Cardiovascular Complications during COVID-19 Infection
In December 2019 a serious outbreak of pneumonia emerged in china. The infection Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), spreads the infection rapidly from China to other countries, and the World Health Organization (WHO) announced Coronavirus disease 2019 (COVID-19) a pandemic. Coronaviruses (CoV) contain a single-stranded RNA genome. The Coronavirus infected through respiratory droplets will be a high-level of transmission and to develop acute respiratory failure but a large portion of patients exploit cardiovascular manifestations. The WHO has stated by august 2020 that 26,171,112 confirmed COVID-19 positive cases and 865,154 deaths were determined all over the world. COVID-19 the consequential hazards to the public health care system of COVID-19 infection for people underlying medical problems have a significantly increased risk of death, especially the ones carrying hypertension, diabetes, cardiovascular diseases, and cerebrovascular disease. Possible vaccines and drugs to treat COVID-19 infection are undergoing. This review discussed cardiovascular complications in severe acute respiratory syndrome produced by coronavirus-2 (SARS-CoV-2).
Introduction
The novel coronaviruses originated in Wuhan, China, acknowledged in December 2019 has been rapidly spread all over the world. On March 11, 2020, it was announced a pandemic by the World Health Organization (WHO) [1]. Coronavirus Disease 2019 (COVID-19) has been officially called severe acute respiratory syndrome corona virus-2 (SARS-CoV2) by the WHO. SARS-CoV2 genome is composed of a single-stranded RNA. It can be highly pathogenic when it is developed in the eruption of causes respiratory infections in humans, although, in general, it has low virulence with excessive infectivity that can rapidly be transmitted also in asymptomatic conditions [2]. The quick transmission of virus infection allowed to be spread out in 185 countries as a pandemic disease [3]. Many governments have considered a different type of lockdown to impede the spread of novel SARS-CoV2. The WHO has initiated fair guidelines on the small amount of physical activity required to maintain enough health and fitness, for example, according to recent statistics the adults aged 18 to 64years are more affected with COVID-19 [4]. The impact of COVID-19 is considered as an increase in morbidity and mortality and high risk for older people (>60years). WHO stated that COVID-19 has an estimated 15,745,102 confirmed cases and 639,317 deaths have been reported (WHO report on July 2020).
The prevalence of human coronavirus diseases such as SARS-CoV and Middle East respiratory syndrome-associated coronavirus (MERS-CoV) has created challenging problems in the public healthcare all over the world [5]. The main symptoms are related to respiratory function failure, ranging from mild flu-like illness such as acute respiratory distress syndrome (ARDS) or fulminant pneumonia. Pre-existing
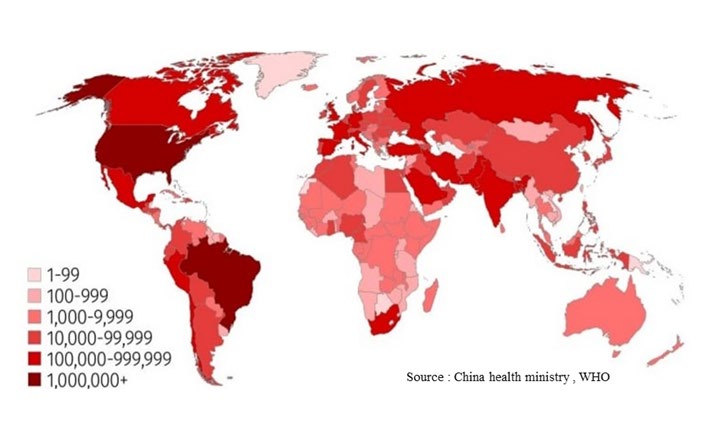
cardiovascular disease and/or cardiovascular risk factors increase the severity of COVID-19 infection [2]. There are no specific characteristics for COVID-19 infection, although respiratory and cardiovascular symptoms are related to the severity of the disease [6]. In the base of SARS‐CoV‐2 infection, it has been found several proinflammatory mediators which play an essential role in the pathophysiology of cardiovascular symptoms, representing around 19% of hospitalized COVID-19 patients. The present review is concentrated on cardiovascular affection by COVID-19 infection [7] (Figure 1).
SARS-CoV-2 Symptoms
SARS-CoV-2 spreads by respiratory droplets through splash and it has been also found in stool. This transmission process takes place in symptomatic or asymptomatic patients with secondary infection at a range of 0.5 -5%. SARS-CoV-2 can remain stable for 3 hours in moisture, for 24hours on cupboards and 3 days on plastics and steels.
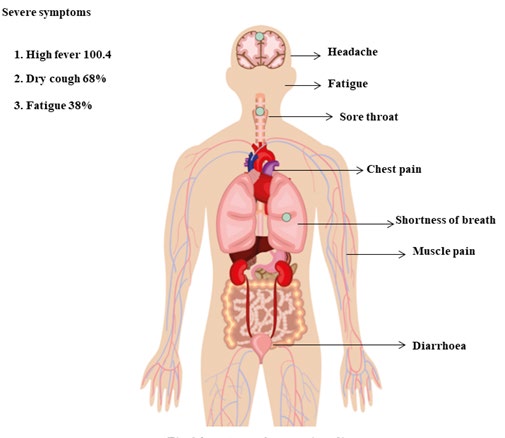
Their lifespan is about 4 -5 days and within 5 days 95.5% of patients will episode symptoms. The most frequent symptoms are fever 100.4, dry cough 68%, and fatigue 38%, accompanied by a viral syndrome; while gastrointestinal symptoms are uncommon in COVID -19 infection. On the other hand, in China over 81% of patients had mild symptoms of COVID-19 while 14% had acute symptoms like dyspnea, low respiratory, septic shock, and multiple organ failure [3] (Figure 2).
Angiotensin-Converting Enzyme 2 in COVID-19 Infection
ACE2 is a carboxypeptidase that mutates angiotensin II into angiotensin (1-7) enzyme homologous to ACE, producing a neutralizing role in angiotensin aldosterone system [8]. A viral infection is related to metabolic demands by doubled when compared to the normal physiology of the heart. The direct outcome of pneumonia can damage cardiac function which is another mechanism for an increased level of angiotensin-converting enzyme 2 [9]. A new study has verified that SARS-Cov-2 uses SARS CoV ACE2 for the entry in a host cell which acts as a pathway leading to infection. The increased ACE2 in SARS-CoV may lead to acute risk [10].
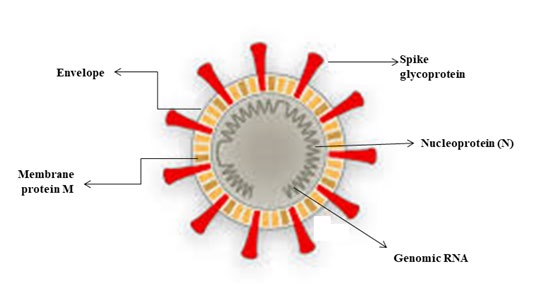
Angiotensin-converting enzyme 2 is a membrane confine aminopeptidase that has an important role in cardiovascular and immune systems. It is associated with hypertension and diabetes mellitus. Besides, it is spotted as an effective structure for coronaviruses like SARS-COV and SARS-CoV-2. The SARS-Cov-2 infection is activated by the bond of spike protein to ACE2 which leads to increase angiotensin II, pulmonary vascular permeability and reduce lung function. It results in respiratory problems by entering alveolar epithelial cells, so patients with cardiovascular disease and increased ACE secretion have more severe symptoms than healthy persons. The ACE2 levels are raised by renin- angiotensin-aldosterone system blockers. It is a functional structure of SARS-CoV-2 [11] (Figure 3).
COVID-19 and Cardiovascular Disease
As per reports, the patients with cardiovascular disease are at greater risk when infected with SARS-CoV. In a file of
138 patients with COVID-19 hospitalized in Wuhan, 46% had an extra co-existing medical condition, mostly cardiovascular disease. It has been a significantly higher risk in patients underlying medical issues. Hypertension was seen in 31.2 % of patients, diabetes in 10%, and cardiovascular disease in 14%. The COVID-19 patents with heart disease lead to an excessive or massive death rate [4]. In one survey of COVID-19 patients, 25% had heart disease, 58% had hypertension, and 44% had arrhythmia, According to NHC the deaths of patients with SARS-CoV-2 had previous experience of hypertension and 17% of them with heart disease. Along with the reports, patients more than 60 years have effective symptoms and acute pneumonia than the ones below 60 years [11].
The COVID-19 infection has the symptoms of lower tract respiratory infection but a large portion of patients exploit cardiovascular symptoms. Among them, it can be highlighted chest tightness. Acute cardiac injury is the most frequently reported cardiovascular problems in COVID-19 infection. In other records, it has been shown that the elevation of high sensitivity cardiac troponin 1 in 10-20% of COVID-19 patients. In China, approximately 11.8% who died from COVID-19 had major heart damage and cardiac arrest without the previous history of cardiovascular disease during hospitalization. The instigate of acute myocardial injury is not clear but it can be related to acute myocarditis or acute coronary syndrome as pre-treated with the Middle East Respiratory Syndrome- associated coronavirus (MERS–CoV). The cardiovascular complication in COVID-19 has some indication like acute cardiac injury, left ventricular systolic dysfunction, heart failure, arrhythmia, and potential long-term consequences like cardiac homeostasis [4]. The process of acute myocardial injury by SARS-CoV-2 infection is correlated to ACE2. It not only affects the lungs but cardiac vascular system too since the signaling pathways is also involved in heart injury. Some of them suggested the process of myocardial injury is by the variated reaction of type I and II helper cells which damages myocardial cells and results in respiratory dysfunction and hypoxemia [11].
SARS-CoV-2 infected patients with acute coronary syndrome always have a low diagnosis. In this case, the cardiac function is reduced resulting in myocardial ischemia or necrosis. There is a cardiac inadequacy likely to occur, which leads to a quick collapse for this type of patient. In Wuhan, some patients with COVID-19 had previous acute coronary syndrome (ACS) with acute illness and major death rates. For patients with heart disease, SARS-CoV-2 acts as projections to exacerbate and leading to death. Heart damage due to drugs during the treatment of COVID-19 infection can occur. The use of antiviral drugs should be examined. In a report of 138 patients with COVID-19 antiviral drugs were administrated. Still, they can induce inadequacy, arrhythmia, or some cardiovascular disorders. So that while administration antiviral drugs for the treatment of COVID-19, the risk of cardiac harm must be observed [11].
Conclusion
The conclusion is public healthcare challenging problems in the world and spread throughout the world. The impact of COVID-19 is considered as an increase in morbidity and mortality. SARS-CoV-2 has an impact on respiratory illness it is at a higher risk for cardiovascular patients. So it is above 25% of critical cases myocardial injury especially angiotensin-converting enzyme inhibitors and angiotensin receptor blocker should be provided by the clinically verified condition. Treatments and investigation are undergoing for COVID-19 and not clinically proven up to date but the researcher was up to their world towards the abolition of COVID-19.
Conflicts of Interest
There are no conflicts of interest
References
-
Pengfei S, Lu X, Xu C, Sun S, Pan B (2020) Understanding of COVID‐19 based on current evidence. Journal of medical virology 92(6): 548-551.
-
Manish B (2020) Cardiovascular disease and COVID-19. Diabetes & Metabolic Syndrome: Clinical Research & Reviews.
-
Clerkin KJ, Fried JA, Raikhelkar J, Sayer G, Griffin JM, et al. (2020) COVID-19 and cardiovascular disease. Circulation 141(20): 1648-1655.
-
Giuseppe L, Henry BM, Sanchis-Gomar F (2020) Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur J Prev Cardiol 27(9): 906-908.
-
Li B, Yang J, Zhao F, Zhi L, Wang X, et al. (2020) Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin Res Cardiol 109(5): 531-538.
-
Jean-Sebastien H (2020) COVID-19 in patients with cardiovascular diseases. Arch Cardiovasc dis 113(4): 225-226.
-
Nunes KA, Tagliari AP, Forleo GB, Fassini GM, Tondo C (2020) Cardiac and arrhythmic complications in patients with COVID‐19.” Journal of Cardiovascular Electrophysiology 31(5): 1003-1008.
-
Akbarshakh A, Marban E (2020) COVID-19 and the heart. Circulation research 126(10): 1443-1455.
-
Rui A, Guzik TJ (2020) Inside the heart of COVID-19. Cardiovascular Research 116(6): e59-e61.
-
Junyi G, Huang Z, Lin L, Lv J (2020) Coronavirus disease 2019 (covid‐19) and cardiovascular disease: a viewpoint on the potential influence of angiotensin‐converting enzyme inhibitors/angiotensin receptor blockers on onset and severity of severe acute respiratory syndrome coronavirus 2 infection. Journal of the American Heart Association 9(7).
-
Ying-Ying Z, Ma YT, Zhang JY, Xie X (2020) COVID-19 and the cardiovascular system. Nature Reviews Cardiology 17(5): 259-260.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells