Ecigarette or Vaping Product Use Associated Lung Injury (EVALI) Reports to NPDS Implicated New Marijuana Substances
Context: Beginning Aug-2019, the Centers for Disease Control and Prevention (CDC) initiated investigation of e-cigarette or Vaping Product Use-Associated Lung Injury (EVALI). We examined all National Poison Data System (NPDS) EVALI cases through 31-Mar-2020 for substances, treatments, clinical effects, and medical outcome. We also examined all NPDS eCig exposures for earlier reports of EVALI. Methods: We extracted all exposures coded to EVALI product code 7322608 (E-Cigarette Associated Pulmonary Illness) and all single substance exposures to any of 6 NPDS eCig generic codes (GCs). We examined substance, patient characteristics, and exposure details on the severity of EVALI via multivariate analyses. We developed an EVALI clinical score (ECS) based on the EVALI clinical effects (CEs) and treatments weighted by the % of cases for each finding. We used ECS to search for EVALI candidate cases from 2001 to 31-Mar-2020. Descriptive statistics and change over time via linear and quadratic regression, and multivariate analyses were via (SAS JMP, 12.0.1). Discussion: Through 31-Mar-2020, PCs reported 822 EVALI cases. The EVALI profile over time 15-Aug - 12-Sep-2019 for 196 cases was described by an exponential increase with a doubling time [95% CI] of 8.31 [8.24, 8.37] days. Age: median [min, max] was 22 [1, 77] years, Male: 64.9%, Chronic 50.3%. Medical Outcomes included Death 1.95%, Major 17.9%, and Moderate 57.1%. Multivariate analysis of the first 107 EVALI cases as of 14-Sep-2019 implicated Marijuana Products (p=0.0007). Similar analyses of all 822 cases confirmed Marijuana (p<0.00001), Chronicity (p=0.00031), and Age (p=0.0152) contributing to CE score. Of the 23,252 eCig exposures (23,463 - 211 EVALI cases), 133 (0.567%) had an ECS > median and 370 (1.57%) scored > 25%tile of EVALI cases (EVALI-25+). The time course of these 370 eCig cases showed a distinct increase (inflection) ~16- Aug-2019. Conclusions: The first 107 NPDS EVALI case scores were related to marijuana product exposure. This was confirmed via similar analyses for all 822 cases. The numbers of EVALI-25+ cases show a distinct increase in Aug-2019, suggesting EVALI was a newly emerging phenomenon. Our analysis should encourage public health agencies to utilize NPDS, especially in data collection.
Introduction
The modern electronic cigarette (e-Cig) was invented in 2003 [1]. E-Cigs are electronic delivery systems with a battery powered heating element to aerosolize a variety of materials for inhalation. Fluids may contain nicotine, tetrahydrocannabinol, cannabidiol, synthetic cannabinoids, marijuana and marijuana plant extract, flavorings, solvents, and other chemicals. The solvent is usually propylene glycol and/or glycerin [1]. Marketed as a cigarette alternative, e-Cigs have gained in popularity since introduction in 2007 and sales have increased annually [2]. The American Association of Poison Control Centers (AAPCC) introduced eCig product codes in 2010 into the Poisindex® (IBM Watson Health, Greenwood Village, CO) products database. The 55 US poison centers use the hierarchical Poisindex system to identify exposure substances in the National Poisons Data System (NPDS). Initial concern was pediatric exposures (infants and children) to the concentrated e-Cig nicotine fluid and CDC reported an increase in pediatric exposure calls to poison centers [3]. In June 2019, health care providers began reporting unexplained pulmonary illnesses associated with e-Cig use. US poison centers also began recording cases involving teen and young adults of unexplained pulmonary illness associated with e-Cig use and a specific code was established to identify e-Cig or vaping product use-associated lung injury (EVALI). The AAPCC Rapid Coding team created an EVALI code on 22-Aug-2019, and the first case was dated 10-Jun-2019.
Beginning in August 2019, the Centers for Disease Control and Prevention (CDC) initiated multistate investigation of e-Cig or vaping product use-associated lung injury (EVALI). By 12 September 2019, CDC had reported 380 confirmed or probable cases.
AAPCC’s NPDS collects data in near real-time from the 55 US poison centers. We examined all NPDS EVALI cases through 31-Mar-2020 for substances, treatments, clinical effects, and medical outcome. We also examined all NPDS e-Cig exposures for earlier reports of EVALI.
Methods
We examined all closed, human exposures coded to IBM/Micromedex EVALI emergent product code 7322608 (eCAPI) cases uploaded by the 55 US poison centers to the NPDS 1-Jun-2019 through 30-Mar-2020 for patient demographics, reported substance, clinical effects (signs, symptoms, diagnostic findings), treatments, and outcomes. We examined substances (nicotine, marijuana, or other); flavoring used (yes, no, unknown); duration of exposure; and chronicity. Outcomes included level of care and medical outcome.
We also examined all closed, human, single substance exposures to any of 6 NPDS e-Cig generic codes (GCs) for 1 January 2001 through 31 Mar 2020.
The NPDS case system has a pick list of 169 clinical effects (CEs) from which the poison center specialist can select 1 or more to record the symptoms, signs, and laboratory findings reported for each case.
We developed an EVALI clinical score (ECS) based on the EVALI clinical effects (CEs) and treatments weighted by the prevalence of that CE or treatment cases in the EVALI cases reported. We used ECS to search for EVALI candidate cases from 2006 to 31 March 2020. We examined substance association, patient characteristics, and exposure details on the severity of EVALI via multivariate analyses.
Descriptive statistics for case characteristics change over time via linear and quadratic regression, and multivariate analyses were via SAS JMP, 12.0.1 (SAS Institute, Cary, NC).
Results
Reported EVALI Cases
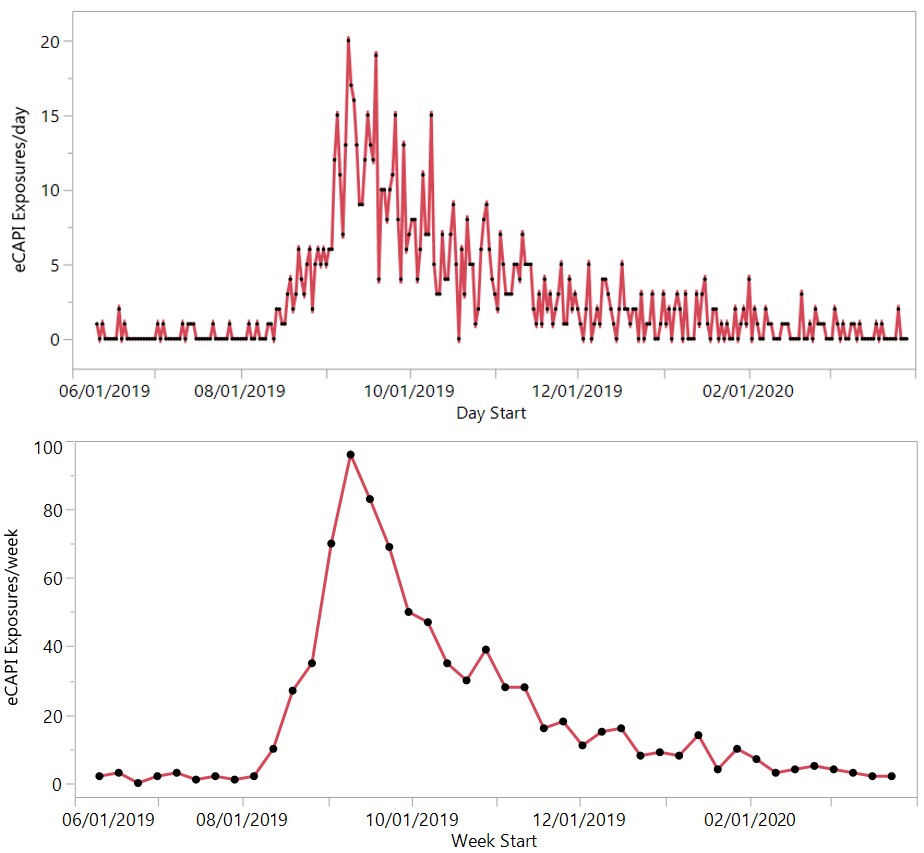
Through 31-Mar-2020, PCs reported 822 EVALI cases. The EVALI profile over time (Figure 1) 15-Aug through 12-Sep-2019 for 196 cases was described by exponential increase: doubling time [95% CI] of 8.31 [8.24, 8.37] days. Table 1 shows the description of patients for the 822 EVALI cases with a breakdown by whether the patient reported exposure to a marijuana-containing product.
| Marijuana Exposure (n=351) | No Marijuana (n=471) | Total (n=822) | |
|---|---|---|---|
| Age (years)a | 26.5 ± 11.9 | 27.6 ± 13.6 | 27.1 ± 12.9 |
| Age (years)a | 22 [13, 76] | 23 [1, 77] | 22 [1, 77] |
| Genderb | F 113 (32.2%) | F 175 (37.2%) | F 288 (35%) |
| Genderb | M 238 (67.8%) | M 296 (62.8%) | M 534 (65%) |
| Number of Productsb | 1: 1 (0.3%) | 1: 210 (44.6%) | 1: 211 (25.7%) |
| Number of Productsb | 2: 254 (72.4%) | 2: 238 (50.5%) | 2: 492 (59.9%) |
| Number of Productsb | 3: 82 (23.4%) | 3: 22 (4.7%) | 3: 104 (12.7%) |
| Number of Productsb | 4: 14 (4%) | 4: 0 (0%) | 4: 14 (1.7%) |
| Number of Productsb | 5: 0 (0%) | 5: 1 (0.2%) | 5: 1 (0.1%) |
| Nicotine Productb | No 92 (26.2%) | No 32 (6.8%) | No 124 (15.1%) |
| Nicotine Productb | Yes 259 (73.8%) | Yes 439 (93.2%) | Yes 698 (84.9%) |
| Other Productb | No 225 (64.1%) | No 324 (68.8%) | No 549 (66.8%) |
| Other Productb | Yes 126 (35.9%) | Yes 147 (31.2%) | Yes 273 (33.2%) |
| Medical Outcomebd | Death 3 (0.9%) | Death 6 (1.3%) | Death 9 (1.1%) |
| Medical Outcomebd | Major 70 (19.9%) | Major 77 (16.3%) | Major 147 (17.9%) |
| Medical Outcomebd | Mod 198 (56.4%) | Mod 204 (43.3%) | Mod 402 (48.9%) |
| Medical Outcomebd | Less S 80 (22.8%) | Less S 184 (39.1%) | Less S 264 (32.1%) |
| Clinical Effect Score – CES (%)a | 129% ± 72.2% | 102% ± 64.2% | 114% ± 68.9% |
| Clinical Effect Score – CES (%)a | 124% [0, 325%] | 98% [0, 336%] | 109% [0, 336%] |
| Therapy Score (%)a | 77.2% ± 59.5% | 61.2% ± 55.9% | 68% ± 58% |
| Therapy Score (%)a | 85.3% [0, 197%] | 56.4% [0, 197%] | 64.9% [0, 197%] |
| EVALI Clinical Score – ECS (%)a | 206% ± 118% | 164% ± 105% | 182% ± 113% |
| EVALI Clinical Score – ECS (%)a | 214% [0, 487%] | 156% [0, 497%] | 179% [0, 497%] |
Table 1: Description of EVALI Patients by Marijuana Exposure.
a reported as mean ± standard deviation, median [min, max]; b reported as number (%); c Mod = Moderate outcome, Less S = Less severe (all other outcomes) Table 1: Description of EVALI Patients by Marijuana Exposure.
| Count | % of 822 cases | Clinical effect | Count | % of 822 cases | Treatment |
|---|---|---|---|---|---|
| 446 | 54.3 | Dyspnea | 385 | 46.8 | Antibiotics |
| 393 | 47.8 | X-ray findings(+) | 363 | 44.2 | steroids |
| 362 | 44 | Coungh/Choke | 338 | 41.1 | Oxygen |
| 253 | 30.8 | Fever/Hyperthermia | 151 | 18.4 | Fluids, IV |
| 247 | 30 | other-Respiratory | 146 | 17.8 | Bronchodilators |
| 181 | 22 | Vomiting | 137 | 16.7 | Others |
| 175 | 21.3 | Nousea | 100 | 12.2 | Intubation |
| 159 | 19.3 | chest pain ( incl. noncradiac) | 97 | 11.8 | Ventilator |
| 130 | 15.8 | Pneumonitis | 55 | 6.7 | Sedation (other) |
| 120 | 14.6 | Tachycardia | 41 | 5 | Benzodiazepines |
| 104 | 12.7 | Diarrhea | 40 | 4.9 | Ventilation, Non-invasive (CPAP, BiPAP) |
| 101 | 12.3 | Hyperventilation/techypnea | |||
| 99 | 12 | Respiratory depression | |||
| 90 | 10.9 | Abdominal pain |
Table 2: Counts of the 15 most frequently reported Clinical Effects and 11 most frequent Therapies for the 822 EVALI cases EVALI
Table 2: Counts of the 15 most frequently reported Clinical Effects and 11 most frequent Therapies for the 822 EVALI cases EVALI Clinical Score (ECS) = Clinical Effect Score (CES) + Treatment Score CES = 54.3 x Dyspnea + 47.8 x Xray + … + 10.9 x Abdominal pain Treatment Score = 46.8 x Antibiotics + 44.2 x Steroids + … + 4.9 x Ventilation (CPAP)
| Generic code Name | Product code Name | Category | |
|---|---|---|---|
| 225 | eCigarettes : nicotine Divise flavor unknown | E-cigarette Associated pulmonary illness | Nicotine |
| 276 | eCigarettes : nicotine Divise without Added flavors | E-cigarette Associated pulmonary illness | Nicotine |
| 226 | Other non-Drug substances | E-cigarette Associated pulmonary illness | Other |
| 155 | eCigarettes : Marijuana Divise flavor unknown | eCigarettes : Marijuana Divise flavor unknown | Marijuana |
| 88 | eCigarettes : nicotine Divise flavor unknown | eCigarettes : nicotine Divise flavor unknown | Nicotine |
| 57 | eCigarettes : nicotine Divise flavor unknown | Nicotine | |
| 43 | eCigarettes : nicotine Liquid flavor unknown | eCigarettes : nicotine Liquid flavor unknown | Nicotine |
| 40 | eCigarettes : Marijuana Liquid flavor unknown | eCigarettes : Marijuana Liquid flavor unknown | Marijuana |
| 32 | eCigarettes : Marijuana Divise flavor unknown | Marijuana | |
| 28 | eCigarettes : nicotine Divise without Added flavors | Elecrtonic Cigarettes | Nicotine |
Table 3: The 822 eCAPI cases were associated with 101 distinct Generic Code + Product Code combinations. These were mapped to 3 c
Table 3: The 822 eCAPI cases were associated with 101 distinct Generic Code + Product Code combinations. These were mapped to 3 categories, Nicotine, Marijuana and Other. Here are the top 10 GC+PC pairs and the Categories. Percent of cases associated with a: Nicotine product 84.9% Marijuana product 42.8% Both nicotine and marijuana products 31.5% Other substances 33.3%
| Source | LogWorth | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Analysis of Variance | ||||
|---|---|---|---|---|
| Source | DF | Sum of | Mean Square | F Ratio |
| Squares | ||||
| Model 6 295455.7 49242.6 11.1252 Error 814 3602937.9 4426.2 Prob > F C. Total 820 3898393.6 <.0001* |
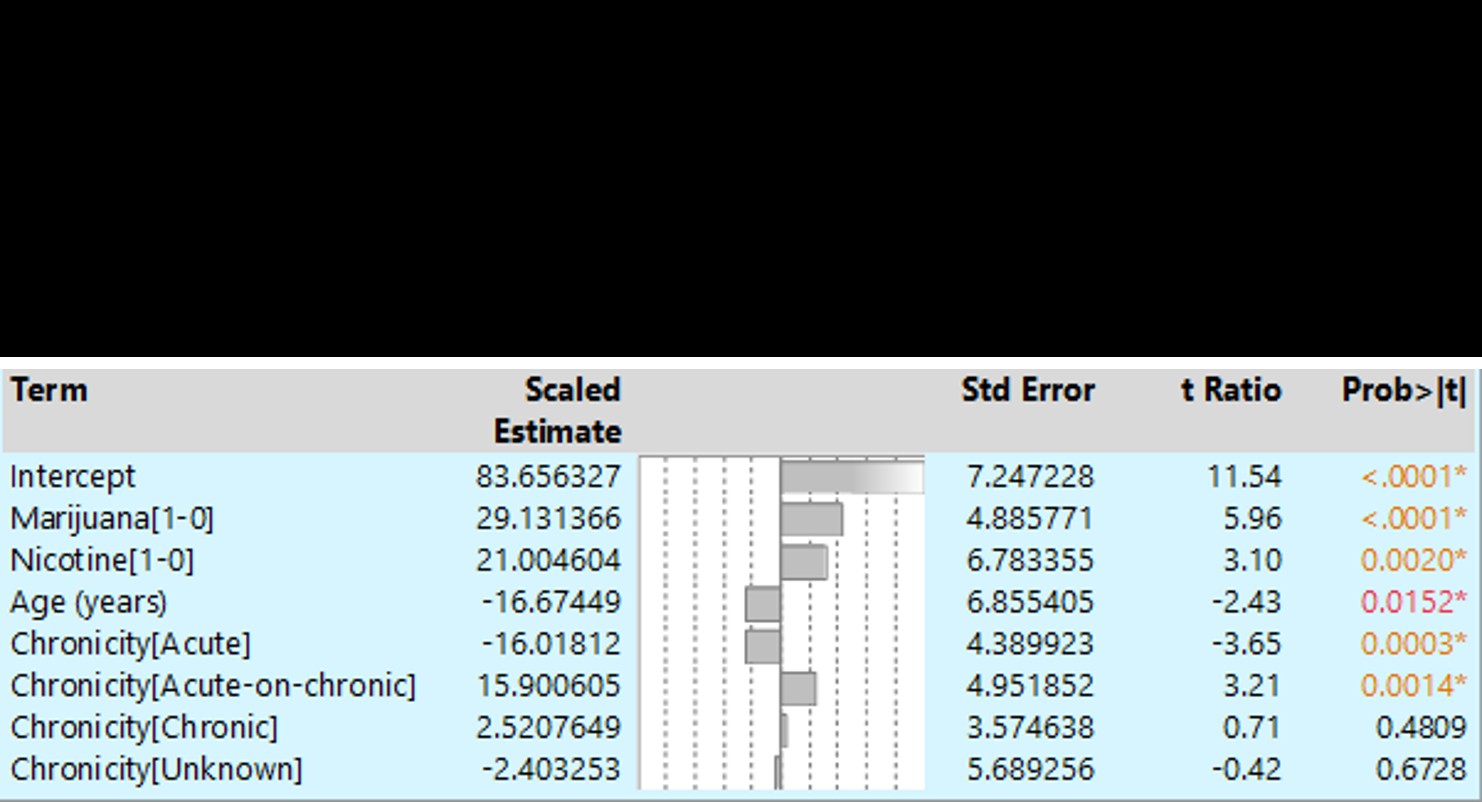
Neither the presence of flavoring additives nor further detail available for the marijuana products were associated with ECAPI severity.
Case Finding
Of the 23,252 e-Cig exposures (after excluding 211 EVALI cases from 23,463 total e-Cig cases), 133 (0.567%) had an ECS > median and 370 (1.57%) scored > 25%tile of EVALI cases (EVALI-25+). Figure 3 shows case number and “run chart” for the EVALI-25+ cases. The Case Number versus the case start date for the EVALI-25+ cases shows a notable
increase (inflection point) at the 120th case, 8/16/2019. The first value which exceeds the upper 95% confidence limit (run limit) was Week 478 (8/15-8/21/2019).
Start Date Case legend: x = EVALI score > median, x = EVALI > 25% tile but < median
Week Number Case legend: + = EVALI score > median, x = EVALI > 25% tile but < median Figure 3: Number of EVALI-25+ cases over time. Panel A shows Case Number versus Date for 231 EVALI-25+ cases -- the inflection point for this plot occurs with the 120th case, 8/16/2019. Panel B shows the number of EVALI-25+ cases by WEEK (6/24/2010 through 3/11/2020) and 95% run limit. First value above 95% run limit was Week 478 (8/15-8/21/2019).
Discussion
The aerosol produced by e-Cigs contains a veritable witches brew of chemicals which have only been partially described. Direct damage to the pulmonary epithelium has been shown and suggested a possible mechanism.1. Multiple case reports in the literature describe similar presentations, though most of those exposures were to nicotine [4, 5, 6].
We wondered what speculations might be washing around on social media. Here’s a Reddit e-cigarette comment posted 9 Sep 2019 “A new class of cutting agent diluent was introduced to the market. Thickeners. … sold under names such as “Viscosity” (TrueTerpenes), “Flavorless” (Floraplex), “Nexus”. These thickeners allow you to cut the shit out of your product and still sell it looking thick and perfect, like pure distillate and terps. Now this doesn’t work in the legal market, … say what you will about the state of the legal market in CA it’s actually pretty strict on the testing but black market. There’s no rules. My money is still either on one or more of the thickener products, or on some synthetic cannabinoid additive, or both.” Epidemiology Investigations of this type are arduous and time consuming. Development of a case definition can take time delaying case finding. In order to track suspect cases, the NPDS system introduced a special code to allow poison centers to tag these cases. Our analysis utilizes cases retrieved by use of this code [7, 8, 9].
Limitations: Both the measures of severity (CES) and substance classes used are quite crude, making the strength of association more surprising. Clearly there is a signal in the noise. NPDS is a passive reporting system and does not capture all cases. Poison center cases, in the main, were not confirmed. However, since most of the e-CAPI calls were from health care providers, the quality and detail may be better than those received from a lay caller.
When CDC reported vitamin E acetate oil as the culprit, officials described difficulties in collecting the EVALI cases from state health departments – they “had to write code for every single state to transfer the information into the CDC system” and “had to create a separate, parallel system exclusively using state department of health (DOH) data-to collect the information, which took several weeks” [7, 8, 9]. CDC’s rationale was state DOH cases had higher data quality, and could be tracked back and investigated. The timeliness of NPDS trumps this arduous process similar to onerous COVID-19 contact tracing. Since many poison center case records record the telephone number, PC cases can also be tracked back. This event should encourage public health agencies to utilize NPDS, especially in data collection.
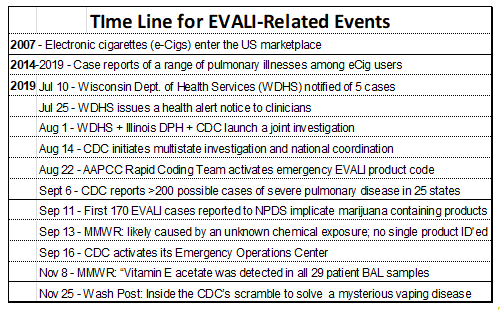
| Date | Event |
| 2007 | Electronic cigarettes (e-Cigs) enter the US marketplace |
| 2014 - 2019 | Case reports of a range of pulmonary illnesses among eCig users |
| 2019 | |
| 10-Jul | Wisconsin Dept. of Health Services (WDHS) notified of 5 cases |
| 25-Jul | WDHS issues a health alert notice to clinicians |
| 1-Aug | WDHS + Illinois DPH + CDC launch a joint investigation |
| 14-Aug | CDC initiates multistate investigation and national coordination |
| 22-Aug | AAPCC Rapid Coding Team activates emergency EVALI product code |
| 6-Sep | CDC reports >200 possible cases of severe pulmonary disease in 25 states |
| 11-Sep | First 170 EVALI cases reported to NPDS implicate marijuana-containing products |
| 13-Sep | MMWR: likely caused by an unknown chemical exposure; no single product identified |
| 16-Sep | CDC activates its Emergency Operations Center |
| 8-Nov | MMWR: Vitamin E acetate detected in all 29 patient broncho-alveolar lavage samples |
| 25-Nov | Wash Post: Inside the CDC’s scramble to solve a mysterious vaping disease |
Table 6: Timeline of major events in the evolution of EVALI.
Conclusion
The first 107 NPDS EVALI case scores were related to marijuana product exposure. This was confirmed via similar analyses for all 822 cases. The numbers of EVALI-25+ cases show a distinct increase in Aug-2019, suggesting EVALI was a newly emerging phenomenon among e-Cig users.
Acknowledgements: Avoiding identifying any of the authors prior to peer review.
References
-
Grana R, Benowitz N, Glantz SA (2013) Background paper on E-cigarettes (electronic nicotine delivery systems). Center for Tobacco Control Research and Education.
-
Stratton K, Kwan LY, Eaton DL (2018) Public health consequences of e-Cigarettes. National Academies Press, Washington, DC, USA.
-
Chatham-Stephens K, Taylor E, Melstrom P, Bunnell R, Baoguang W, et al. (2014) Calls to Poison Centers for Exposures to Electronic Cigarettes-United States, September 2010–February 2014. MMWR 63(13): 292- 293.
-
Arter ZL, Wiggins A, Hudspath C, Kisling A, Hostler DC, et al. (2019) Acute eosinophilic pneumonia following electronic cigarette use. Respir Med Case Rep 27: 100825.
-
Thota D, Latham E (2014) Case report of electronic cigarettes possibly associated with eosinophilic pneumonitis in a previously healthy active-duty sailor. J Emerg Med 47(1): 15-17.
-
He T, Oks M, Esposito M, Steinberg H, Makaryus M, et al. (2017) “Tree-in-Bloom”: Severe Acute Lung Injury Induced by Vaping Cannabis Oil. Ann Am Thorac Soc 14(3): 468-470.
-
Sun LH (2019) Searching for a killer: Inside the CDC’s scramble to solve a mysterious vaping disease. Washington Post.
-
Hajek P, Przulj D, Pesola F, Smith MK, Bisal N, et al. (2019) A Randomized Trial of E-Cigarettes versus Nicotine- Replacement Therapy. N Engl J Med 380(7): 629-637.
-
Schweitzer KS, Chen SX, Law S (2015) Endothelial disruptive proinflammatory effects of nicotine and ecigarette vapor exposures. Am J Physiol Lung Cell Mol Physiol 309(2): L175-L187.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells