A Single-Centre, Observational Study to Evaluate Immune Re- Sponse to Covid-19 Vaccines in Immunocompromised Patients with Haematological Disorders (COVAC-IC)
To evaluate immunological response to Covid-19 vaccines in immunocompromised haematology patients we compared total Anti-SARS-CoV-2 spike antibody and T cell response in45 immunocompromised haematology patients with 30 healthy adults following 2 doses of Covid-19 vaccine for 3 -5 months at 30-day intervals. We found, non - significant difference in T celland total Anti-SARS-CoV-2 S antibody response between study and control group patients. Conclusions: Though there was a non - significant difference in T cell and total Anti-SARS-CoV-2 S anti body response between immunocompromised patients and healthy controls this did not result in any severe infection or Covid-19 related mortality in our study cohort. We did not identify any patient-specific factor (age, gender), specific haematological condition or treatment as determinant of response. Covid-19 vaccination was well tolerated without major side effects in both groups.
Introduction
Severe Acute Respiratory Syndrome coronavirus 2 (SARS- Cov-2; Covid-19) infection and disease has affected millions of persons worldwide. The World Health Organization declared it as a global pandemic in March 2020. Since the beginning of the pandemic over 22million people have been infected with Covid-19 in the United Kingdom with over 175,000 deaths (until June 2022) [1]. Patients with hematological diseases often have impaired immunity due to their blood disorder and/or as a consequence of treatment with chemotherapy or immunotherapy. Patients remain immunocompromised for several months after diagnosis and treatment.Covid-19 infection in immunocompromised patients was reported early in the pandemic to be more severe with higher mortality [2]. These individuals were a high-risk group to be prioritized for vaccination against Covid-19. Vaccines against Covid-19 were developed and introduced with great speed to control the pandemic. When introduced, these vaccines had not been tested in immunocompromised individuals. Their protective efficacy, safety and durability in immunocompromised individuals was therefore unknown. Covid-19 vaccines were the first mRNA technology based vaccines approved for widespread clinical use. Prior to this the mRNA based vaccines had only been used in animal studies or clinical trials. mRNA technology is dependent on an intact immune system of the recipient to generate an immune response. Vaccine serological response following influenza vaccination was found to be suboptimal in immunocompromised individuals. Definite conclusions could not be obtained from these studies due to considerable heterogeneity and bias. In patients with hematologic malignancies, preliminary studies reported a low seroconversion rate after the first BNT162b2 inoculum in patients, ranging from 18 to 25% [3].
Materials and Methods
We initiated this study in March 2021 to compare immunological response to Covid-19 vaccine in immunocompromised patients with haematological disorders and compared it with healthy control (COVAC- IC, Clinical Trials.gov Identifier: NCT04805216). The study was conducted in accordance to declaration of Helsinki and good clinical practice following REC approval (London Bridge Research Ethics Committee, reference 21/HRA/0304). Patients with haematological disorders and clinically assessed to be immunocompromised either due to their haematological condition or treatment constituted the study group. Healthy volunteers assessed to have normal immunity were recruited as the control group. The original study protocol required participants to have a baseline sample to assess for Total Anti-SARS-Cov-2 antibody response. Due to very rapid roll-out of Covid-19 vaccination in the UK with high priority to immunocompromised individuals, we amended the study (with ethics approval) to al-low any participant who had received at least two doses of Covid-19 vaccine. The participants were expected to give blood samples to assess serologic response at the nearest 30 day time point after their 2nd dose of vaccine. This was to allow greater participation and assess longitudinal serologic response. It did however introduced considerable heterogeneity in the study. The study design was discussed and approved by expert in statistics and operational research and approved again by the regional ethics committee.
Between 3 and a maximum of 5 venous blood samples were obtained from all participants at 30 day intervals following their 2nd dose of Covid-19 vaccination. Due to changes in public health vaccination schedule, participant entry criteria and blood sample scheduling had to be modified (with REC and sponsor approval). Study modification allowed recruitment of participants at the nearest 30 day time–point after the 2nd dose ofCovid-19 vaccination. Immune response was monitored for 3-5 months at 30 day time intervals. The blood samples were tested for Total Anti-SARS-CoV-2 to S and N-antigen (Roche Elecsys®) and for SARS-CoV-2 S1/S2 IgG antibody (DiaSorin Liaison®). Seropositivity was defined as SARS-CoV-2 spike- receptor binding domain specific total IgG antibody above the threshold of detection for the assay. T-cell response was assessed by Interferon gamma release assay (IGRA) using the Qiagen Quanti FERON SARS-Cov-2RUO® blood collection tubes and ELISA. A positive response was defined as increase in frequency of SARS-CoV-2 specific CD4/CD8 T cells after vaccination. We had initially planned to perform the T-cell analysis at 3 time points however lack of kit availability only allowed us to do this test on 1st blood sample (participant entry to the study). Statistical techniques including data summarization, graphs and hypothesis testing were performed to make valid conclusions.
Results
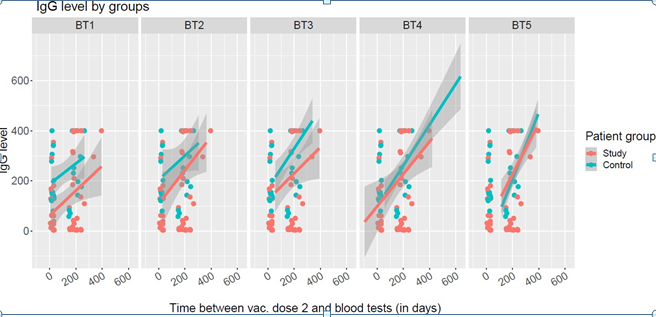
Forty-five patients (25 male, 20 female) age range 19- 78 years (median 67 years, IQR13 years) with impaired immunity due to haematological disorder or treatment and 30 immunocompetent healthy individuals (6 male, 24 female) age range 18-74 years (median 50 years, IQR 23 years) were recruited to the study between April – December 2021 (Table 1). All participants had received at least 2 doses of Covid-19 vaccine (Either ChAdOx1-S (AstraZeneca) or BNT162b2 mRNA vaccine (Pfizer)) before entry into the study. Three hundred and thirty two blood samples were collected and analyzed to evaluate immune response as per the study protocol. Comparison was made of Total Anti- SARS-CoV-2S antibody between study and control groups at specific time points after 2nd dose of Covid-19 vaccination (Figure 1). T cell response was assessed on the first blood test at entry to the study. Six (13%) study group participants did not have detectable Total Anti-SARS –Cov-2 S antibodies at any time point throughout the study monitoring period (Table 1). Three (7%) of the study group participants had no response, even after additional booster doses of Covid-19 vaccine.
| Patient cohort (study group) | Control group | |
|---|---|---|
| Age | ||
| Median | 67 | 49.5 |
| IQR | 13 | 22.5 |
| Range | 19-78 years | 18-74 years |
| Sex | ||
| Male | 25 (56%) | 6 (20%) |
| Female | 20 (44%) | 24 (80%) |
| Vaccine received | ||
| Pfizer | 14 (31%) | 14 (47%) |
| Astra Zeneca | 31 (69%) | 16 (53%) |
| Time (days) after 2nd dose vaccine to 1st | Number of patients (study group) | Number of patients (control group) |
| 15 | 7 | 7 |
| 30 | 13 | 8 |
| 150 | 4 | 3 |
| 180 | 10 | 5 |
| 210 | 4 | 4 |
| 240 | 5 | 2 |
| 270 | 1 | 1 |
| 330 | 1 | |
| Underlying haematological Diagnosis | Study Group | Control group |
| Acute Leukaemia | 3 (7%) | |
| Chronic Lymphocytic Leukaemia | 11 (24%) | |
| Hodgkin’s Lymphoma | 2 (4%) | |
| Non-Hodgkin’s Lymphoma | 5 (11%) | Healthy volunteers |
| Multiple Myeloma | 21 (46%) | |
| Chronic ITP on | 3 (7%) | |
| Immunosuppressive Therapy |
Table 1: Details of patient cohort.
All (100%) of the control group had detectable Anti- SARS-Cov-2 S antibodies after 2 doses of Covid-19 vaccine. The T cell response assessed by IGRA was reactive in 53% of study group patients compared to 77% of the control group at least 30 days after the 2nd Covid-19 vaccine. This difference was not significant (p-value = 0.098 > 0.05) (Table 3). We found non-significant difference in T cell and total Anti-SARS-CoV-2 S antibody response between study and control group patients (p-value > 0.05 other than for test 1 where p-value < 0.05) (Tables 2 & 3). Different vaccination times, doses, timing of blood test and natural infection with Covid-19 were variables which would have affected the vaccine response. Other factors include age, haematological disorder, immunosuppressive treatment (and its timing).
T cell response QuantiFERON SARS-Cov-2: Reactive (%)
Total Anti-SARS-CoV-2 S antibody: Positive (≥ 0.8U/ml)
Study Group Control Group
Blood test 1 76% 100%
Blood test 2 88% 100%
Blood test 3 83% 100%
Blood test 4 88% 100%
Blood test 5 86% 100%
- *Non-significant difference found for blood tests 2 - 5 with p-value > 0.05. Only significant difference found in test 1 with p-values = 0.009.
Table 2: Total Anti-SARS-Cov-2 S antibody positive response.
Study Group Control Group
Blood test 1 53% (n=30) 77% (n=27) (at least 30days after 2nd dose of Covid-19 vaccine) 78% (n=27)
- *Non-significant difference found with p-value = 0.098.
Table 3: T cell response assessed by IGRA assay.
When the study subgroup that had not received additional doses of Covid vaccine or had suffered from natural infection was compared with the control group the difference was still not significant (p-value > 0.05).
We tried to identify clinical characteristics which were determinants of response by comparing study subgroups with poor or good antibody response. Poor responders were defined as individuals who had anti-SARS CoV-2 S antibodies below the level of detection at all-time points. Good responders were responders with antibody levels above the upper limit of detection at all-time points. Neither a specific haematological diagnosis nor chemotherapy or immunotherapy was identified as a determinant of response (Tables 4 & 5).
Total Antibody to Spike protein (result U/ml; days after 2nd dose of covid vaccine) Age range(yr)/ Sex Clinical(diagnosis; treatment) BT1 BT2 BT3 BT4 BT5
71-75/F Stage B progressive CLL; Ibrutinib <0.4; 30d <0.4; 64d <0.4; 90d <0.4; 120d ND
71-75/F Acute Myeloid Leukaemia; Aza-Aza-citidine, venetoclax <0.4; 30d <0.4; 60d <0.4; 89d <0.4; 118d ND
71-75/F CLL, chronic ITP; low dose pred, MMF <0.4; 34d <0.4; 58d <0.4; 90d <0.4; 119d ND
76-80/ M High risk Burkitts Lymphoma; RCHOP, EPOCH-R
<0.4; 210d, 20days after 3rd dose <0.4; 330d, 140 days after 3rd dose, 20days after 4th dose <0.4; 240d, 50days after 3rd dose <0.4; 270d, 80days after 3rd dose <0.4; 300d, 110days after 3rd dose
| 66-70/ M | CLL; No treatment | <0.4; 240d, 50days after 3rd dose | <0.4; 270d, 80days after 3rd dose | <0.4; 300d, 110days after 3rd dose | <0.4; 330d, 140days after 3rd and 12 days after 4th dose | <0.4; 360d, 170days after 3rd and 42days after 4th dose |
|---|---|---|---|---|---|---|
| 61-65/ M | CLL; Acalabrutinib | <0.4;240d, 40days after 3rd dose | <0.4; 270d, 70days after 3rd dose | <0.4; 300d, 100days after 3rd, 5days after 4th dose | <0.4;330d 130days after 3rd, 35days after 4th dose | |
| *no response despite 4 doses of covid vaccination |
Table 4: Study group (immunocompromised) patients with poor antibody response to Covid-19 vaccination.
| Age range (yr)/ Sex | Clinical (diagnosis; treatment) | Total Antibody to Spike protein (result; days after second dose of covid vaccine) (Positive result ≥ 0.8 U/ml) | ||||
|---|---|---|---|---|---|---|
| BT1 | BT2 | BT3 | BT4 | BT5 | ||
| 61-65/M | Myeloma; VTD, daratutumab, lenalidomide | >250; 30 d | ND | >250; 60 d | >250; 90 days after 2nd dose | >250; 120 days after 2nd dose |
| 51-55/F | Myeloma; lenalidomide | >250; 30 days after 2nd dose | ND | >250;60 days after 2nd dose | >250; 90 days after 2nd dose | >250; 120 days after 2nd dose |
| 16-20/ M | ALPS; no treatment | >250; 30 days after 2nd dose | ND | >250;60 days after 2nd dose | >250; 90 days after 2nd dose | >250; 120 days after 2nd dose |
| 31-35/ F | Myeloma; lenalidomide | >250; 15 days after 2nd dose | >250; 30 days after 2nd dose | >250;60 days after 2nd dose | >250; 90 days after 2nd dose | >250; 120 days after 2nd dose |
| 71-75/F | Acute Myeloid Leukaemia | >250; 15 days after 2nd dose | >250; 30 days after 2nd dose | >250;60 days after 2nd dose | >250; 90 days after 2nd dose | >250; 120 days after 2nd dose |
| 71-75/ M | Myeloma, post ASCT, lenalid- omide maint | >250; 150days after 2nd dose | >250; 180days after 2nd dose | >250; 210days after 2nd and 45days after 3rd | >250; 240days after 2nd, 75days after 3rd dose | >250; 270days after 2nd, 105 days after 3rd dose |
| 56-60/ M | Stage A CLL, no Treatment | >250; 180days after 2nd dose, | >250; 210days after 2nd dose, 20days after 3rd | >250; 240days after 2nd dose, 50days after 3rd dose | >250; 270days after 2nd dose, 80days after 3rd dose | >250; 300days after 2nd, 110days after 3rd dose |
| 66-70/ M | Myeloma, Cardiac Amyloidosis; Daratutumab, velcade, dex | >250; 180days after 2nd dose, 30days after 3rd | >250, 210days after 2nd and 60days after 3rd dose | >250; 240days after 2nd, 90days after 3rd and 2 days after 4th dose | >250; 270days after 2nd, 120days after 3rd and 32 days after 4th dose | >250; 300days after 2nd, 150days after 3rd and 60days after 4th dose |
| 71-75/ M | Stage A CLL, no Treatment | >250; 180days after 2nd dose | >250; 210days after 2nd dose,45days after 3rd dose | >250; 240days after 2nd, 75days after 3rd dose | >250; 270days after 2nd, 105days after 3rd dose | >250; 300days after 2nd, 135days after 3rd and 30days after 4th dose |
| 66-70/ F | Myeloma, Cardiac Amyloidosis; Daratutumab, velcade, dex | >250; 180days after 2nd dose, 30days after 3rd | >250, 210days after 2nd and 60days after 3rd dose | >250; 240days after 2nd, 90days after 3rd and 2 days after 4th dose | >250; 270days after 2nd, 120days after 3rd and 32 days after 4th dose | >250; 300days after 2nd, 150days after 3rd and 60days after 4th dose |
| 66-70/ F | LG NHL, no treatment | >250; 210days after 2nd, 30days after 3rd dose | >250; 240days after 2nd, 60days after 3rd dose | >250; 270days after 2nd, 90days after 3rd dose | >250; 300days after 2nd, 120days after 3rd, 21days | >250; 330days after 2nd, 150days after 3rd, 51days |
| 71-75/ F | St A CLL | >250; 240days after 2nd, 60days after 3rd dose | >250; 270days after 2nd, 90days after 3rd and 2days after 4th dose | >250; 300days after 2nd, 120days after 3rd and 32days after 4th dose | >250; 330days after 2nd, 150days after 3rd and 60days after 4th dose | >250; 360days after 2nd, 180days after 3rd and 90days after 4th dose |
| 76-80/ F | IgM MGUS, no treatment | >250; 240days after 2nd, 50days after 3rd dose | >250; 270days after 2nd, 80days after 3rd dose | >250; 300days after 2nd, 110days after 3rd dose | >250; 330days after 2nd, 140days after 3rd dose | >250; 390days after 2nd, 120days after 3rd, 60days after 4th dose |
| 56-60/ M | Myeloma, Daratutumab, le- nalidomide | >250; 240days after 2nd, 25 days after 3rd dose | >250; 270days after 2nd, 55days after 3rd dose | >250; 3000days after 2nd, 85days after 3rd dose | >250; 330days after 2nd, 115 days after 3rd dose |
Table 5: Details of study group (immunocompromised) patients with good antibody response following Covid-19 vaccination.
There were no reports of grade 2 or higher adverse events following vaccination. Only local AE were reported by 12 participants with no difference between the two groups. No participant suffered from Vaccine induced thrombocytopenia and thro mbosis.It is possible the inability to identify significant differences between study and co n-trol groups was due to small sample size, clinical heterogeneity, different time points of vaccination and samples taken.No participant died or was hospitalised due to severe Covid-19 infection during the study period. This included study group participants who had no antibody response at any time point.
Discussion
SARS-CoV-2 vaccines have proven highly effective in preventing severe Covid-19 but there remains considerable concern about their efficacy in haematological immunocompromised patients [3]. This prospective study evaluated immune response and safety in immunocompromised individuals with haematological diseases who had received at least 2 doses of Covid-19 vaccination and compared it with an immunocompetent control group. When planning our study in Jan 2021, we wanted rapid confirmation of clinical efficacy and safety of these vaccines in immunocompromised haematology patients. There was uncertainty about the response to the vaccine and fear of side effects particularly after reports of vaccine induced thrombosis and thrombocytopenia [4]. We chose to measure serologic response with the assumption that this will be the best correlate for clinical efficacy. The study assessed immunological response at 30 day time intervals after the second dose of Covid-19 vaccination. Blood samples were tested for antibody response was tested up to 5 time points at 30 day intervals. All participants who were able to get at least 3 tests were included in the analysis. T cell response was checked at 1st blood test. It was intended to perform T cell response assessment at 3time points ho w-ever shortage of kit during the pandemic did not allow this to happen.
There were significant challenges during the conduct of the study. The public health vaccination schedule changed the vaccine dose interval from 21-28 days to 10-12 weeks. To allow study recruitment the trial management group (TMG) had to amend the study to allow participation of all individuals who had received at least 2 doses of vaccine at least 30days before their 1st blood test and thereafter tested samples at 30 day intervals. Public health changes to vaccination happened again introducing 3rd and 4th doses for immunocompromised individuals. This resulted in some blood samples being taken after 3rd and 4th doses. These changes introduced considerable heterogeneity in the study.
All participants received either ChAdOx1-S (AstraZeneca) or BNT162b2 mRNA vaccine (Pfizer). No participant reported any grade II or more side effects. Grade I side effects between the two groups were comparable. Several investigators have studied humoral and T cell response following one or two doses of Covid-19 vaccine in people with haematological malignancies.
Overall seropositivity rate reported in terms of anti- SARS-Cov-2 S antibody was 62-66% after 2 doses of Covid-19 vaccine. The neutralizing antibody response rate was 57- 60% though this declined with emergence of new covid-19 variants of concern. The T cell cellular response rate reported in these studies varied between 40-75% [5]. This was lower than the vaccine efficacy reported in immunocompetent individuals of 74-95% [6] Vaccine induced antibodies against the spike domain have potent SARS-Cov-2 neutralizing activity [7]. Some researchers have proposed higher cut- off values for serologic response to better correlate with neutralising antibody response. This however varied between different assays and was also affected by the emergence of new covid variants [6, 8]. Our study confirmed that 13% of immunocompromised individuals had no detect-able Anti- SARS –Cov-2 S antibody response at any time point. Three (7%) of study group participants had no response even after additional booster doses of Covid-19 vaccine.
We found a non-significant difference in T cell and total Anti-SARS-CoV-2 S anti-body response between study and control group patients. Different factors including age, underlying haematological condition, immunosuppressive treatment (and its timing), vaccine type, number of doses, timing of blood test and natural infection would have affected our results. Due to this heterogeneity, definite response determinants are difficult to identify. We compared immunocompromised subgroups with poor or good antibody response. No specific haematological diagnosis, chemotherapy or immunotherapy was identified as determinant of response.
Similar findings have been reported by several investigators. In a meta-analysis of more than 7000 patients with haematologic malignancies statistical heterogeneity was substantial in more than 70%. Studies were clinically heterogeneous because of different haematologic malignancies, lack of standardized platforms and variable follow-up periods. Patients with haematologic malignancies are reported to have a lower serologic response following 2 doses of Covid-19 vaccination [5]. This response is improved following 3rd and 4th doses of covid vaccine [9]. What is unclear however, is whether a positive total Anti-SARS- CoV-2 S antibody correlates with vaccine efficacy. None of the studies have reported clinical efficacy in terms of incidence of severe Covid-19 disease or mortality between immunocompromised individuals with and without antibody response. In our cohort no study group participant suffered from severe disease or mortality due to covid. While this could be due to small sample size or strict isolation followed by immunocompromised individuals, the possibility remains that T-cell immunity provides considerable protection from severe disease and Covid-19 mortality. With emergence of new Covid-19 variants the serologic response in terms of neutralizing antibodies declined. T-cell responders however had a better protection against Covid-19 variants of concern [10].
Covid-19 anti-spike antibodies can be considered an indicator of immune response but are not a reliable correlate of clinical protection. In the majority of studies, including our own, the outcome of interest was sero positivity, which does not equate to sero protection. There is lack of standardized thresholds and variability across different commercial assays and platforms. The neutralizing antibody response is dependent on the Covid-19 variant tested against. To date there is no reliable correlate of protection that allows definite deduction of clinical efficacy from immune response generated either in the immunosuppressed or the general population [6]. Further studies should focus on identifying the correlation between serological response, T cell response, neutralization and clinical protection from symptomatic and severe Covid-19 infection. This would enable development of standardized assays and cut-off which would correlate with clinical protection.
In conclusion our study found non-significant difference in T cell and total An-ti-SARS-CoV-2 S antibody response between immunocompromised patients with haematological diseases when compared with immunocompetent adults. Covid-19 vaccination was well tolerated without major side effects in both groups. We did not identify any patient-specific factor (age, gender), specific haematological condition or treatment as determinant of response. Different vaccination times, doses, timing of blood test and natural infection with Covid-19 added considerable heterogeneity in the study. No patient suffered from severe Covid-19 infection or died due to Covid-19 during the study.
Author Contributions
Conceptualization, design, planning and conducting, DC, KK; Trial management, LO’M, AB; Statistical design and analysis, MdA; Recruitment, LB, AR; Lead virologist KB, Lead immunologist SG, Data management and validation, MA, RB; Funding acquisition and sponsors supervision, SL, KW; Patient identification and recruitment, JP, BB, NP, SP, PD, FW, FB, NK, KP; Project administration, KL, JL. All authors have read and agreed to the published version of the manuscript Funding: This study is funded by the University Hospitals of North Midlands Research Charitable Fund.
Institutional Review Board Statement
The study was sponsored by the Research and Innovation Directorate at University Hospitals of North Midlands. The study was conducted in accordance to declaration of Helsinki and good clinical practice following REC approval (London Bridge Research Ethics Committee, reference 21/ HRA/0304).
Informed Consent Statement: Informed consent was obtained from all subjects involved in the Study Acknowledgments: The investigators are grateful to Dr Simon Lea, Dr Keira Watts, Ms Karen Sneade, Ms Zuzana Tothova and Mr Jack Tilstone for their support and assistance.
Conflicts of Interest: The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
-
coronavirus.data.gov.uk/details/deaths
-
Pagano L, Salmanton-Garcia J, Marchesi F, Busca A, Corradini P, et al. (2021) COVID-19 infection in adult patients with haematological malignancies: a European Haematology Association Survey (EPICOVIDEHA). J Hematol. Oncol 14(1): 168.
-
Monin L, Laing AG, Muñoz-Ruiz M, McKenzie DR, Del Molino Del Barrio I, et al. (2021) Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: interim analysis of a prospective observational study. Lancet Oncol 22(6): 765-778.
-
Greinacher A, Thiele T, Warkentin TE, Weisser K, Kyrle PA, et al. (2021) Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 vaccination. N Engl J Med 384(22): 2092-2101.
-
The JSK, Coussement J, Neoh ZCF, Spelman T, Lazarakis S, et al. (2022) Immunogenicity of COVID-19 vaccines in patients with hematologic malignancies: asystematic review and meta-analysis. Blood Adv 6 (7): 2014-2034.
-
Fendler A, de Vries EGE, Geurtsvan Kessel CH, Haanen JB, Wormann B, et al. (2022) COVID-19 vaccines in patients with cancer:immunogenicity, efficacy and safety. Nat Rev Clin Oncol 19(6): 385-401.
-
Robbiani DF, Gaebler C, Muecksch F, Lorenzi JCC, Wang Zijun, et al. (2020) Convergent antibody responses to SARS-CoV-2 in convalescent individuals. Nature 584(7821): 437-442.
-
Garcia-Beltran WF, Denis KJST, Hoelzemer A, Lam EC, Nitido AD, et al. (2022) mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS- CoV-2 Omicron variant Cell 185(3): 457-466.
-
Greenberger LM, Saltzman LA, Senefeld JW, Johnson PW, Degennaro LJ, et al. (2021) Antibody response to SARS-CoV-2 vaccines in patients with hematologic malignancies. Cancer Cell 39(8): 1031-1033.
-
Waldhorn I, Holland R, Goshen-Lago T, Shirman Y, Szwarcwort-Cohen M, et al. (2021) Six-month efficacy and toxicity profile of BNT162b2 vaccine in cancer patients with solid tumors. Cancer Discov 11(10): 2430- 2435.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths