Anemia Risk in Relation to Occupational and Environmental Lead Exposure among Inhabitants of Enyigba Lead-Zinc Mining Community in Ebonyi State, Nigeria
Introduction: Environmental and occupational exposure to lead contamination is associated with numerous adverse health effects. This study brought forth the case of anemia risk in relation to occupational and environmental lead exposure among inhabitants of Enyigba lead-zinc mining community, in Ebonyi State, Nigeria. Methodology: Blood samples (4mls) were collected from 150 consented participants, by venopuncture and preserved in plain vacutaner bottles. Blood-lead concentration was determined using FS 240AA atomic absorption spectrophotometer (Agilent Technology, USA) according to the method of American Public Health Association. The iron status (total iron, unsaturated iron binding capacity, ferritin, total iron binding capacity, transferin) and hematological indices (hematocrit, hemoglobin, red blood cell count, mean corpuscular volume, mean corpuscular hemoglobin, and mean corpuscular hemoglobin concentration) were determined according to standard methods. An interviewer-administered structured questionnaire designed to reflect basic demographic features was administered to the subjects. Correlation analyses were used to investigate the relationships between blood lead concentrations and hematological indices, iron status and related confounders. Results: The mean blood lead concentrations (BPbC) of the participants were: occupationally–exposed, 42.30 ±10.90 µg/dl; environmentally-exposed, 28.66 ± 9.12µg/dl; Controls, 4.76 ±2.16 µg/dl. There were significant differences (p < 0.05 for each) between the blood lead concentrations of the exposed participants and the control. The mean blood iron concentrations (BFeC) of the participants were: occupationally exposed 29.54 ± 4.23 µg/dl; Environmentally-exposed, 41.97 ± 7.44µg/dl; Controls,
Elvis N Shu1, Fred C Otuu2*, Bello H Tilako3, Irene L Shuneba4, Ijeoma M Otuu-Fred5 and Anthony F Otuu6
55.00 (23.19±23.19 µg/dl. There were significant differences (p < 0.05 for each) between the blood iron concentrations of the exposed participants and the control. There were significant negative correlations between blood lead concentration (BPbC) and each of the hematological indices: RBC (r = -0.165, p<0.05), Hb (r = -0.506, p<0.001), Hct (r = -0.478, p<0.001), MCV (r = -0.408, p<0.001), MCH (r = -0.397, p<0.001) as well as MCHC (r= -0.385, p<0.001). Conclusion: There was anemia risk in relation to occupational and environmental lead exposure among the inhabitants of the Enyigba lead-zinc mining community. Keywords: Anemia; Iron Status; Environmental Exposure; Occupational Exposure; Hematology Abbreviations: TIBC: Total Iron-Binding Capacity; UIBC: Unsaturated Iron Binding Capacity; Sat: Transferrin Saturation; Hct: Haematocrit; Hgb: Hemoglobin, RBC: Red Blood Cell Count; MCV: Mean Corpuscular Volume; MCH: Mean Corpuscular Hemoglobin; MCHC: Mean Corpuscular Hemoglobin Concentration.
Study Background
The adverse health effects of lead exposure are well documented Tasleem JA, et al. [1]; Jadoon S, et al. [2]. Body lead contamination routes include skin contact, ingestion and inhalation of inorganic lead from occupational and environmental exposure and from dietary origin. Thus, lead exposure may come from dust, fume, and poor personal hygiene including eating and smoking with contaminated hands. Bioaccumulation of lead in the body may be determined by different methods (Lead levels in bone, blood, urine, and exfoliated teeth are the major biomarkers of internal dose) [3], but blood lead concentration (BPbC) measurement is still the most common technique to investigate recent lead accumulation in the body. Exhalation of lead condensate from the breath is an emerging non-invasive biomarker of occupational exposure in recent years. Transportation of the inhaled/ingested lead to the heart, bones, intestines, kidneys, reproductive, and nervous systems, causes tissue- specific adverse effects.
Adverse effects on some hematological variables are among the manifestations of lead poisoning in lead-exposed subjects [4, 5]. Interference with enzymatic steps in heme synthesis pathways resulting from chronic lead poisoning inhibits production of hemoglobin in the body, diminishes red blood cells and increases the risk of anemia [6].
Abakaliki lead-zinc mining areas, comprising of Ameka, Ameri and Enyigba communities, provide the inhabitants with economic sustenance next to agriculture. With the discovery and exploitation of solid minerals in Abakaliki division of the old Eastern Nigeria, in the nineteen forties, artisanal mining activities have become significant occupation among the inhabitants, to the extent that virtually all the households within the mining areas are involved in artisanal mining Nwaugo et al. This has affected the environment of the mining areas negatively [7], as heaps of mining tails are scattered everywhere, and lead-zinc metals are heaped in most households, exposing the inhabitants of mining communities to metal pollution [8].
Mining-related environmental pollution is worsened when the mining operations are carried out in crude manner by unskilled artisanal miners resulting in the improper disposal of mining wastes Nwaugo, et al. This is the case with the Abakaliki lead-zinc mining where the impacts of extensive galena extractions by increasing indiscriminate artisanal activities, result to environmental heavy metal load [9].
Studies so far on the impacts of lead-zinc mining in Abakaliki lead-zinc mining area have focused mainly on water, soil and plant metal loads [10, 11], and their speculative health and environmental impacts [8, 12]. Literatures on the impacts of Abakaliki lead-zinc mining on plant physiology, anatomy and nutrient compositions are also available [7, 13]. However, there is scarcity of literature on the impacts of the lead-zinc mining activities on the health status of inhabitants of the Abakiliki mining environment, except for those of Tilako BH, et al. [14] which associated occupational and environmental exposure of the inhabitants of Enyigba community to blood lead contamination and which reported the relationship of lead exposure to the renal status of the inhabitants of Enyigba lead-zinc mining community.
In a culture characterized by poor economic background, high level of illiteracy, inadequate knowledge of primary hygiene, fragile ecosystem, and dispersed demography, the impacts of indiscriminate mining activities may have disastrous public health implications. This study reports anemia risk in relation to occupational and environmental lead exposure among inhabitants of lead–zinc community, in Ebonyi State, Nigeria. Materials and Methods
Ethical Consideration
Ethical approval was obtained from the Research Ethics Committee of the College of Medicine, University of Nigeria, Enugu Campus and from the Research Ethics Committee of the Ebonyi State Ministry of Health, Abakaliki.
Description of the Study Areas
The study took place at Enyigba, one of the four (Enyigba, Ameka, Amagu and Ameri) highly mineralized rural communities that make up the Abakaliki mining area (Federal Ministry of Mines and Power Ebonyi State Office). The Abakiliki mining area lies between latitudes 60081N and 60241N and longitudes 80001E. The principal minerals of interest are lead and zinc, though there are significant concentrations of other elements such as, iron, copper and quartz in some quarters. The total lead mine area is about 21.8sq.km, consisting of three Local Government Areas -Enyigba in Abakaliki LGA, Ameka in Ikwo LGA, and Ameri in Ezza LGA. Enyigba is about 4KM from Abakiliki metropolis which is the capital of Ebonyi State.
Among the four mining communities of the Abakiliki mining area, Enyigba has the longest history of mining activities. The Enyigba Pb-Zn Mine was intermittently mined for lead from 1925 though mining operations ceased during the Nigerian Civil War (1967-1970) that badly affected the industry, but has recently been activated with artisanal mining activities highly pronounced.
The control area- Ezangbo is a non-mining community about 19 km from the Abakiliki metropolis and 23KM from the Enyigba mining site. An Agricultural community with a population of 4,515 (NPC, 2006), Ezzamgbo is the administrative headquarter of Ohaukwu Local Government Area, Ebonyi State and has a geo-reference of 6°23’56.2”N 7°57’41.6”E.
Sampling Population and Procedure
The study involved 150 participants who have lived in the community from 2 years and above and 65 participants who were not living within the vicinity of the mining community. The control participants were recruited from Ezangbo. Non probability purposive sampling technique using Krejcie and Morgan (1970) table constructed using the formula for determining sample size was adopted for selection of the miners, while random sampling technique was adopted for the selection of environmentally exposed and the control participants. The miners comprised of both sexes between the ages of 6 years and 65 years. Voluntary, first person Informed Consent of the participants was obtained.
Blood samples (4mls) were collected from 215 participants consisting of 150 participants from the mining community and 65 from the control, by venopuncture and preserved in plain vacutainer bottles. Blood-lead concentration was determined using FS 240AA atomic absorption spectrophotometer (Agilent Technology, USA) according to the method of American Public Health Association. Total iron and unsaturated iron binding capacity were determined with visible spectrophotometer (Jenway, 67000, UK). Ferrtin was determined by the enzyme-linked immunoassay according to standard methods, while total iron binding capacity was calculated as the sum of total iron and unsaturated iron binding capacity and transferin was calculated from the ratio of serum iron and total iron binding capacity. Hematological parameters [haematocrit (Hct), hemoglobin (Hgb), red blood cell count (RBC), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC)] were analyzed according to standard methods. An interviewer-administered structured questionnaire designed to reflect basic demographic features (gender, age, marital status, educational level, occupation and length of time of living in the community) was administered to the participants. Correlation analyses were used to investigate the relationships between BPbC and hematological indices, iron status and related confounders.
Results
The results of the study are presented in Tables 1-3 and Figures 1(a-f) & 2(a-d). Table 1 represents the demographic features of the participants. Male participants dominated the occupationally exposed (56.18%) and the controls (53.85%) population but females (62.30%) dominated environmentally-exposed. Majorities (52.81%) of the occupationally exposed participants were singles, while married participants (72.28%) dominated the environmentally-exposed and controls (53.83%). The dominant age range for the occupationally exposed (29.21%) and controls (35.38%) was 21-30 years, but for the environmentally-exposed, it was 41-50 years. The dominant duration of stay in the community was >25 years for the occupationally-exposed (40.46%), environmentally-exposed (54.10%) and controls (35.39%).
| Occupationally Exposed n(%) | Environmentally Exposed n(%) | Control n(%) | |
|---|---|---|---|
| Sex | |||
| Male | 50 (56.18) | 23 (37.70) | 35 (53.85) |
| Female | 39 (43.82) | 38 (62.30) | 30 (46.15) |
| Total | 89 100.00 | 61 100.00 | 65 100.00 |
| Age (Yrs) | |||
| <10 | 05 (05.62) | 10 (16.39) | 05 (07.69) |
| 11 – 20 | 22 (24.72) | 03 (04.92) | 08 (12.31) |
| 21 – 30 | 26 (29.21) | 04 (06.56) | 23 (35.38) |
| 31 – 40 | 23 (25.84) | 12 (19.67) | 18 (27.69) |
| 41 – 50 | 05 (05.62) | 17 (27.87) | 07 (10.77) |
| 51 – 60 | 07 (07.87) | 10 (16.39) | 02 (03.08) |
| >60 | 01 (01.12) | 05 (08.20) | 02 (03.08) |
| Total | 89 100.00 | 61 100.00 | 65 100.00 |
| Marital Status | |||
| Married | 39 (43.82) | 44 (72.13) | 35 (53.82) |
| Single | 47 (52.81) | 12 (19.67) | 28 (43.08) |
| Widow/Widower | 03 (03.37) | 05 (08.20) | 02 (03.10) |
| Total | 89 100.00 | 61 100.00 | 65 100.00 |
| Educational Level | |||
| No Formal Education | 08 (08.99) | 17 (27.87) | 07 (10.77) |
| Primary | 29 (32.58) | 34 (55.74) | 17 (26.15) |
| Secondary | 49 (55.06) | 07 (11.47) | 35 (53.85) |
| Tertiary | 03 (03.37) | 03 (04.92) | 06 (09.23) |
| Total | 89 100.00 | 61 100.00 | 65 100.00 |
| Duration in the Community (Yrs) | |||
| <5 | 09 (10.11) | 12 (19.67) | 07 (10.77) |
| 6 – 10 | 09 (10.11) | 08 (13.11) | 04 (06.15) |
| 11 – 15 | 15 (16.85) | 02 (03.28) | 11 (16.92) |
| 16 – 20 | 17 (19.10) | 02 (03.28) | 14 (21.54) |
| 21 – 25 | 03 (03.37) | 04 (06.56) | 06 (09.23) |
| >25 | 36 (40.46) | 33 (54.10) | 23 (35.39) |
| Total | 89 100.00 | 61 100.00 | 65 100.00 |
Table 1: Demographic Features of the Participants.
The mean blood lead concentrations (BPbC) of the participants were: occupationally-exposed 42.30 ±10.90 µg/ dl; environmentally-exposed, 28.66 ± 9.12µg/dl; and Controls, 4.76 ± 2.16 µg/dl. There were significant differences (p < 0.05 for each) between the blood lead concentrations of the occupationally and environmentally-exposed participants and between each of the groups with the control.
The mean blood iron concentrations (BFeC) of the participants were: occupationally-exposed, 29.54 ±4.23 µg/dl; environmentally-exposed, 41.97 ± 7.44µg/dl; and Controls, 55.00 (23.19 ± 23.19µg/dl. There were significance differences (p < 0.05) between the blood iron concentrations of the occupationally and environmentally exposed participants and between each of the groups with the control. The hematological indices of the participants are presented in Table 2. The mean RBC, Hb, Hct, MVC, MCH, MCHC levels of occupationally-exposed and environmentally- exposed individuals were significantly lower (p<0.001 for each), monocytes mean levels were significantly higher (p<0.001 for each) and lymphocytes were significantly lower (p<0.05 for each) when compared with the mean levels of corresponding controls. The neutrophil levels of the occupationally-exposed were significantly higher (p<0.05) when compared with the controls.
| Parameters | Occup. Exposed n=89 Mean (SD) | Environ. Exposed n=61 Mean (SD) | Control n=65 Mean (SD) |
|---|---|---|---|
| WBC (x109/L) | 5.53 (1.55) | 5.14 (1.67) | 5.31 (1.26) |
| RBC (x1012/L) | 4.62 (0.67)** | 4.52 (0.67)** | 4.94 (0.39) |
| Hb (g/dl) | 11.42 (1.18)** | 11.69 (1.59)** | 13.38 (0.91) |
| Hct (%) | 34.62 (3.70)** | 35.87 (5.03)** | 40.68 (3.33) |
| Plts (x109/L) | 212.30 (73.11) | 204.01 (68.70) | 203.71 (55.05) |
| MCV (fl) | 78.70 (5.09)** | 80.72 (6.34)** | 85.06 (3,86) |
| MCH (pg) | 25.85 (1.82)** | 25.93 (2.41)** | 28.51 (1.33) |
| MCHC (g/dl) | a31.02 (1.91)** | 31.69 (1.24)** | 33.03 (1.01) |
| Neut (%) | 50.23 (12.28)* | 46.74 (12.00) | 47.89(11.23) |
| Lymp (%) | 41.16 (6.63)* | 43.84 (7.29)* | 45.54 (11.19) |
| Mono (%) | 4.91 (2.78)** | 5.01 (5.06)** | 2.74 (1.52) |
| Eos (%) | a2.73 (2.58) | 1.87 (2.22) | 2.16 (1.76) |
| Baso (%) | 0.97 (0.85) | 0.83 (0.79) | 0.88 (0.67) |
Table 2: Hematological Indices of the Participants. Occup/Environ vs controls: *p<0.05, **p<0.001; Occup. vs Environ: ap<0.05 RBC
Table 2: Hematological Indices of the Participants. Occup/Environ vs controls: *p<0.05, **p<0.001; Occup. vs Environ: ap<0.05 RBC= Red blood cells; Hb= Haemoglobin; Hct= Haematocrit; Plt= Platelets; MCV= Mean cell volume; MCH= Mean cell haemoglobin; MCHC= Mean cell haemoglobin concentration; Neut= Neutrophils; Lymp= Lymphocytes; Mono= Monocytes; Eos= Eosinophils; Baso= Basophils.
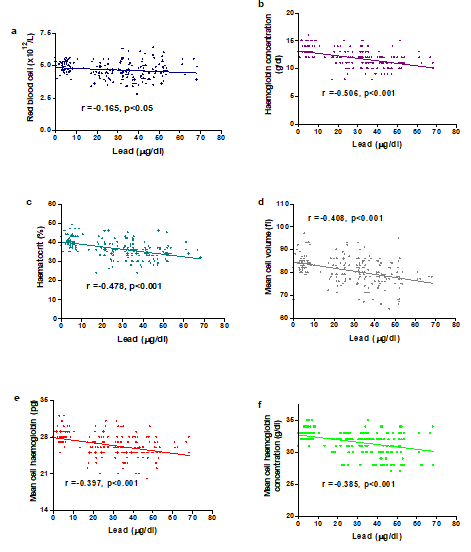
Figures 1(a-f) represents a correlation between blood lead concentration (BPbC) and some hematological indices of the participants. There were significant negative correlations between BPbC and each of the hematological indices: RBC (r = -0.165, p<0.05), Hb (r = -0.506, p<0.001), Hct (r = -0.478, p<0.001), MCV (r = -0.408, p<0.001), MCH (r = -0.397, p<0.001) as well as MCHC (r= -0.385, p<0.001).
Table 3 represents the iron status of the study participants. The mean ferritin, total iron, total iron binding capacity and transferin saturation concentrations of occupationally-exposed individuals were significantly lower (p<0.001 for each) when compared with the mean concentrations of controls, while the unsaturated iron binding capacity was significantly higher (p<0.05) when compared with the controls.
In the environmentally-exposed participants, the mean total iron, total iron binding capacity and transferin saturation concentrations were significantly lower (p<0.001 for each) while the unsaturated iron binding capacity mean concentration was significantly higher (p<0.05) when compared with the controls.
In the occupationally-exposed, the mean ferritin concentration was significantly lower (p<0.001) when compared with the corresponding mean levels of environmentally-exposed individuals.
| Parameters | Occup. Exposed n=89 Mean (SD) | Environ. Exposed n=61 Mean (SD) | Control n=65 Mean (SD) |
|---|---|---|---|
| Ferritin (ng/ml) | a50.12 (24.01)** | 84.23 (48.28) | 90.62 (36.17) |
| Total iron (µg/dl) | 39.23 (18.73)** | 42.10 (30.47)** | 109.08 (36.33) |
| TIBC (µg/dl) | 298.01 (80.67)** | 295.35 (83.02)** | 336.72 (88,87) |
| UIBC (µg/dl) | 259.15 (71.64)* | 258.04 (72.49)* | 228.97 (72.83) |
| Trans. Sat. (%) | 14.39 (6.41)** | 14.88 (11.30)** | 31.83 (8.83) |
Table 3: Iron Status of the Participants. Occup/Environ vs controls: *p<0.05, **p<0.001; Occup. vs Environ: ap<0.001 TIBC = Total
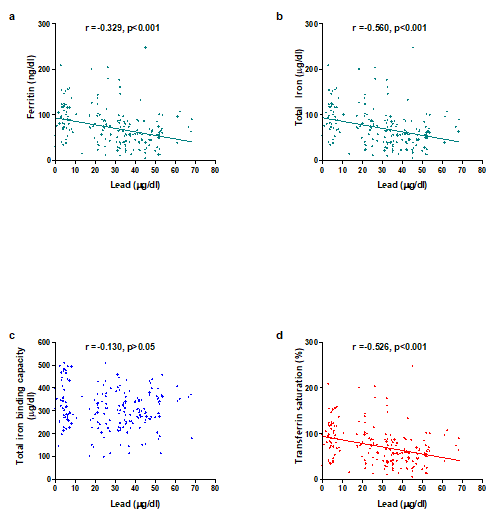
Figure 2 represents a correlation between blood lead concentrations and iron status of the study participants. There were significant negative correlations between blood lead levels and each of ferritin (r= -0.329, p<0.001), total iron (r= -0.560, p<0.001), transferrin saturation (r= -0.526, p<0.001), but no correlation with total iron binding capacity (r= -0.130, p>0.05).
Discussion
This study was designed to focus on anemia risk in relation to occupational and environmental lead exposure among inhabitants of Enyigba lead-zinc mining community. Therefore, hematological indices (red blood cell, RBC; hemoglobin, Hb; heamatocrit, Hct; mean corpuscular volume, MCV; mean corpuscular hemoglobin, MCH, and mean corpuscular hemoglobin concentration, MCHC) and iron status (total iron, ferritin, transferin, TIBC, UIBC) were used to represent BPb-induced iron deficiency anemia. The use of these hematological indices in the diagnostic workup of lead-related occupational anemia has been reportedly applied to evaluate the critical BPbCs to protect lead workers [15].
Demographically, women (51.30%) dominated mining activities in the community, probably because lead-zinc mining and farming activities are common occupations in the lead-zinc mining communities of Abakaliki [16]. In the absence of quality education for enhanced employment opportunities, subsistence agriculture is a common occupation among the Ebonyi ruralites. Though women are actively involved in this subsistence farming practice, the recent recognition of the economic opportunities in artisanal lead-zinc mining is gradually shifting agricultural dominated economy to mixed economy. Consequently, the women ruralists are emerging as artisanal miners. Recycling of lead by sieving stream sediments and mining tails seem less tedious than farming and holds strong attraction to women, especially when relatively quicker money can be realized with lesser efforts. According to Ausalu Tadesse D, et al. [17], the socio-cultural environment and the nature of business are among the factors influencing a female’s participation in any business. The global gender report [18] also supported the fact that women tend to shy away from businesses with potential threats to physical and environmental health, and in the ignorance of the adverse health effects of lead-zinc mining activities, the female ruralites would show more preference to lead recycling. The absence of divorcées among the respondents presupposed strong marriage bond. This could also favor more women participation in the mining activities as some of the men are polygamous, a culture commonly found in Abakaliki rural communities [19]. Polygamy is culturally accepted among rural agricultural communities since it means more helping hands to the husbands in their farms.
Tilako BA, et al. [19] reported that lack of knowledge of the harmful effects of lead contamination and the need to use appropriate protective gadgets contributed to the environmental lead exposure and high blood lead levels among the inhabitants of Enyigba mining community. In a culture characterized by poor economic background, high level of illiteracy, inadequate knowledge of primary hygiene, fragile ecosystem, and dispersed demography, occupational and environmental exposure to lead contamination and its adverse health implications are strongly possible.
That the mean BPbC of the exposed participants was higher than that of the control meant that mining activities exposed the inhabitants to lead contamination. This agreed with a similar study by Tilako BA, et al. [19] which associated occupational and environmental exposure of the inhabitants of Enyigba community to lead contamination. Ukaejiofo EO, et al. [4] also implicated occupational exposure in blood lead contamination among lead handlers in Enugu urban, Enugu State, Nigeria and Fazli D, et al. [20] reported that work practices in the automobile repair shop seemed to increase the body burden of lead and could pose a health risk to the workers.
The exposed participants generally had lower blood iron concentration (BFeC) than the control participants. This was in line with the study of Hegazy AA, et al. [21] which reported that high blood lead levels were associated with low serum iron and ferritin in a population of 60 children from the pediatric clinic in Al-Zhraa University hospital and a special pediatric clinic in a rural area, and that of Słota M, et al. [22] which reported a correlation between blood lead level and a reduced body iron store and increasing the risk of anemia in a systemic review of 58 studies.
A study Hegazy AA, et al. [21] reported that at the blood lead level range of 10-20 μg/dl, a significant association was found for mild and severe anemia; the blood level of iron and ferritin was found to be significantly lower in high blood lead level and anemic groups than those of the low blood lead level and control groups, implicating blood lead in iron deficiency anemia. The negative and significant correlation (p <0.05) of BPbC with the hematological indices in the present study supported the above statement and implicated lead exposure in the prevalence of iron efficiency anemia among the inhabitants of Enyigba lead-zinc mining community. Similarly other studies Keramati MR, et al. [23]; Hsieh NH, et al. [24] also correlated iron deficiency anemia with occupational and environmental lead exposure.
According to WHO criteria [25] a person is considered anemic when the Hb concentration is < 13g/dl in male or < 13g/dl. The values obtained in both occupationally and environmentally exposed participants were < 13g/dl, unlike that of the control, and the existence of significant difference (p < 0.05) between the exposed participants and the control suggested that exposure to lead was responsible for the anemic condition among the lead exposed participants. Other hematological indices (RBC, Hb, Hct, MCV, MCH, and MCHC) and iron status (total iron, ferritin, transferin, TIBC, UIBC) are often used to situate the anemia as iron deficiency anemia [5, 26]. According to Faruqi A, et al. [26], in iron-deficient conditions, the relative transferrin content compared to serum iron content increases, and thus the TIBC values are high. The opposite happens in iron overloaded states of the body; the quantity of free transferrin in blood decreases, and consequently, TIBC values are low.
That the values of most of the hematological indices of the exposed participants in the present study were significantly different with those of the control corroborated the study of Chewable A, et al. [5] which reported that the values of Hct, MCV, and MCH were significantly lower in the lead-exposed group than in the controls by 3%, 5%, and 3%, respectively in a study of 80 male subjects employed in the zinc-lead works in Miasteczko Śląskie. However, the present study which presented higher value of MCHC in the control than in the exposed participants contradicted the study Chewable A, et al. [5] which reported a higher value of MCHC in the exposed group than in the controls by 3%. Other studies Soleman SR, et al. [27]; Chukwukasi KW, et al. [28] has reported similarly on the negative effects of lead exposure on hematological indices and incidence of anemia.
Serum iron indicates the amount of iron bound to transferrin in the plasma, but only a small proportion of the body’s iron is bound to transferrin at any given time [29]. Owing to the fact that there is a rapid turnover of transferrin- bound iron and circulating iron concentration can be affected by dietary intake, there is significant variation in iron concentration within each day and between days [15]. Consequently, an assessment of serum iron alone may not provide sufficient information on iron deficiency anemia.
Thus, total iron-binding capacity (TIBC) assay which determines the amount of iron that can be bound to unsaturated transferring is usually a substantive measure of transferring [26]. Though TIBC concentrations do not change rapidly in the plasma, it is not a useful marker of early iron deficiency as values do not change until stores are depleted (WHO) [25]. However, both TIBC and transferrin rise in iron deplete states and fall in inflammatory and iron overload disorders [26]. In the present study TIBC and transferin were significantly (P <0.05) lower in the exposed participants than in the control, pointing to the possibility of inflammatory and iron overload disorders. In the word of Faruqi A, et al. [26], TIBC also decreases in liver diseases, like cirrhosis, as transferrin is synthesized by the liver. Thus, TIBC levels may be low in multifactorial anemias or anemias of chronic inflammation which could be the case with the present study, though the study did not investigate inflammatory disease markers.
The major iron storage protein in the body is ferritin which is mainly intracellular though a soluble form is found in the blood which can be assayed in iron status study Cohen LA, et al. [30]. Although a ferritin concentration of less than 15μg/L in adults (WHO) [25] is diagnostic of iron deficiency and its elevation may reflect iron overload, ferritin is nevertheless, an acute phase protein which may also be increased in liver disease, malignancy, infection and inflammatory diseases [31]. Thus, a normal ferritin concentration alone does not necessarily exclude iron deficiency.
Conclusion
There was anemia risk in relation to occupational and environmental lead exposure among the inhabitants of the Enyigba lead-zinc mining community. It is recommended that adequate sensitization of the inhabitants on the health implications of unregulated and unprotected mining activities be embarked upon by appropriate government agencies to forestall the progression of lead-related diseases. Investigation of BPbC should be integrated among necessary diagnostic requirements for the management of anemia in Enyigba community of Ebonyi State.
Acknowledgment
This study was funded by Tertiary Education Trust Fund (TETFUND/DR&D/CE/UNI/NSUKKA/RP/VOL.I). Authors also wish to acknowledge the assistance of the community leaders who made it possible for peaceful community entry to be achieved.
Conflict of Interest: None
References
-
Tasleem JA, Mudsser A, Kehkasha S, Arif A, Inho C (2015) Heavy metals and human health, mechanistic insight into toxicity and counter defence system of antioxidant. Int J Mol Sci 16(12): 29592-29630.
-
Jadoon S, Malik A (2017) DNA Damage by Heavy Metals in Animals and Human Beings: An Overview. Biochem Pharmacol 6: 235.
-
Barbosa F, Tanus-Santos JE, Gerlach RF, Parsons PJ (2005) A Critical Review of Biomarkers used for Monitoring Human Exposure to Lead: Advantages, Limitations and Future Needs. Environ Health Perspect 113(12): 1669- 1678.
-
Ukaejiofo EO, Thomas N, Ike SO (2009) Haematological assessment of occupational exposure to lead handlers in Enugu urban, Enugu State, Nigeria. Niger J Clin Pract 12(1): 58-64.
-
Chewable A, Maksym B, Dobrakowski M, Kasperczyk S, Pawlas N, et al. (2018) The effect of occupational chronic lead exposure on the complete blood count and the levels of selected hematopoietic cytokines. Toxicol Appl Pharmacol 355: 174-179.
-
ATSDR (2007) Toxicological Profile for lead”, Final Report of the Agency for Toxic Substances and Diseases Registry, Public Health Service, US Department of Health and Human Services.
-
Otuu FC, Shu EN, Aloh O (2018) Environmental Pollution and Food Quality: Impact of Lead-Zinc Mining on Four Staple Foods. Lambert Academic Publishing.
-
Elvis SN, Fred OC, Ignatius M, Bello TH, Alfreda NO, et al. (2019) Public Health Implications of Continous Ethnomedical Use of Some Plant Species Encountered in Enyigba Lead-Zinc Mining Community of Ebonyi State, Nigeria. IOSR Journal of Environmental Science, Toxicology and Food Technology 13(6): 62-68.
-
Eze VC, Okoye JI, Agwung FD Nnabueke C (2008) Chemical and microbiological evaluation of soybeans flours bought from local markets in Onitsha, Anambra State, Nigeria. Continen J Appl Sci 3: 39-45.
-
Edeogu CO, Ekuma CE, Okaka ANC, Ezeonu FC, Uneke CJ, et al. (2007) Public health significance of metals concentration in soils, water and staple foods in Abakaliki South Eastern Nigeria. Trends Appl Sci Res 2: 439-444.
-
Ezeh HN, Chukwu E (2011) Small scale mining and heavy metals pollution of Agricultural soils: The case of Ishiagu Mining District, South Eastern Nigeria. Journal of Geology and Mining Research 3(4): 87-104.
-
Utumoh EJ, Uraku AJ, Omaka ON, Nwabue FI (2012) Global Journal of Bio-science and Bio-technology. Root Indexing 1(2): 320-323.
-
Okogbue CO, Ukpai SN (2013) Evaluation of trace element contents in groundwater in Abakaliki metropolis and around the abandoned mine sites in the southern part, Southeastern Nigeria. Environ Earth Sci 70(7): 3351- 3362.
-
Tilako BH, Ogbodo SO, Okonkwo IN, Shuneba IL, Enyinna O, et al. (2020) Nephrotoxicity Effect in Inhabitants of a Lead-Zinc Mining Community, Ebonyi State, Nigeria. Journal of Biological Sciences 20(2): 80-87.
-
Dale JC, Burritt MF, Zinsmeister AR (2002) Diurnal variation of serum iron, iron-binding capacity, transferrin saturation, and ferritin levels. Am J Clin Pathol 117(5): 802-809.
-
Aloh OG, Aloh HE, Obasi NA, Chukwu K (2017) Evidence of heavy metal contamination of agricultural soil in Ameri, Abakaliki lead- zinc mining area, Ebonyi state Southeast Nigeria: An indication for phytoremediation. Nutr Food Tech 3(3): 1-5.
-
Ausalu Tadesse D (2020) Factors affecting women entrepreneurs in establishing their own business: The case of afans region, Ethiopia. Afr J Bus Mgt 14(3): 86-92.
-
(2018) The Global Gender Report. World Economic Forum, pp: 10-11.
-
Tilako BA, Chibuisi FO, Bassey EE, Shu EN (2019) Blood- lead levels among Inhabitants of Enyigba lead-Zinc Mining Community of Ebonyi State, Nigeria: Indications of Occupational and Environmental Health Hazards. Adv Clin Toxicol 4(3): 000162.
-
Fazli D, Malekirad A, Mirzaee M, Dastjerdi H, Mostafalou S, et al. (2014) Study on the Link between Lead Exposure and Hematological, Psychological, and Memorial Parameters in Automobile Repair Workers. Health 6(8): 712-719.
-
Hegazy AA, Zaher MM, Abd El-Hafez MA, Morsy AA, Saleh RA (2010) Relation between anemia and blood levels of lead, copper, zinc and iron among children. BMC Res Notes 3: 133.
-
Słota M, Wąsik M, Stołtny T, Machoń-Grecka A, Kasperczyk S (2022) Effects of environmental and occupational lead toxicity and its association with iron metabolism. Toxicology and Applied Pharmacology 434: 115794.
-
Keramati MR, Manavifar L, Badiee Z, Sadeghian MH, Farhangi H, et al. (2013) Correlation between blood lead concentration and iron deficiency in Iranian children. Nigerian medical journal. Journal of the Nigeria Medical Association 54(5): 325-328.
-
Hsieh NH, Chung, SH, Chen SC, Chen WY, Cheng YH, et al. (2017) Anemia risk in relation to lead exposure in lead-related manufacturing. BM C Public Health 17(1): 389.
-
(2011) Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System. Geneva: World Health Organization.
-
Faruqi A, Mukkamalla SKR (2022) Iron Binding Capacity. _In:_ Stat Pearls [Internet]. Treasure Island (FL): Stat Pearls.
-
Soleman SR, Andini SA, Rosita L (2020) Lead Exposure Effect on Peripheral Blood Parameters among People around Bus Terminal in Yogyakarta. Asia Pacific Journal of Medical Toxicology 9(1): 11-16.
-
Chukwukasi KW, Chikee AE, Ndudi OE, Nwabueze AE (2021) Association between Lead Exposure and Haematological Parameters among Roadside and Organized Panel Beaters in Enugu Metropolis. Nigeria. JOHE 10(1): 48-56.
-
Takami T, Sakaida I (2011) Iron regulation by hepatocytes and free radicals. J Clin Biochem Nutr 48(2): 103-106.
-
Cohen LA, Gutierrez L, Weiss A (2010) Serum ferritin is derived primarily from macrophages through a nonclassical secretory pathway. Blood 116(9): 1574- 1584.
-
Gabay C, Kushner I (1999) Acute-phase proteins and other systemic responses to inflammation. N Engl J Med 340(6): 448-454.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells