The Conflict between Emerging SARS-Cov-2 Variants and the Potential Immune Response with Vaccination
The emergence of variants of the SARS-CoV-2 virus is certainly a serious threat to controlling the COVID-19 pandemic. After its irruption, some variants disappear or are irrelevant and others persist and are concerning because of its potential health repercussions and the immune response of vaccines that are being administered with great effort. One of the reasons why the SARS-CoV-2 virus is generating variants and will continue to do so is because a relatively few people in the world are immune and protected. The virus replicating is communicating to us that it is going to exhibit a lot of changes. Acquiring the infection involves risks of serious illness and death, so immunization is more logical, convincing and indispensable. It is also a better recourse for slowing viral replication, since infection offers viruses the opportunity to improve their performance. In addition, since multiple treatments, including antibody-based treatments, are often administered in severe infections, the surviving escape variants may be more resistant to these therapies effective against earlier versions of the virus. Two contenders (the surviving virus and the immune system) will be confronted with each other in an attempt to win, with the virus utilizing new weapons and subterfuges in a race that will lead to an evolutionary deadlock. A rising concern is whether available vaccines and those under investigation have a reduced or inadequate level of protection against emerging variants of SARS-CoV-2, particularly the variants of concern with changes in the spike protein. Despite these ongoing threats, at this time the general preventive measures and protection offered by the available SARS-CoV-2 vaccines are already a fundamental resource in the fight against COVID-19 and its variants, and a very hopeful measure for the immediate future. In the current situation, people should be aware of and learn to live with the virus variants and how to optimize its prevention and control.
Introduction
Protection against COVID-19 is largely based on an immune response targeted against the spike protein of this virus. The variants arising from this spike protein that increase the viral load that an infected person is able to spread, or that favor its affinity for ECA2 receptors, are likely to result in increased transmission of the virus. Furthermore, identical or related changes may alter the shape of spike protein, compromising or damaging the binding sites of the neutralizing antibodies generated either from past infection or through vaccination.
The information that is coming on SARS-CoV-2 variants is being broad and constant with particular focus on areas where they are prevalent, whether they cause more severe disease, if it enhances the transmission, and the possible resistance to available vaccines. But there is insufficient disclosure of information, also of general interest, on why the emerging variants are important from a population perspective, and how this impact at the individual level once the vaccination program is in progress.
There is speculation whether it is possible for vaccines to provide broader immunity to variants than that achieved solely by infection with the original virus. Regardless of the platform on which the vaccine is based, the point is that there is a particular antigen and a virus that changes. Sooner or later, will a mutant arrive that evades it?.
In a more optimistic view, it is also not possible in predicting whether less pathogenic variants will appear and dominate, as many mutations of the virus have little or no impact on transmission capacity and disease.
Living with Variants
As with other RNA-encoded viruses, which exhibit a very high mutation rate, the coronavirus uses the RNA polymerase (replicase) machinery to self-replicate. A process that is also prone to copying errors when replication occurs in the invaded cells (frequently repeat what they think have learned), so mutations will be generated more frequently during infections [1].
It was not a surprise when SARS-CoV-2 variants began to emerge because virologists are very familiar with the fact that viruses usually experience changes in their normal behavior when replicating in order to survive. And precisely their survival is conditioned to the availability of a sufficient number of persons susceptible to be infected in order to replicate easily, and a higher replication rate implies that more mutations are present, often destroying cells [2]. During this process and with the corresponding reaction of the immune system, the symptoms of infection will appear and if this defensive activity fails to control the microorganism, the person may not survive. Fortunately, infections of lower severity seem to be associated with a reduced replication of the virus [3].
The SARS-CoV-2 virus attempts to evade the obstacles of the immune system of the person that it is infecting through two strategies in an effort to survive: 1) By finding new susceptible people who did not pass the infection or are not vaccinated to infect them more efficiently and spread the replication of their genome. As more people become immune to the virus after passing the infection or after vaccination, the pressure for the virus to survive is greater. It has a harder time. 2) By camouflaging or modifying their appearance through genetic changes, of sequence in key positions, varying its surface proteins so that the immune system cannot identify them. It is also propitiated if the virus encounters specific resistance or pressures from neutralizing antibodies (NAB) at levels that are still insufficient to eliminate the infection, from previously infected persons or vaccinated (those very recently vaccinated or recipients of a first dose pending the second dose) [4]. With each infection, the virus has a chance to change and “outgrow itself” in a way that increases the pool of susceptible people. For people, this means that if the virus succeeds and mutates, it may enhance its ability to generate infections, facilitate infection of more people and/ or make susceptible those previously immune (infected by original strains of the virus).
As comforting detail, of the more than one million of distinct SARS-CoV-2 virus sequences reported to the Global Initiative on Sharing All Influenza Data (GISAID) database [5], many mutations are unremarkable and do not represent the emergence of a viable variant. A small number will do so by changing the amino acids, the basic components of viral proteins, modifying their characteristics.
They become new, high-profile versions that will continue to spread, often termed “mutants or evasion or escape variants” and with a new name, different from those currently circulating and allowing the virus to evade the immune system.
The escape variants are only successful if, in addition to the structural modification acquired in the spike protein that attempts to avoid existing antibodies, retain the functional integrity of the virus. That is, it cannot alter or lose its necessary ability to bind to the ACE2 receptor that allows it entry into cells. Thus, individual changes are usually small. But over time, such changes can accumulate, resulting in different identifiable traits of viruses that are more frequent and less susceptible to existing treatments or vaccine- induced immunity. Unusual variants have been reported when the virus replicates at high levels for prolonged periods in immunocompromised patients [6].
With so much information coming in with respect to coronaviruses from scientific and non-scientific sources, the terminology used for viral modification can lead to confusion with indistinct use of expressions. A new variant may arise when specific mutations, or sets of mutations, are selected after numerous cycles of viral replication. If the sequence of variation generates a virus with different phenotypic traits, the variant is called a strain. If genetic sequencing and phylogenetic analysis detect a distinct variant as a different branch, a new lineage is created [7].
Variant Types
The European Centre for Disease Prevention and Control (ECDC) and the Centers Of Diseases and Control (CDC) (Table 1) [8, 9] have classified the current SARS-CoV-2 variants (with some difference in criteria) by their characteristics regarding cellular receptor binding, response to NAB or available treatments, potential impact on diagnosis, and likelihood of being more easily transmitted or causing more severe disease. Recently, the WHO assigns simple names to the predominant variants, easy to pronounce and remember especially by the non-scientific sector, using letters of the Greek alphabet [9].
Variants of Concern (VOC): There is conclusive evidence of being more infectious or causing more severe disease than other circulating coronaviruses. They have an impact on transmission, severity and/or immunity with likely repercussions on the epidemiological scenario. The pooled genomic, epidemiological and in vitro evidences for these attributes invoke at least a degree of confidence.
• Alpha (B.1.1.7) y B.1.1.7+E484K. Originated in the United Kingdom. They spread very rapidly, and it was estimated that could be more severe. However, some studies have not found that infected persons have more severe symptoms or a higher risk of developing a prolonged illness compared to those infected with original strains [10].
• Beta (B.1.351). Arising in South African. Transmitted more rapidly and is relatively resistant to NAB after vaccination or infection and to monoclonal antibodies.
• Gamma (P.1) From Japan and Brazil. Shows a reduced neutralization by convalescent or vaccine sera.
• Delta (B.1.617.2): Arising in India. It is one of three distinct sublineages of B.1.617 variant that have distinct mutation profiles and warrant individual estimation to understand their behavioral differences. In addition to being the most common variant reported in that country, it has already expanded quickly to other countries. Delta variant grows very rapidly in the respiratory tract and with a very high viral load (about 1000 copies more than those infected with the original virus) [11]. There is as yet no evidence that it is more lethal or has different symptoms to Alpha variant. There are also no data available on in vitro neutralization to determine possible immune escape against serum from previously infected or vaccinated individuals.
Variants of interest (VOI): They present certain genetic markers associated with the previous mentioned characteristics, with potential impact on transmission, severity and/or in evading immunity. These descriptions are still preliminary or raise unresolved questions.
• Epsilon (B.1.427 and B.1.429). Originated in the United States, spread rapidly in this country, and was somewhat less susceptible to NAB from vaccination or infection. According to the ECDC’s criteria, these variants are not currently protagonists and are designated as variants de-escalated, due to their scarce circulation and with scientific evidence that they no longer present characteristics of concern [8].
• B.1.617. Originated in India and with an exponential increase of cases occurring in that country. Of its three sub-lineages, B.1.617.1 (Kappa) and B.1.617.3 are being investigated as functionally significant if such high increase is linked to the coincidence of a triple modification of three mutations: E484Q/L452R/P681R [12]. The B.1.617.3 variant, which has little impact in the European community, is considered to be under surveillance in the United Kingdom. The main factor in spreading these variants is the behavior of the population, and in India there are favorable conditions due to overcrowding, movement of people, large gatherings and population displacements for religious and politics events. Further, propitiated by false confidence with a message that COVID-19 was essentially under control delaying the initiation of India’s vaccination campaign against COVID-19 and with a very low percentage of the population immunized [13, 14].
| Variants | ECDC | CDC | Origin Country | Main Mutation (RBD) | Transmission Impact | Severity Impact | Immunity Impact |
|---|---|---|---|---|---|---|---|
| Alpha (B.1.1.7) | VOC | VOC | United Kingdom | N501Y, K417N | Yes | Potential↑ | Minimal |
| B.1.1.7+E484K | VOC | United Kingdom | N501Y, E484K | Yes | Potential↑ | Minimal | |
| Beta (B.1.351) | VOC | VOC | South Africa | E484K, N501Y, K417N | Yes | Yes | Reduced |
| Gamma (P.1) | VOC | VOC | Japan/Brazil | E484K, N501Y, K417T | Yes | Yes | Reduced |
| Delta (B.1.617.2) | VOC | VOC | India | L452R, T478K, P681R | Yes | Uncertain | Potential↓ |
| Epsilon (B.1.427/B.1.429) | VDE | VOI | United States | L452R | Unclear | Uncertain | Minimal/ Reduced |
| B.1.617 | VOI | VOI | India | L452R, E484Q | Yes | Uncertain | Potential↓ |
| Kappa (B.1.617.1) | VOI | VOI | India | L452R, E484Q, P681R | Yes | Uncertain | Potential↓ |
| B.1.617.3 | VUM | VOI | India | L452R, E484Q, P681R | Yes | Uncertain | Potential↓ |
| Eta (B.1.525) | VUM | VOI | Nigeria | E848K. D614G, Q677H | No Evidence | No Evidence | Neutralization |
| Lota (B.1.256) | VUM | VOI | United States | E848K, D614G, A701V, L452R | No Evidence | No Evidence | Reduced/ Neutralization |
| B.1.426.1 | VUM | VOI | United States | L452R, D614G | No Evidence | No Evidence | Reduced/ Neutralization |
| Zeta (p2) | VUM | VOI | Brazil | E484K, D614G, V1176F | No Evidence | No Evidence | Reduced/ Potential↓ |
Table 1: SARS-CoV-2 variants of major relevance (August 2021) [8,9].
VOC: Variants of concern, VOI: Variants of interest, VUM: Variants under monitoring, VDE: Variants de-escalated, RBD: Receptor binding domain Table 1: SARS-CoV-2 variants of major relevance (August 2021) [8, 9].
Variants under monitoring: Are those detected in at least one outbreak and as signals or warnings according to epidemiological information, tracking of established genomic variants or preliminary scientific data. In August 2021, 22 variants with this definition are being studied and considered by ECDC [8]. In June 2021 a new variant, Delta Plus (B.1.617.2.1 or AY.1), was reported in India. This new version of the Delta VOC variant is generating attention and uncertainty whether it will perform similarly or worse than its relative in transmissibility, severity and response to vaccines. Delta Plus shares a mutation, K417N, with other variants of the virus including the Alpha and Beta VOCs but is not expected to play a major role. At present, that new variant is under surveillance and there is not yet enough evidence to indicate it as a major threat. Variants of high consequences: Of enormous transmission and with clear evidence of a significantly reduced response to NAB generated by natural infection or vaccination with original circulating strains. At present, there are no SARS- CoV-2 variants that reach this level of impact.
The Expected Immune Response of the Vaccines against SARS-CoV-2
It should not be forgotten that individuals become immune only after they have passed the infection or after vaccination. In addition, the NAB response to SARS- CoV-2 virus differs depending on how the antibodies were generated: after a naturally acquired infection or from a COVID-19 vaccine. The adaptive immune system is complex, raising the question of which type of immunity develops in people with acquired natural immunity who are vaccinated. The concurrence of both types of immunity, or “hybrid immunity”, is particularly of interest.
The available vaccines are based on spike protein of virus, the focus of the NAB generated [2]. This acquired protection as with natural infection, largely mediated by humoral immunity, is enhanced and complemented by cell memory immunity of great importance and less mentioned in considering the immune response to SARS-CoV-2 memory B cells and proliferation of specific memory CD4+ and CD8+ T lymphocytes, both in the circulation and tissues. COVID-19 vaccines that have been developed to prevent clinical infection and/or severity of disease caused by the original virus show that after a second dose, induce an amnesic or delayed immune response against the spike protein, and produce elevated levels of NAB comparable or higher than those observed once the infection passed [14]. Recent studies reveal that most infected individuals with even mild disease develop a robust, durable, and polyvalent T-lymphocyte immunity months after infection, even with decline of NAB, which has implications for durability of immunity and future vaccine projects [16, 17]. The antiviral memory lymphocytes are primed for a coordinated response to SARS-CoV-2 re- exposure that could contribute to immunity and help to curb the pandemic.
Variants of Concern and Interest and Eventual Protection with Available Vaccines
There are already reports suggesting certain optimism about a favorable effect of the vaccines, taking into account the type of vaccine and variant. For example, subjects immunized with two doses of the AstraZeneca AZD1222 vaccine showed a lower median of NAB than those acquired after two doses of the Pfizer BNT162b2 vaccine, against Alpha, Beta, and Delta variants [18]. Recently a preprint study indicates that after the second dose of the Pfizer BNT162b2 vaccine, it induces a cross-neutralization of the circulating Alpha and Beta variants. Enough against the Alpha variant and a 5-fold reduction of the Beta variant, but still showing a modest (> 20) neutralization titer [19]. Sera from immunized with one dose of the Janssen Ad26.COV2.S vaccine showed a neutralizing activity, although reduced, against Alpha, Beta, Gamma, and Delta VOCs. The most accentuated reduction was with the Beta and Gamma variants and the lowest against Delta, suggesting that the efficacy with one dose of this vaccine would be preserved against this VOC [20].
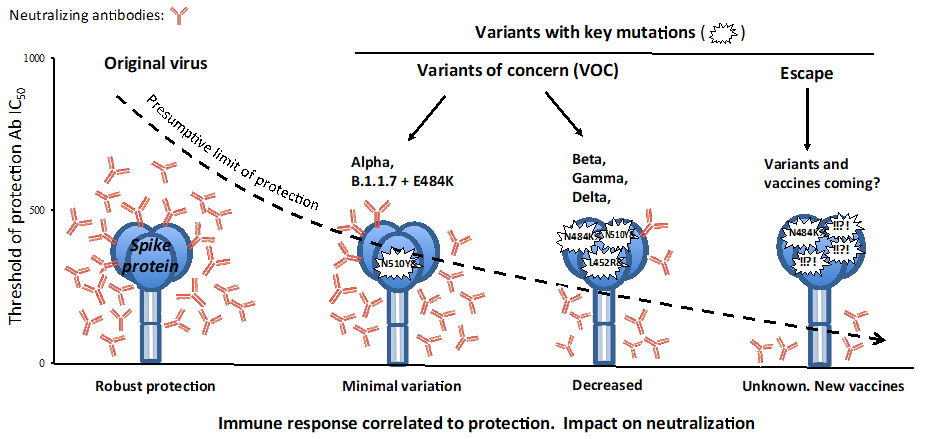
Against these variants there is still no known cut-off point to indicate what level of antibody is needed to achieve optimal protection. It is unclear whether a reduction in neutralizing activity means that the vaccines will be ineffective, although it is expected that despite such a reduction, the immune response observed will be sufficiently high to confer protection even if there are changes in the antigenic sites of the SARS-CoV-2 variants (Figure 1). At the time of writing, some information is available:
- Beta (B.1.351) variant: Vaccines of mRNA have shown an antibody response up to 6 times and 20-30% (depending on vaccine) lower than those achieved against the original strains. This level of antibody achieved is still significant enough to be able to protect against COVID-19, or at least against the most severe disease after full vaccination [2, 21]. A nanoparticle vaccine (NVX-CoV2373, Novavax) was effective and induced significant cross-protection during the course of the pandemic where there was a dominant circulation of this variant [22]. However, after two doses with the AstraZeneca vaccine, the NAB response was substantially diminished, with no efficacy against non-severe disease, but a broad T-cell reaction was preserved, providing a potential protection against more severe cases [23].
- Alpha (B.1.1.7) and B.1.1.7+E484K variants: According to some preliminary studies, these variants do not show particular resistance and are becoming susceptible to NAB generated by mRNA vaccines and with an immune activity (in particular against Alpha) lasting several months [3, 24, 25]. Also, the AstraZeneca AZD1222 vaccine continues to protect people from infection with the Alpha variant even though there is a decrease, but still effective, in the NAB titers achieved. Furthermore, the T-lymphocyte immune responses dampen or stop symptoms even if infection occurs [26]. In a recent study, Alpha and Epsilon -B.1.429- VOCs were effectively neutralized with serum samples from vaccinated with inactivated virus (CoronaVac Sinovac Biotech). These results are in accordance with those obtained in other investigations using sera from both mRNA-immunized and inactivated virus vaccines. However, other circulating VOCs carrying the E484K mutation showed a very low level of neutralization from sera of individuals who received the inactivated virus vaccine [27].
- Gamma (P.1) variant: The impact of the vaccines remains to be confirmed in clinical studies. A small laboratory study with mRNA vaccine sera showed a good and equivalent neutralization of both this variant and the Alpha variant [28].
- B.1.617 variants: There are promising data according to early studies, showing that existing vaccines should be effective. Sera from convalescents of COVID-19 cases and vaccinated persons (specifically with vaccine BBV152- Covaxin) were able to neutralize the B.1.617 variant, at that time under investigation, and with a similar capacity [29]. The Delta VOC, which is spreading rapidly worldwide, requires urgent information about the vaccine immune response. Recently a study from Public Health England suggests that two doses of Pfizer BNT162b2 y AstraZeneca AZD1222 vaccines offer high levels of protection against symptomatic disease and hospital admission with the Delta variant [29]. In another study a significant majority of serum samples from COVID-19 convalescents and all samples from mRNA vaccine recipients showed neutralizing activity still above the threshold of detection against Delta and Kappa variants for three months after infection or after administration of second doses of vaccine (Figure 1) [30].
In fact, with vaccines that require two doses to achieve maximum efficacy, the NAB may already be detected after the first dose, but serum titers increase significantly with the second dosage. Thus, virus replication will be suppressed since a weak response of NAB will have little effect on replication [3]. As soon as each person receives the increased protection conferred through the second dose of the vaccine, the better it will be for individuals as well as for the population. Some inactivated vaccines such as those developed in China and India appear to induce lower levels of antibodies and could theoretically be less effective [4].
Variants will Not Cause Serious Illness in Most People Who have Recovered from COVID-19
Especially if they receive the immunization sometime after infection has passed. In persons already infected with the original virus and now recovered, the level of antibodies reached after vaccination will be important to prevent reinfection with new variants. In order to increase the levels of antibodies that may have declined after infection, it has been reported that one dose of mRNA vaccines, may result in increased but short-lived reactogenicity, such as headaches and fever. This is attributed to a very high and rapid rise in antibodies because vaccination is especially potent in people who have already been infected (hybrid immunity). Importantly, these individuals after one dose of mRNA vaccines exhibit an increased memory B and T cell response and an effective NAB against Alpha and Beta variants. It was also reported that immunization with mRNA and AstraZeneca AZD1222 vaccines in recovered individuals elicits a durable immune response above the neutralization threshold against Alpha, Beta and Delta variants [31, 32, 33, 34]. More evidences are needed to confirm these findings. It seems prudent to question whether a second dose of these mRNA vaccines is necessary in those who have passed the infection.
Effect of Vaccines on Transmission of New Variants
Generally, all vaccines that have been shown to be effective in reducing and controlling other types of infections different to SARS-CoV-2, have a significant impact on decreasing transmission. It is therefore to be expected that anti-COVID-19 vaccines will also reduce transmission of the virus. There is increasing evidence to support this idea. Studies carried out in the United Kingdom and Israel (with predominant circulation of variant Alpha) among healthcare workers immunized with the mRNA vaccine Pfizer BNT162b2 when compared to unvaccinated participants, reveal a significant reduction in symptomatic and asymptomatic SARS-CoV-2 infection 3 weeks after the first dose and more than 7 days after the second dose of vaccine. An important indicator of reduced transmission [35, 36]. Interestingly also in Israel and following immunization with an mRNA vaccine, the viral load decreased substantially in infections that occurred between 12 and 37 days after the first dose of vaccine. This reduction in viral load in nasal swabs points to potentially lower infectivity and a further contribution to vaccine efficacy in virus transmission [37]. However, a remarkable feature of Delta variant, due to its high viral load, is that the spread is very fast, it is very infectious during the initial stage of infection, such as in asymptomatic or minimally symptomatic periods, with the risk and impact that it implies on disease transmission [11]. Given the potential role of asymptomatically infected persons in the progression of the COVID-19 pandemic, the effect of that post-vaccination reduction in the silent spread of SARS-CoV-2 infection will certainly have important implications for preventing transmission in the population and an undoubted public health benefit. Hoping this effect continues to be realized.
Optimizing the Protection against New Variants.
To date, most studies on antibodies blocking SARS-CoV-2 have been based on those targeting the receptor binding domain (RBD) region of the spike protein, the component that attaches to human cells. This was the basis for research on antibodies specifically targeting this site, and able to effectively combat the SARS-CoV-2.
A new study Voss WN, et al. [38] examined the full spectrum of antibodies against the spike protein from patients recovered from COVID-19. Most of the antibodies were directed to different parts of this protein other than RBD. Concretely, the N-terminal domain area (NTD) and the S2 subunit. The remarkable feature is that the NTD zone is precisely where the spike protein has mutated frequently, especially in Alpha and Beta VOCs, suggesting that have mutated at that point to evade antibodies directed against the RBD zone. In relation to the S2 subunit, this region is not as mutable as the NTD area, indicating that antibodies directed here could offer an umbrella of protection against a wider selection of variants. Moreover, the authors note, the S2 subunit could represent an ideal target for future vaccines, as this portion is highly conserved in SARS-CoV-2 and related coronaviruses. An optimal immune response would not only concentrate in the RBD zone, implying the need to generate new vaccines that produce antibodies capable of reaching all areas of the spike.
However, it is conceivable that vaccines may provide a different and broader immunity to variants than that achieved only after passing infection with the original virus. In comparison to the antibodies acquired after natural infection, there is already some evidence showing that the protective antibodies generated by a particular mRNA vaccine target a broader spectrum of variants carrying specific changes in a key portion of its spike protein. In particular, these antibodies are more concentrated and at a greater variety of loci, on the RBD region [39]. Against the circulating variants, it is therefore possible to conjecture that the immunity acquired after vaccination will offer a not insubstantial protection. And it is also a reaffirmation regarding the benefit of vaccination in people already recovered from SARS-CoV-2 infection.
The constant information that is coming in about new variants, with the resulting uncertainty, underscores the importance of the race between a broad and sufficient immunization and the natural selection of potential escape mutants. One form of masking SARS-CoV-2 as detected in two variants (Alpha and Beta) according to a pre-print study [40], is through its potential ability to induce a rapid cell fusion. That is, it spreads from cell to cell resulting in supercells or syncytia, multinuclear cell compartments with clustered nuclei. Thus the variants become more resistant to NAB already circulating, delaying the elimination of the virus or favoring the persistence of infection. Ideally, antibodies generated by natural infection or a vaccine should be present prior to exposure to a hypothetical variant so that a strong and long-lasting NAB response can act at contagion and before the virus infects cells with potential risk of intercellular spread. Since antibody response requires several weeks to reach an optimal level of activity, or a particular vaccine generates a lower neutralization capacity, if contagion occurs in this interval, the cells could already be infected and generates syncytia. Neutralization by antibodies may not be effective in the same way in all cells and compartments. The virus doesn’t come out, it is hidden in a factory where it replicates. Fortunately, it is then that the intervention of cellular immunity of T lymphocytes mediated by the vaccine becomes important to eliminate these cellular reservoirs refractory to the antibodies.
Research progress is inexorable. Most of the life cycle processes of RNA viruses such as SARS-CoV-2 are aimed at multiplying, transporting and delivering their RNA to new cells. It has been shown that these viral genes cannot encode all the proteins necessary to perform its mission, so the viruses to attach their RNA utilize cellular binding proteins (CBPs) from the host. These proteins are key regulators of the virus life cycle, limiting or initiating infection. The response would be to search for drugs or vaccines targeting these CBPs that interact with SARS-CoV-2 RNA to inhibit the infection with the risk of new variants [41].
Fortunately, children will be the next candidates to be vaccinated as key players in protecting both themselves and the community. In the time of writing, immunization of children over 12 years of age is imminent and clinical trials are underway in children over 6 months of age. Although COVID-19 is not completely benign in them, with much lower hospitalization and case fatality rates than in adults [42], it is clear that children can carry a potential viral load and be transmitters. But also the response of their immune system after the age of infancy and presumably after vaccination is usually more potent and more persistent than in adults, thus generating a virus-resistant population with reduced circulation of the virus and its variants [43].
Conclusion
Vaccination should not be postponed because of uncertainty with the new variants. It must be accepted that the mentioned reduction in vaccine efficacy of some of them which will probably continue to appear in the future does not mean that the vaccines are completely ineffective. This should be mitigated or solved, and so it is being studied, with booster vaccination (if the loss of immune protection is finally demonstrated after months), by the modification and design of vaccines of new generation with mutations in the sequences of the spike protein, and using alternative viral antigens or bivalent vaccines (1:1) with a VOC and the original strain.
The control and eventual eradication of SARS-CoV-2 will depend on the acceptance of vaccination by the majority of people. An easy message to convey: As more people are vaccinated and protective measures are maintained, there is confidence that virus circulation will decrease significantly, resulting in fewer mutations. In short, considering the missed opportunities that the virus could encounter as the number of non-susceptible people increases, achieving herd immunity, including children, is essential. But it is unknown how long natural immunity lasts and whether it is equally protective against emerging variants of SARS-CoV-2. And attaining herd immunity to reach control through natural infection alone is a long and painful process that was not achieved with other infections such as smallpox and measles, for example, without the contribution of universal vaccination. Furthermore, the planned initial target of 70% of the population vaccinated, given the behavior of SARS-CoV-2 and the idiosyncrasy and behavior of different population groups and countries, it will be insufficient and complicated to control the pandemic.
If someone is protected and cannot become infected, the virus will not replicate and therefore mutate. That person already represents a barrier to the spread of the virus. If more effective obstacles exist in a community, the spread of infection will be slower and more difficult, with fewer opportunities to regain the control with mutants. A national action is not enough; it must be a global action by all countries, because those that do not eliminate the virus well represent a threat to the rest. The global response must be prompt and science-based [44].
The available resources, with results that are being successful, are what they are, while continuing to be improved. We are all safe only if everybody is safe.
Declarations
- Ethics approval and consent to participate: No applicable
- Consent for publication: No applicable.
- Availability of data and materials: No applicable
- Funding and competing interest: No funding was provided for this manuscript. Author declares no conflict of interest.
- Authors’ contributions: No applicable
- Acknowledgements: No applicable
References
-
Belshaw R, Gardner A, Rambaut A, Pybus OG (2008) Pacing a small cage: mutation and RNA viruses. Trends Ecol Evol 23(4): 188-193.
-
Rubin R (2021) COVID-19 Vaccines vs Variants— Determining How Much Immunity Is Enough. JAMA 325 (13): 1241-1243.
-
Moore JP (2021) Approaches for Optimal Use of Different COVID-19 Vaccines. Issues of viral variants and vaccine efficacy. JAMA 325(13):1251-1252.
-
Moore JP, Offit PA (2021) SARS-CoV-2 Vaccines and the Growing Threat of Viral Variants. JAMA 325(9): 821-822.
-
Maxmen A (2021) Popular genome site hits one million coronavirus sequences. Nature 593(7857): 21.
-
Kemp SA, Collier DA, Datir RP, Ferreira I, Gayed S, et al. (2021) SARS-CoV-2 evolution during treatment of chronic infection. Nature 592(7853): 277-282.
-
Mascola JR, Graham BS, Fauci AS (2021) SARS-CoV-2 Viral Variants—Tackling a Moving Target. JAMA 325(13): 1261-1269.
-
(2021) European Centre for Disease Prevention and Control. SARS-CoV-2 variants of concern as of 5 August 2021.
-
(2021) Centers Of Diseases and Control. SARS-CoV-2 Variant Classifications and Definitions**.** Updated August 10, 2021.
-
Frampton D, Rampling T, Cross A, Bailey H, Heaney J, et al. (2021) Genomic characteristics and clinical effect of the emergent SARS-CoV-2 B.1.1.7 lineage in London, UK: a whole-genome sequencing and hospital-based cohort study. Lancet Infect Dis S1473-3099(21).
-
Li B, Deng A, Li K, Hu Y, Li Z, et al. (2021) Viral infection and transmission in a large well-traced outbreak caused by the Delta SARS-CoV-2 variant. MedRxiv Preprint.
-
Cherian S, Potdar V, Jadhav S, Yadav P , Gupta N, et al. (2021) Convergent evolution of SARS-CoV-2 spike mutations, L452R, E484Q and P681R, in the second wave of COVID-19 in Maharashtra, India. MedRxiv Preprint.
-
Thiagarajan K (2021) Why is India having a covid19 surge?. BMJ 373: n1124.
-
(2021) India’s COVID-19 emergency. The Lancet 397(10286): 1683.
-
Stephens DS, McElrath MJ (2020) COVID-19 and the path to immunity. JAMA 324(13): 1279-1281.
-
Jagannathan P, Wang TT (2021) Immunity after SARS- CoV-2 infections. Nat Immunol 22(5): 539-540.
-
Jung JH, Rha MS, Sa M, Choi HK, J Jeon JH, et al. (2021) SARS-CoV-2-specific T cell memory is sustained in COVID-19 convalescent patients for 10 months with successful development of stem cell-like memory T cells. Nat Commun 12(1): 40-43.
-
Wall EC, Wu M, Harvey R, Kelly G, Warchal S, et al. (2021) AZD1222-induced neutralising antibody activity against SARS-CoV-2 Delta VOC. Lancet 398(10296): 207-209.
-
Jalkanen P, Kolehmainen P, Häkkinen HK, Huttunen M, Tähtinen PA, et al. (2021) COVID-19 mRNA vaccine induced antibody responses against three SARS-CoV-2 variants. Nat Commun 12(1): 3991.
-
Jongeneelen M, Kaszas K, Veldman D, Huizingh J, Van der Vlugt R, et al. (2021) Ad26.COV2.S elicited neutralizing activity against Delta and other SARS-CoV-2 variants of concern. BioRxiv Preprint.
-
Wu K, Werner AP, Moliva JI, Koch M, Choi A et al. (2021) mRNA-1273 vaccine induces neutralizing antibodies against spike mutants from global SARS-CoV variants. BioRxiv Preprint.
-
Shinde V, Bhikha S, Hoosain Z, Archary M, Bhorat Q, et al. (2021) Efficacy of NVX-CoV2373 Covid-19 vaccine against the B.1.351 variant. N Engl J Med 384(20): 1899- 1909.
-
Madhi SA, Baillie V, Cutland CL, Voysey M, Koen AL, et al. (2021) Efficacy of the ChAdOx1 nCoV-19 Covid-19 vaccine against the B.1.351 variant. N Engl J Med 384(20): 1885-1898.
-
Liu Y, Liu J, Hongjie X, Zou J, Weaver SC, et al. (2021) Neutralizing Activity of BNT162b2-Elicited Serum. N Engl J Med 384(20): 1466-1468.
-
Edara VV, Hudson WH, Xie X, Ahmed R, Suthar MS (2021) Neutralizing antibodies against SARS-CoV-2 variants after infection and vaccination. JAMA 325(18): 1896- 1898.
-
Emary KRW, Golubchik T, Aley PK, Ariani CV, Angus B, et al. (2021) Efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine against SARS-CoV-2 variant of concern 202012/01 (B.1.1.7): An exploratory analysis of a randomized controlled trial. Lancet 397(10282): 1351-1362.
-
Chen Y, Shen H, Huang R, Tong X, Wu C (2021) Serum neutralizing activity against SARS-CoV-2 variants elicited by CoronaVac. Lancet Infect Dis 21(8): 1071-1072.
-
Yadav PD, Sapkal GN, Abraham P, Ella R, Deshpande G, et al. (2021) Neutralization of variant under investigation B.1.617 with sera of BBV152 vaccinees. Clin Infect Dis Ciab 411.
-
Stowe J, Andrews N, Gower Ch, Gallagher E , Utsi L et al. (2021) Effectiveness of COVID-19 vaccines against hospital admission with the Delta (B.1617.2) variants. N Engl J Med 385(7): 585-594.
-
Edara VV, Lai L, Sahoo MK, Floyd K, Sibai M, et al. (2021) Infection and vaccine-induced neutralizing antibody responses to the SARS-CoV-2 B.1.617.1 variant. BioRxiv Preprint.
-
Stamatatos L, Czartoski J, Wan YH, Homad LJ, Rubin V, et al. (2021) Antibodies elicited by SARS-CoV-2 infection and boosted by vaccination neutralize an emerging variant and SARS-CoV-1. Science eabg9175.
-
Krammer F, Srivastava K, The PARIS team, Simon V (2021) Robust spike antibody responses and increased reactogenicity in seropositive individuals after a single dose of SARS-CoV-2 mRNA vaccine. MedRxiv Preprint.
-
Reynolds CJ, Pade C, Gibbons JM, Butler DK, Otter AD, et al. (2021) Prior SARS-CoV-2 infection rescues B and T cell responses to variants after first vaccine dose. Science eabh 1282.
-
Planas D, Veyer D, Baidaliuk A, Staropoli I, Guivel- Benhassine F et al. (2021) Reduced sensitivity of SARS- CoV-2 variant Delta to antibody neutralization. Nature 596(7871): 276-280.
-
Hall VJ, Foulkes S, Saei A, Andrews N, Oguti B, et al. (2021) COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): a prospective, multicenter, cohort study. Lancet 397(10286): 1725-1735.
-
Angel Y, Spitzer A, Henig O, Saiag E, Sprecher E et al. (2021) Association between vaccination with BNT162b2 and Incidence of symptomatic and asymptomatic SARS- CoV-2 infections among health care workers. JAMA 325(24): 2457-2465.
-
Levine Tiefenbrun M, Yelin I, Katz R, Herzel E, Golan Z, et al. (2021) Initial report of decreased SARS-CoV-2 viral load after inoculation with the BNT162b2 vaccine. Nat Med 27(5): 790-792.
-
Voss WN, Hou YJ, Johnson NV, Kim JE, Delidakis G, et al. (2021) Prevalent, protective, and convergent IgG recognition of SARS-CoV-2 non-RBD spike epitopes. Science 372(6546): 1108-1112.
-
Greaney AJ, Loes AN, Gentles LE, Crawford KHD, Starr TN et al. (2021) Antibodies elicited by mRNA-1273 vaccination bind more broadly to the receptor binding domain than do those from SARS-CoV-2 infection. Sci Transl Med 13(600): eabi9915.
-
Jackson L, Rodel H, Hwa SH, Cele S, Ganga Y, et al. (2021) SARS-CoV-2 cell-to-cell spread occurs rapidly and is insensitive to antibody neutralization. BioRxiv Preprint.
-
Kamel W, Noerenberg M, Cerikan B, Chen H, Järvelin AI, et al. (2021) Global analysis of protein-RNA interactions in SARS-CoV-2 infected cells reveals key regulators of infection. Mol Cell 81(13): 2851-2867.
-
Castagnoli R, Votto M, Licari A, Brambilla I, Bruno R, et al.(2020) Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents: A Systematic Review. JAMA Pediatr 174(9): 882-889.
-
Plotkin SA, Levy O (2021) Considering mandatory vaccination of children for COVID-19. Pediatrics 147(6): e2021050531.
-
Krause PR, Fleming TR, Longini IM, Peto R, Briand S, et al. (2021) SARS-CoV-2 variants and vaccines. N Engl J Med 385(2): 179-186.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths