Case Report of Rare cause of Acute Hemolytic Anemia in Saudi Patient (Babesiosis)
Babesiosis is one of the protozoan zoonotic diseases its presentation rang from asymptomatic to severe clinical conditions, with severe hemolysis. Immune status of the host and the species of the parasite has impact on the clinical presentations of the infected patient our patient is presented here; the patient was admitted from a countryside with severe anemia and a deterioration in his general condition, he was admitted to intense care unit and received blood transfusion, in addition to antimicrobial treatment in form of azithromycin and Ceftriaxon, his condition improve and released from ICU on the second day and discharge from hospital after improvement on the seventh day.
Case Report
On Examination
Male patient, 27 years old, and single. He was ill, irritable and in acute distress. He was conscious, alert and oriented. He was feverish, his temperature was 39°C, his blood pressure was 115/74mmHg with a heart rate of 90 beats/ minute, respiratory rate of 17 breaths/minute, and oxygen saturation of 97% in room temperature air, admitted to ICU for one day then discharge.
Laboratory Investigations
As regard his complete blood count (on admission). The clinically significant results are as follows:
- Red blood cell count (RBC) of 2.51M/µL (Low) (n 3.8- 4.8M/µL) with hemoglobin of 7.2gm/dL (n 13-17gm/ dL).
- White blood cell count (WBC) of 10.25k/µl (High) (n4- 10k/µL)
- Platelet count of 224K/µL (n 150-410K/µL)
- Reticulocytic count 2.7%
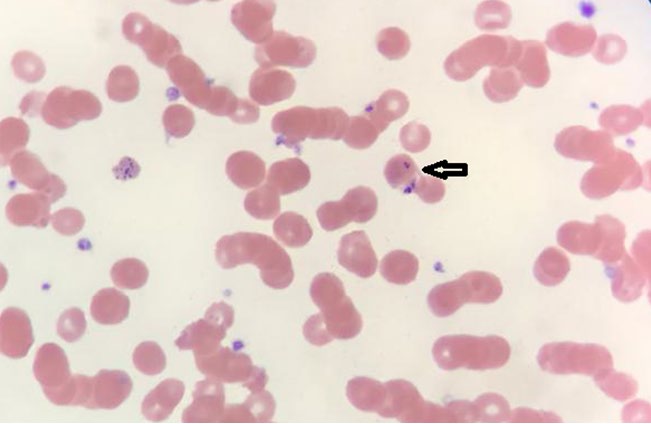
- Blood Film examination: +3 coarse inclusion bodies (Babesia is diagnosed by the pathognomonic appearance of maltese cross as in Figure 1 & 2.
- As regard his chemistry His random glucose of 124mg/ dL (n 70-140mg/dL)), calcium of 9.52mg/dL (n 8.6-
10.20mg/dL)
- SGOT (AST) of 154µ/L (n 15-37µ/L), SGPT (ALT) of 66µ/L (n 1-63µ/L), bilirubin (total) of 8.6mg/dL (0- 1.1mg/dL) direct bilirubin 1.52mg/dL (n 0-0.2).
- LDH: 337 u/l(81-234u/l)
- Coombs test: Negative
- Malaria rapid test: Negative.
- Blood culture: Negative
- Stool culture: Negative for shigellas & Salmonellas isolation
- As regard urine analysis
- Pus cells: Dark, Granular Cast (+), 51-90 WBCs/hpf, RBC: 20-30 RBCs/hpf, occult blood +3
- After one week (patient treated against babesiosis)
- Blood film negative for inclusion bodies
- AST: Normal
- LDH: 347u/l
- Total biluribin: Normal
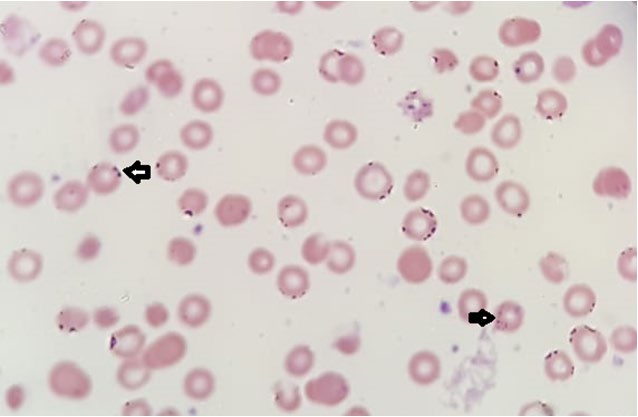
Figure1: Basophilic stippling +3 arrowed, polychromasia.
Discussion
Hemolytic anemia has a variety of causes that include extrinsic causes as infections, tumors, autoimmune disorders, medication side effects, leukemia, and lymphomas or intrinsic as sickle cell anemia and thalassemia patients [1]. Symptoms of hemolytic can be fatigue, fever, confusion, lightheadedness, dizziness, weakness, pale skin, or even in some cases up to heart failure. Differential diagnosis of hemolytic anemia includes many diseases such as all immune, autoimmune hemolytic anemia, drug induced, and infections [2]. An important clue in defining that hemolytic anemia is the cause if the anemia is an increased reticulocyte count that is not preceded by any bleeding or recent correction of iron or other nutrient deficiency. Signs of RBCs destruction can occur such as elevated lactate dehydrogenase enzyme and bilirubin levels, low haptoglobin level, and changed shape of RBCs [3], which in our case contain the Babesia organism. Human babesiosis is a zoonotic disease caused by organisms of the genus Babesia that can be transmitted through infected ticks’ bites, blood transfusions, or transplacentally. Genus Babesia has more than 100species and most of them only infect animals, so sparing humans except for some Babesia species that can be infectious to humans such as Babesia duncani, Babesia divergens, Babesia venatorum, Babesia sp. KO1, and Babesia microti. Babesiosis cases have been reported throughout the globe with Babesia divergens reported as the most common cause of babesiosis in Europe. Infected individuals may be asymptomatic or experience symptoms in which headache, nausea, vomiting, and fever are commonly experienced. Asymptomatic or persistent infections with Babesia microti can occur up to 2years. Persistent parasitemia can cause Babesia infections through blood transfusion and even organ transplantations whose cases are immunosuppressed who are at risk of severe persistent relapsing babesiosis. Other risk factors of developing severe Babesiosis include ages more than 50, splenectomy, malignancies, and HIV infection (immunocompromised patients) [4, 5].
The diagnosis of babesiosis is based on epidemiological and medical history, physical examination, and confirmatory laboratory tests. Travelling to a Babesia endemic area or blood transfusion in the last six months with symptoms of Babesiosis is helpful in diagnosing the disease. The main confirmatory test of Babesiosis is a Giemsa or Wright-stained blood films favorably examined at the beginning of symptoms as the parasitemia decreases thereafter. PCR is also used as it provides a better sensitivity and the ability to differentiate different species of the Babesia organism. Serological tests can be of use in supporting or confirming Babesiosis diagnosis. A recent infection can be detected by a rise of four folds in the Babesia IgG titer in the sera of patients in acute and convalescent stages of the disease. Serologic assays for Babesia diagnosis include ELISA, western blot, and the most used assay, indirect immunofluorescence assay [5].
Treatment for asymptomatic cases includes a course of one-week of atovaquone with azithromycin if the person is infected for more than three months [5]. Babesia microti resolves within 1-2 weeks with one course of atovaquone with azithromycin or clindamycin with quinine [4]. The treatment recommended for mild to moderate babesiosis cases is consisted of atovaquone with azithromycin for 7-10days. For patients with risk factors for developing severe Babesiosis, clindamycin plus quinine is the recommended choice. Prevention of babesiosis is required especially in immunocompromised individuals and others with risk factors of severe Babesiosis. Prevention of babesiosis can be achieved by avoidance of tick-infested areas such as forests, brushes, and areas with tall grass, in addition to spraying acaricides on these areas. No vaccine of Babesia is available for humans, but Babesia bovis and Babesia bigemina vaccines are available for cattle [5].
From this case of Babesiosis must be consider as one of the infectious agent causing acute hemolytic, as most of the patients come only by one attack almost all cases not full investigated , as most cases are sub clinical, and as postulated, babesiosis is self-limiting disease in some cases, but may be fatal in immucompromise host and splenectomy patients lack of practical experience to differentiate between (babesia) and basophilic stippling which caused by thalassemia anemia-chronic lead poisoning, megaloblastic anaemia. So the recommendation is to increase awareness for presence of babesiosis among Saudi community, and that will be by communication between health sectors like public health and detect its prevalence that of babesia in animals in the veterinary, to found infected animals, which will affect the regimen for blood transfusion screening and donor selection.
References
-
Li H, Guan D, Xu J, Jin E, Sun S (2020) Atraumatic splenic rupture was attributed to intra-cystic haemorrhage and hypersplenism in a patient with cirrhosis and portal hypertension: A case report. SAGE Open Med Case Rep 23: 8.
-
Phillips J, Henderson AC (2018) Hemolytic Anemia: Evaluation and Differential Diagnosis. Am Fam Physician 98(6): 354-361.
-
Xue J, He Q, Xie X, Su A, Cao S (2019) Clinical utility of targeted gene enrichment and sequencing technique in the diagnosis of adult hereditary spherocytosis. Ann Transl Med 7(20): 527.
-
Jia N, Zheng YC, Jiang JF, Jiang RR, Jiang BG, et al. (2018) Human Babesiosis Caused by a Babesia crassa-Like Pathogen: A Case Series. Clin Infect Dis 67(7): 1110- 1119.
-
Vannier EG, Diuk-Wasser MA, Ben Mamoun C, Krause PJ (2015) Babesiosis. Infect Dis Clin North Am 29(2): 357- 370.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths