [9, 10, 11, 12]. Our findings demonstrated that in wards or cells where most inmates admitted that they smoke regularly concentrations of PM2.5 and other pollutants were high. Although for some logistical reasons we were unable to carry out full 24 h monitoring, the concentrations recorded often exceeded the WHO 24h mean upper guidance limit of 25 μg/m3, (WHO, 2009). Concentrations of pollutants in male cells where smoking was considered a relaxation therapy were particularly high. Since ETS contains several thousand toxins and many carcinogens, the hazards associated with this exposure are likely to be significant [13]. Smoking in prisons is therefore a significant lifestyle characteristic with potential to cause harm to the health of smokers and non-smokers in the Enugu prison. One of the most important types of indoor pollution is from tobacco smoke, which contributes to levels of respirable particles, nicotine, polycyclic aromatic hydrocarbons, carbon monoxide, acrolein, nitrogen dioxide, N- nitrosodimethylamine, acetone, and benzene [14]. It is possible that the inhalation of cigarette smoke may injure the bronchial epithelium possibly by expanding the narrow junctions between epithelial cells, resulting in enhanced bronchial epithelial permeability. This could lead to increased penetration of antigen through the epithelial layer and the sensation of irritations that may present in different symptoms including cough and wheeze. Passive tobacco smoke is one of the most important types of exposure related to indoor air pollution and in Enugu prison cells where free tobacco abound, the health of non smoking inmates is endangered.
The finding in the present study linking the prevalence of tobacco smoking among the inmates to the prevalence of symptoms of respiratory diseases is in accordance with an earlier study of acute symptoms in nurses exposed to ETS and with several studies on ETS and chronic respiratory symptoms in adults [10, 15, 16, 17, 18]. For the inmates who spend more time in these cells than in outdoor environments, exposure to 5these air pollutants could cause adverse health effects on their pulmonary and respiratory systems. Bentayeb, et al. showed that chronic exposure to low-level indoor air pollutants, including CO, NO2, PM0.1, PM10 and HCHO, affected the increasing incidence of respiratory and cardiovascular diseases in the elderly population permanently living in nursing homes in seven European countries [19]. Tunsaringkarn, et al. also found that among the elderly in Bangkok, Thailand, indoor levels of HCHO and VOCs were significantly associated with the increase of cancer risks and respiratory disease symptoms [20]. The study of Lee, et al. implicated indoor sources as principle environmental factors affecting VOCs and HCHO levels at the elderly care centers in Korea. These reports are in agreement with our present study [8].
Otuu FC, et al. Indoor Air Quality, Cell Features and Lifestyle Characteristics: Implications on the Prevalence of Some Respiratory Tract Diseases and Symptoms among Inmates of Enugu Prison, Nigeria. Adv Clin Toxicol 2019, 4(3): 000163.
Conclusion and Recommendations
This study affirms that the risk of respiratory diseases among the Enugu prison inmates is significantly associated with exposure to low-levels of indoor air pollution, primarily generated from mainly the demographic and lifestyle characteristics but least from cell features. There is a dire need for more studies on indoor pollution and health of the inmates, and especially in the elderly inmates who are more at health risk due to other confounding geriatric complications. Future studies should address both short-term and long-term health effects related to indoor air pollutants. Identification of other cell features and life style characteristics within the prison environment that may exacerbate the susceptibility of the inmates to the adverse effects of air pollutants will also be an important step to support preventive measures. Few studies have evaluated the role of indoor pollutants in determining the prognosis of pre- existing diseases. Such studies may become an important new area for research by those concerned with prisoners’ health and well fare, given the fact that inmates are more often restricted to indoor environments with possible high levels of exposure to indoor pollutants.
There is a strong need for more studies on indoor pollutants and health in the prison, with focus on improved exposure assessment, various types of short- term and long-term health outcomes, and identification of cell features and other lifestyle characteristics associated with susceptibility to the adverse effects. Our findings thus provide strong evidence that smoking in prisons in Enugu is a source of high ETS exposure for both smoking and non-smoking prisoners and therefore the need to modify some existing policies, especially with regard to tobacco smoking inside the cells.
Authors’ contributions
FCO participated in the design and execution of the study, and drafting the manuscript. ENS participated in the statistical analysis and interpretation of data. CNO and ILS participated in the air sampling analysis. All authors participated in the final draft of the manuscript.
Acknowledgments
We acknowledge the time and effort of all participants in this study. We also like to thank and acknowledge the contributions of the prison staff for conducting the data collection.
Conflicts of Interest
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for- profit sectors.
References
-
Rumchev K, Zhao Y, Spickett J (2017) Health Risk Assessment of Indoor Air Quality, Socioeconomic and House Characteristics on Respiratory Health among Women and Children of Tirupur, South India. Int J Environ Res Public Health 14(4): 429.
-
Balakrishnan K, Ramaswamy P, Sambandam S, Thankgavel G, Sambandam S, et al. (2011) Air pollution from household solid fuel combustion in India: an overview of exposure and health related information to inform health research priorities. Glob Health Action 4 (1).
-
Brook RD, Franklin B, Cascio W, Hong Y, George H, et al. (2004) Air Pollution and Cardiovascular Disease. Circulation 109(21): 2655-2671.
-
Thomas RJ (2013) Particle size and pathogenicity in the respiratory tract. Virulence 4(8): 847-858.
-
Otuu FC, Shu EN (2019) Prevalent diseases among inmates in three Federal Prisons in South-east geopolitical zone of Nigeria: A peep into the environmental factors. J Environ Sci Public Health 3(1): 010-024.
-
Otuu FC, Shu EN, Maduka IC, Okechukwu CC (2018) Vehicular activities and tailpipe carbon (II) oxide emission at Osisioma, Aba, Abia State, Nigeria: A potential public health hazard to roadside traders and artisans. J Medical Toxicol Res 1(2): 1-6.
-
World Health Organization (2009) World Health Organization Guidelines for Indoor Air Quality: Dampness and Mould, WHO Regional Office in Europe.
-
Lee K, Choi JH, Lee S, Park HJ, Oh YJ, et al. (2018) Indoor levels of volatile organic compounds and Otuu FC, et al. Indoor Air Quality, Cell Features and Lifestyle Characteristics: Implications on the Prevalence of Some Respiratory Tract Diseases and Symptoms among Inmates of Enugu Prison, Nigeria. Adv Clin Toxicol 2019, 4(3): 000163. formaldehyde from emission sources at elderly care centers in Korea. PLoS ONE 13(6).
-
Bruce N, Perez-Padilla R, Albalak R (2000) Indoor air pollution in developing countries: a major environmental and public health challenge. Bull. World Health Organ 78(9): 1078-1092.
-
_Jaakkola MS (2000) Environmental tobacco smoke and_ _respiratory diseases._ Eur Respir Monograph 5_(15):_ 322_-383._
-
Hyland A, Travers MJ, Dresler C, Riward C, Michael CK (2008) A 32-country comparison of tobacco smoke derived particle levels in indoor public places. Tobacco Control 17(3): 159-165.
-
Sureda X, Fernandez E, Lopez MJ, Nebot M (2013) Second hand tobacco smoke exposure in open and semi-open settings: a systematic review. Environ Health Perspect 121(7): 766-773. _13._ Royal College of Physicians (2005) Going smoke-free: the medical case for clean air in the home, at work and in public places. A report on passive smoking by the Tobacco Advisory Group of the Royal College of Physicians, July 2005. _Royal College of Physicians of_ _London._
-
Spengler J (1992) Outdoor and indoor air pollution. In: Principles and practice of environmental medicine. Plenum Medical Book Co, New York, pp: 21- 41.
-
Schwartz J, Zeger S (1990) Passive smoking, air pollution, and acute respiratory symptoms in a diary study of student nurses. Am Rev Respir Dis 141(1): 62-67.
-
Ng TP, Hui KP, Tan WC (1993) Respiratory symptoms and lung function effects of domestic exposure to tobacco smoke and cooking by gas in non-smoking women in Singapore. J Epidemiol Community Health 47(6): 454-458.
-
Leuenberger P, Schwartz J, Ackermann-Liebrich UA, Blaser K, Bolognini G, et al. (1994) Passive smoking exposure in adults and chronic respiratory symptoms (SAPALDIA Study). Am J Respir Crit Care Med 150(5 Pt 1): 1222–1228.
-
Eisner MD, Smith AK, Blanc PD (1998) Bartenders' respiratory health after establishment of smoke-free bars and taverns. JAMA 280(22): 1909-1914.
-
Bentayeb M, Norback D, Bednarek M, Bernard A, Cai G, et al. (2015) Indoor air quality, ventilation and respiratory health in elderly residents living in nursing homes in Europe. Eur Respir J 45(5): 1228- 1238.
-
Tunsaringkarn T, Prueksasit T, Morknoy D, Sawatsing R, Chinveschakitvanich V, et al. (2015) Indoor air assessment, health risks, and their relationship among elderly residents in urban warrens of Bangkok, Thailand. Air Quality Atmosphere Health 8(6): 603-615. Otuu FC, et al. Indoor Air Quality, Cell Features and Lifestyle Characteristics: Implications on the Prevalence of Some Respiratory Tract Diseases and Symptoms among Inmates of Enugu Prison, Nigeria. Adv Clin Toxicol 2019, 4(3): 000163.
- Evaluation of Skin Aging Preventive Effects of Cherry Blossom Petal Extracts Through Antioxidant and Anti-Glycation Activities
- Is Cell Death Responsible for False Positive Results of In Vivo Comet Assay?
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism