Comparison of Autonomic Nervous System Activity in Subjects with Chronic Neck Pain and Healthy Controls
Objective: This study investigated if differences in autonomic nervous system activity exist in patients with chronic neck pain as compared to controls measured by using a fully automated pupillometry system. Methods: 100 chronic neck pain subjects and 50 controls participated in this quasi-experimental study design evaluating the effect of chronic pain on the autonomic nervous system using a fully automated method of pupillometry. The Chisquare test for categorical data was used to establish homogeneity of baseline characteristics. The Mann-Whitney U test determined the difference in pupil diameter between the chronic neck pain group and the healthy control group. The Spearman’s rho test was used to relate the pupil diameter to the Neck Disability Index (NDI) scores, subject’s age, and the duration of chronic neck pain. Results: This study demonstrated that the chronic neck pain group had a statistically significant smaller pupil diameter than the healthy control group (p=0.022). This study showed that there was no relationship between the NDI scores and the pupil diameter change. However, there was a weak to moderate correlation between age and pupil size (p<0.001), indicating that there is a significant negative relationship and that the pupil diameter decreases with age. There was a weak but non-significant correlation between the pupil diameter and the duration of chronic neck pain (p>0.05). Discussion: The results of this study demonstrate that subjects with chronic neck pain exhibited a smaller pupil diameter than healthy controls. This is a direct indication of an altered autonomic balance.
Introduction
Chronic pain prevalence ranges from 2 to 40% in the general population.1 Amongst the many pain disorders, the occurrence of chronic spinal pain has been reported to be as high as 54 to 80% [1, 2, 3]. Chronic pain associated with the cervical spine has been reported to occur in up to 60% of patients 5 years or longer after the initial reports of symptoms [1, 4, 5]. Chronic neck pain results in significant health care cost, the inability to work, and loss of work-related productivity [6, 7, 8]. Jette, et al. [9] found that about 25% of all patient visits in outpatient clinics are for the management of neck pain. Physical therapists have been using manipulation as an intervention in the management of patients with neck pain [10, 11, 12, 13, 14] for a long time and it is a modality with proven effectiveness [15].
Chronic pain, pain that exists beyond the normal time line of tissue healing [1], can involve both local and central mechanisms. At the local level, nociceptive stimulation may cause tissue destruction or damage resulting in activation of the peripheral nociceptors, which are present in great abundance and form a large network throughout all tissues [16, 17, 18]. Chemical mediators such as serotonin, bradykinin, and potassium are effective stimulants for nociceptors lowering their facilitation threshold [17, 18, 19, 20, 21, 22]. It appears that these substances, which can be generated in local tissues, can cause a prolonged hypersensitivity of peripheral nerves resulting in peripheral sensitization [21, 22, 23, 24].
When ongoing, or tonic, nociceptive information as a result of peripheral sensitization reaches the spinal cord, it appears that there is a change in processing of central nociceptive information [25]. A lowering of threshold for excitation of the inter-neurons in the spinal cord occurs, which will result in an increased central discharge on relatively normal effective inputs and inputs that previously did not exceed facilitation threshold [26].
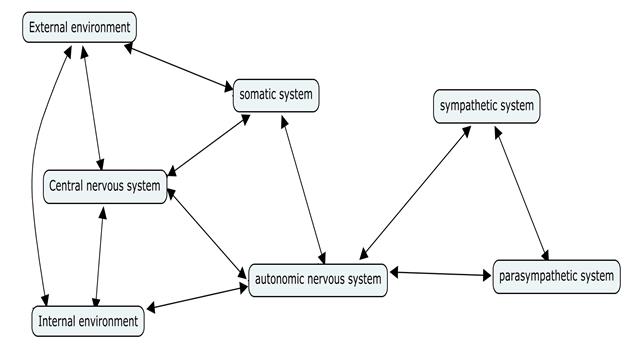
The central nervous system functions as one single unit (Figure 1), therefore, the somatic and autonomic nervous system will have direct interaction at the level of both the central and peripheral nervous system, and their functioning will be influenced by each other [27, 28, 29]. Several areas of interaction between the somatic and autonomic nervous system have been identified in the periphery, dorsal horn of the spinal cord, brainstem, and forebrain [30, 31]. In a state of either peripheral or central sensitization, hyperactivity is taking place at the level of nociceptive input in the spinal cord [32]. As a result, corresponding over-activity in the lateral gray matter and an expected increase in sympathetic activity will be present [32, 33].
periphery, which could lead to a state of orthostatic hypotension and activity intolerance [40]. Prolonged sympathetic activity can lead to ischemic changes, resulting in higher risk of tissue damage during the performance of normal activities [41].
Because the close relationship between pain and the autonomic nervous system, its parameters are often regarded as objective measures of pain in humans [42]. Several ways to assess the activity of the autonomic nervous system and its components have been identified in the literature. Traditionally, the autonomic symptoms consisting of vasomotor, sudomotor disturbances and trophic changes have been observed and measured [43, 44]. The parameters of interest have been the heart rate, local blood flow in the periphery, and the sweat response. More recently, an interest has emerged to measure the pupil diameter to obtain a direct impression of autonomic functioning [45, 46, 47, 48]. A dilation of the pupil is a result of a simultaneous increase of sympathetic activity and a decrease of parasympathetic activity [17, 43, 44, 45, 46, 47, 48, 49].
In a situation of central sensitization, the human body will be in a state of ‘attention’ and will be ready for movements and postural planning that will avoid pain [31]. Such activity can negatively impact functional abilities and treatment outcomes. To date no studies have compared autonomic nervous system activity by measuring the pupillary size between individuals with chronic neck pain and healthy controls. Hence the purpose of this study is to investigate if differences in autonomic nervous system activity exist in patients with chronic neck pain as compared to controls.
Material and Methods
Subjects
Consecutive patients with chronic cervical pain were recruited from 5 outpatient physical therapy clinics in Indiana. For the purpose of this study, cervical pain was operationally defined as the presence of non-specific pain in the cervical and cervicothoracic region down to T4, which was provoked with neck movements [50, 51]. Chronicity was operationally defined as the presence of pain that had not subjectively changed much in intensity, and had been present for at least three months [52].
An age matched healthy control group was recruited through direct advertisement in the local newspaper and by postings in the participating outpatient clinics. All available subjects were screened for the inclusion and exclusion criteria of this study. The inclusion criteria included being between the ages of 18 and 65 and able to speak and read the English language fluently. Subjects were excluded from this study if they were previously diagnosed with autonomic diseases such as the Horner’s syndrome; had a history of current neurological; ocular, and / or retinal disease; used two or more alcoholic beverages daily; or trained for endurance sports. After obtaining physician approval, the chronic cervical pain group subjects were instructed not to take any medication that could alter the functioning of the autonomic nervous system for at least 24 hours prior to participating in the study. If physician approval could not be obtained the subject was not eligible to participate in the study. All subjects were instructed not to consume caffeinated drinks, smoke, or eat anything for at least 12 hours prior to the study. If at the time of measurement, the healthy control subject were experiencing any pain or taking any medication they were also excluded from this study. This study received Institutional Review Board approval from NOVA Southeastern University. All subjects provided written consent prior to participating in the study.
Self-Reported Measures
The visual analog scale (VAS) was used to assess pain. The VAS consists of a 100-millimeter line with an anchor at each end. The left anchor indicated “ no pain” and the right anchor indicated “the worst pain imaginable” [53, 54]. The validity and reliability of the VAS has been previously reported for patients with acute and chronic pain [53, 55, 56, 57, 58, 59]. The VAS is a widely used clinical assessment tool allowing the individual to record small changes in pain intensity, and scoring of the test is simple and fast [58].
The Neck Disability Index (NDI) was used to measure each subjects level of reported disability [8, 51, 60, 61, 62] Content, construct validity, and reliability of the NDI has been previously shown in patients with neck pain [60, 63, 64].
Automated Measures
To obtain a measure of autonomic nervous system activity, the pupil diameter can be measured directly via automated pupillometry [46, 48, 49, 65, 66, 67]. The pupil responses, during this study, were measured with the fully automated Vorteq® system. The Vorteq® system for recording of the pupil reaction was developed by Micromedical Technologies, Inc (Chicago, Illinois). It includes goggles, which the subject wears during the measurement, that create a completely dark environment for both eyes. An infrared camera was attached to the goggles, allowing measurement of the pupil diameter of the right eye (Figure 2). Fully automated pupillometry devices have been used previously in a number of studies investigating autonomic nervous system activity [45, 48, 68, 69, 70, 71, 72, 73]. The measurement error has been shown to be minimal and differences smaller than 0.2 mm will be detected [71, 73, 74, 75]. It has been previously demonstrated that the intra-rater repeatability of automatic pupillometric devices is good, with coefficient of repeatability ranging from 0.6 to 1.4 mm [68, 69]. The diameter of the pupil can be considered as a direct reflection of the “live” balance between the parasympathetic and the sympathetic nervous systems [76].

The previous “gold standard” to evaluate the pupil diameter was a direct manual measure using a ruler or the Rosenbaum card [68]. The methods of automated pupillometry have a superior capacity to measure small difference (<0.5mm) in the pupil with greater accuracy than the human eye can detect with the manual method [74, 75, 77, 78, 79]. Several studies have evaluated the correlation between autonomic function tests and pupillometry and have shown that there is a significant correlation [78, 79]. Other studies have shown that pupillometry is sensitive enough to identify autonomic differences [45, 75, 80, 81].
Study Protocol
All subjects were in complete darkness during the pupillometric measurement phase of this study. The darkness was achieved by the goggles placed on the subject’s head, which allowed for a constant maximum pupil diameter during the pupil measurement without the influences of light.
During the measurement phase, all subjects were placed in the supine position with the knees slightly flexed over a bolster and the head, with the goggles in place, was placed on a pillow in a neutral position of the cervical spine. After three minutes of accommodation to the dark environment, the pupil of the right eye was measured, by the infrared camera at a frequency of 50Hz, continuously for a sixty second duration.
Statistical Analysis
Data analyses were performed using the SPSS, version 14.0, statistical software package. The Chi-square test for categorical data was used to analyze the gender distribution amongst both groups. Analysis of the skewness and kurtosis of the distribution of the pupil diameter in both groups showed a non-normal distribution, therefore, the assumption for the use of parametric statistics was not satisfied. Hence, a nonparametric analysis was necessary. The Mann- Whitney U test was used to determine the difference in baseline pupil diameter between the chronic neck pain group and the healthy control group. The Spearman’s rho test was used to relate the pupil diameter to the NDI scores, age, and the duration of chronic neck pain.
Results
Baseline Characteristics for both Groups
A total of 135 consecutive chronic neck pain subjects were assessed for eligibility. Twenty-six patients refused to participate and 8 did not have physician approval. The remaining 101 subjects were enrolled in the study. One subject with chronic neck pain was removed during the measurement phase because the subject was unable to keep their eye in a position such that the infrared camera could measure the pupil. Additionally, 50 age matched control subjects were selected. A total of 150 subjects completed the testing protocol. Demographics for the subjects with chronic neck pain and controls can be found in Table 1. No significant differences between baseline variables existed between both groups.
| Gender | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Mean duration o | f | ||||||||||
| f | emal | e | mal | e | ||||||||
| Age | symptoms | |||||||||||
| Pain Group | 77 | 23 | 44.77 | 24.3 months | ||||||||
| Control Group | 37 | 13 | 43.48 | |||||||||
| P-value | 0.685 | 0.507 |
Table 1: Baseline demographics.
Pupil Diameter
The graphic distribution of pupil diameter for both the chronic neck pain and control group can be seen in Figure
3. Given that both groups had non-normal distributions with outliers, the Mann-Whitney U test was performed [82]. The chronic neck pain group exhibited a statistically significantly smaller median pupil diameter than the control group, p=0.022 (Table 2).
![Figure 3: Given that both groups had non-normal distributions with outliers, the Mann-Whitney U test was performed [82]. The chronic neck pain group exhibited a statistically significantly smaller median pupil diameter than the control group, p=0.022 (Table 2).](/fulltextimages/6896/fig_3.png)
| Mean Pupil diameter | |||
|---|---|---|---|
| Pain Group | 146.69 | ||
| Control Group | 161.19 | ||
| P-Value | 0.022 |
Table 2: Mean pupil diameter of both groups.
Correlation between Pupil Diameter and NDI Scores, Age, and Duration of Pain
Although there was a weak correlation between the pupil diameter and the NDI score it was not statistically significant (r(148)= -0.093, p>0.005). There existed a weak to moderate correlation between age and pupil size (r(148) = -0.329, p<0.001), indicating that there is a significant negative relationship and that the pupil diameter decreases with age. There was a weak but non- significant correlation between the pupil diameter and the duration of chronic neck pain (r(98)= -0.071, p>0.05).
Discussion
The results of our study demonstrated that patients with chronic neck pain exhibited smaller pupil diameter than healthy controls. We used automated pupillometry in this study to capture the pupil diameter, which has been shown to be a valid and reliable method of assessing nervous system activity [45, 46, 67, 68, 69, 71, 74, 75, 76, 77, 83]. Therefore, it appears that chronic neck pain may impact autonomic nervous system activity, which could have therapeutic implications for physical therapists.
In a dark environment, the activity of the parasympathetic nervous system is greatly reduced and, therefore, the pupil diameter is determined by the activity of the sympathetic nervous system [67, 76]. When in a complete dark environment the subject displayed an increase in pupil diameter. This increased pupil diameter would be indicative of a relative unopposed increase in activity of the sympathetic system [17]. If there is pupil constriction, this would be indicative of a relative decrease in activity of the sympathetic system [17]. However, we cannot make causal inferences from the current study regarding the impact of chronic pain as other variables may impact pupil size and autonomic function [46, 48, 84, 85].
The overall functioning of the autonomic system will determine the overall homeostasis and the ability of the body to regain local homeostasis after tissue trauma. Pain has the simultaneous effect of activating the central sympathetic pathways and inhibiting the parasympathetic pathways [34, 35, 36, 85]. Therefore, it seems logical to assume that a group of chronic cervical pain patients would have shown an overall larger pupil diameter than a healthy pain free control group. Although there was a significant difference in pupil diameter between the chronic cervical pain group and the healthy control group, the study results show that the chronic cervical pain group had a smaller pupil diameter. Similar to the findings of Bertinotti, et al. [45] and Bakes, et al. [76] the findings of this study did not support the principle that chronic cervical pain leads to an increased pupil diameter. Additionally, this study showed that there was no correlation between the duration of chronic cervical pain and the pupil diameter. This might have been the result of a possible down regulation within to sympathetic nervous system in chronic pain patients resulting in a decreased pupil diameter in the dark when compared to the healthy controls. Additional research should further investigate if such down regulation occurs.
The normal pupil size ranges between 10 to 85 mm [35, 68, 86, 87]. There have been reports that the pupil diameter decreases with age, [46, 73, 87] which concurs with our findings that there was a weak to moderate negative correlation between age and pupil diameter in the subject population of this study.
A potential limitation of pupillometry is the fact that each pupil has a slightly different curvature; therefore, the distance between the infrared camera and the eye is not the same for each subject. Twa, et al. [74] have reported a similar concern during their assessment of pupil diameter using a digital camera. The pupil diameter between subjects with chronic neck pain and healthy controls might have been different as a result of this difference in pupil curvature amongst subjects. However, considering the sample size used in this study we would expect that this effect should have been neutralized over both groups.
There could have been a number of other variables that might have created pupillometric variations. Tyron [88] reports on the fact that fatigue, alertness, and relaxation effects the pupil diameter. Blinking temporarily reduces the pupil diameter, sometimes even to 0.0 during the measurement. To reduce the blinking effects, all pupil measurement deviations larger than one standard deviations of the mean pupil size were considered to be a blink and was eliminated from the data [65].
Conclusion
The results of this study demonstrated that patients with chronic cervical pain display a smaller pupil diameter than a healthy control group. This is a direct indication of an altered autonomic balance. This altered balance could have clinical implications for physical therapists when choosing modalities to effectively treat patients with chronic neck pain. Additionally, age is inversely related to pupil diameter. Future studies should investigate if acute pain has a different effect on the sympathetic nervous system compared to the chronic pain group used in this study. Pupillometry offers a valid and reliable assessment tool to evaluate the effect of treatment modalities on the autonomic nervous system.
References
-
Boswell M, Shah R, Everett C (2005) Interventional Techniques in the Management of Chronic Spinal Pain: Evidence-Based Practice Guidelines. Pain Physician 8(1): 1-47.
-
Abdi S, Datta S, Trescot AM (2007) Epidural Steroids in the Management of Chronic Spinal Pain: A Systematic Review. Pain Physician 10(1): 185-212.
-
Manchikanti L, Singh V, Pampati V, Damron K, Beyer C, et al. (2002) Is There Correlation of Facet Joint Pain in Lumbar and Cervical Spine? An Evaluation of Prevalence in Combined Chronic Low Back and Neck Pain. Pain Physician 5(4): 365-371.
-
Manchikanti L, Manchikanti K, Cash K, Singh V, Giordano J, et al. (2008) Age-Related Prevalence of Facet-Joint Involvement in Chronic Neck and Low Back Pain. Pain Physician 11(1): 67-75.
-
Manchikanti L, Manchikanti K, Manchukonda R (2007) Evaluation of Lumbar Facet Joint Nerve Blocks in the Management of Chronic Low Back Pain: Preliminary Report of A Randomized, Double-Blind Controlled Trial: Clinical Trial NCT00355914. Pain Physician 10(3): 425-440.
-
Gross A, Hoving J, Haines T (2004) A Cochrane Review of Manipulation and Mobilization for Mechanical Neck Disorders. Spine 29(14): 1541- 1548.
-
Gross A, Kay T, Hondras M (2002) Manual therapy for mechanical neck disorders: a systematic review. Manual Therapy 7(3): 131-149.
-
Tseng Y, Wang W, Chen W, Hou T, Chen T, et al. (2006) Predictors for immediate responders to cervical manipulation in patients with neck pain. Manual Therapy 11(4): 306-315.
-
Jette A, Simth K, Haley S, Davis K (1994) Physical Therapy Episodes of Care for Patients With Low Back Pain. Physical Therapy 74(2): 101-115.
-
Paris SS (2000) course notes Chicago.
-
Winkel D (1996) Diagnosis and Treatment of the Spine. Gaithersburg, Maryland: Aspen Publishers Inc.
-
Van der El A, Lunacies P, Wagemaker A (1993) Manuele Therapies. Rotterdam: Manuel.
-
Cantu R, Grodin A (2001) Myofascial Manipulation, Theory and Clinical application second edition. Gaithersburg, Maryland: Aspen publications Inc.
-
Kerry R, Taylor A, Mitchell J, McCarthy C, Brew J, et al. (2008) Manual Therapy and Cervical Arterial Dysfunction, Directions for the Future: A Clinical Perspective. J Man Manip Ther 16(1): 39-48.
-
Ruelle A, Datti R, Pisani R (1999) Thoracic Epidural Hematoma After Spinal Manipulation Therapy. J Spinal Disord 12(6): 534-536.
-
Coutaux A, Adam F, Willer J, Le Bars D (2005) Hyperalgesia and allodynia: peripheral mechanisms. Joint Bone Spine 72(5): 359-371.
-
Bernards J, Bouman L (1988) Fysiologie van de mens. Utrecht: Bohn, Scheltema & Holkema.
-
Cyriax J (1982) Textbook of orthopaedic Medicine, Volume one Diagnosis of Soft Tissue Lesions. 8th ed. London: Bailliere Tindall Inc.
-
Bendtsen L (2003) Central and Peripheral Sensitization in Tnesion-type Headaches. Current Pain and Headache Reports 7(6): 460-465.
-
Millan M (2002) Descending control of pain. Prog Neurobiol 66(6): 355-474.
-
Curatolo M, Arendt-Nielsen L, Petersen-Felix S (2004) Evidence, Mechanisms, and Clinical Implications of Central Hypersensitivity in Chronic Pain After Whiplash Injury. Clin J Pain 20(6): 469-476.
-
Chen X, Levine J (2005) Epinephrine-Induced Excitation and Sensitization of Rat C-Fiber Nociceptors. The Journal of Pain 6(7): 439-446.
-
Sluka K, Price M, Breese N, Stucky C, Wemmie J, et al. (2003) Chronic hyperalgesia induced by repeated acid injections in muscle is abolished by the loss of ASIC3, but not ASIC1. Pain 106(3): 229-239.
-
Kingery W, Guo T, Davies M, Limbird L, Maze M, et al. (2000) The alpha(2A) adrenoceptor and the sympathetic postganglionic neuron contribute to the development of neuropathic heat hyperalgesia in mice. Pain 85(3): 345-358.
-
Staud R, Vierck C, Cannon R, Mauderli A, Price D, et al. (2001) Abnormal sensitization and temporal summation of second pain (wind-up) in patients with fibromyalgia syndrome. Pain 91(1-2): 165-175.
-
Woolf C, Doubell T (1994) The pathophysiology of chronic pain-increased sensitivity to low threshold Abeta-fibre inputs. Curr Opin Neurobiol 4(4): 525- 534.
-
Van Cranenburgh B (1989) Inleiding in the toegepaste neurowetenschappen. Lochem: Uitgeversmaatchappij de Tijdstroom Inc.
-
Benarroch E (2006) Pain-autonomic interactions. Neurol Sci 2: S130-S133.
-
Barman S, Wurster R (1978) Interaction of descending spinal sympathetic pathways and afferent nerves. American Journal of Physiology 234(3): H223-H229.
-
Benarroch E (2001) Pain-autonomic interactions: a selective review. Clin Auton Res 11(6): 343-349.
-
Zusman M (2002) Forebrain-mediated sensitization of central pain pathways: 'non-specific' pain and a new image for MT. Man Ther 7(2): 80-88.
-
Sato A (1972) Somato-Sympathetic Reflex Discharges Evoked through Supramedullary pathways. Pflugers Arch 332(2): 117-126.
-
Sato A (1997) Neural Mechanisms of Autonomic Responses Elicted by Somatic Stimulation. Neurosci Behav Physiol 27(5): 610-621.
-
Yang L, Niemann C, Larson M (2003) Mechansim of Pupillary Reflex Dilation in awake Volunteers and in Organ Donors. Anesthesiology 99(6): 1281-1286.
-
Irene E. Loewenfeld, David A. Newsome (1971) Iris Mechanics I Influance of pupil size on dynamics of pupillary movements. American Journal of Ophthalmology 71(1): 347-362.
-
Kawasaki A (1999) Physiology, assessment, and disorders of the pupil. Curr Opin Ophthalmol 10(6): 394-400.
-
Thomas G, Segal S (2004) Neural control of muscle blood flow during exercise. J Appl Physiol 97(2): 731- 738.
-
Segal S (2005) Regulation of Blood Flow in the Microcirculation. Microcirculation 12(1): 33-45.
-
Segal S (1994) Cell-to-cell communication coordinates blood flow control. Hypertension 23(2): 1113-1120.
-
Rowell L (1997) Neural Control of Muscle Blood Flow: Importance During Dynamic Exercise. Clinical and Experimental Pharmacology and Physiology 24(2): 117-125.
-
Maguire A, Craig M, Craighead A (2007) Autonomic Nerve Testing Predicts the Development of Complications. Diabetes Care 30(1): 77-82.
-
Vicenzino B, Collins D, Wright T (1994) Sudomotor Changes Induced by Neural Mobilisation Techniques in Asymptomatic Subjects. The Journal of Manual & Manipulative Therapy 2(2): 66-74.
-
Butler D (2000) The Sensitive Nervous System. Adelaide, Australia: Noigroup Publications.
-
Menck J, Requejo S, Kulig K (2000) Thoracic Spine Dysfunction in Upper Extremity Complex Regional Pain Syndrome Type I. J Orthop Sports Phys Ther 30(7): 401-409.
-
Bertinotti L, Pietrini U, Del Rosso A (2002) The Use of Pupillometry in Joint and Connective Tissue Diseases. New York Academy of Sciences 966(1): 446-455.
-
Bitsios P, Prettyman R, Szabadi E (1996) Changes in Autonomic Function with Age: A Study of Pupillary Kinetics in Healthy Young and Old People. Age Ageing 25(6): 432-438.
-
Capao Filipe J, Falcao-Reis F, Castro-Correia J, Barros H (2003) Assessment of autonomic function in high level athletes by pupillometry. Auton Neurosci 104(1): 66-72.
-
Fotiou F, Fountoulakis K, Goulas A, Alexopoulos L, Palikaras A, et al. (2000) Automated standardized pupillometry with optical method for purposes of clinical practice and research. clinical physiology 20(5): 336-347.
-
Gibbons P, Gosling C, Holmes M (2000) Short-Term Effects of Cervical Manipulation on Edge Light Pupil Cycle Time: A Pilot Study. Journal of Manipulative and Physiological Therapeutics 23(7): 465-469.
-
Gonzalez-Iglesias J, Fernandez-De-Las-Penas C, Cleland J, Alburquerque-Sedin F, Palomeque-del- Cerro L, et al. (2008) Inclusion of Thoracic spine thrust manipulation into an electro-therapy/thermal program for the management of patients with acute mechanical neck pain: A Randomized clinical trial. Man Ther 14(3): 306-313.
-
Cleland JA, Childs JD, McRae M, Palmer JA, Stowell T, et al. (2005) Immediate effects of thoracic manipulation in patients with neck pain: a randomized clinical trial. Man Ther 10(2): 127-135.
-
Elliott A, Smith B, Penny K, Smith W, Chambers W, et al. (1999) The epidemiology of chronic pain in the community. The Lancet 354(9186): 1248-1252.
-
Ries A (2005) Minimally Clinically Important Difference for the UCSD Shortness of Breath Questionnaire, BOrg Scale, and Visual Analogue Scale. Journal of Chronic Obstructive Pulmonary Disease 2(1): 105-110.
-
Bird S, Dickson E (2001) Clinically Significant Changes in Pain Along the Visual Analoge Scale. Ann Emerg Med 38(6): 639-643.
-
Jensen M (2003) The Validity and Reliability of pain measures in Adults with Cancer. The Journal of Pain 4(1): 2-21.
-
Jensen M, Connie C, Brugger A (2002) Postsurgical pain outcome assessment. Pain 99(1-2): 101-109.
-
Jensen M, Turner J, Romano J, Fisher L (1999) Comparative reliability and validity of chronic pain intensity measures. Pain 83(2): 157-162.
-
Gallagher E, Liebman M, Bijur P (2001) Prosepctive Validation of Clinically Important Changes in Pain Severity Measured on a Visual Analoge Scale. Ann Emerg Med 38(6): 633-638.
-
Bijur P, Silver W, Gallagher E (2001) Reliabilty of the Visual Analog scale for Measurement of Acute Pain. Academy of Emergency Medicine 8(12): 1153-1157.
-
Vernon H, Mior S (1991) The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther 14(7): 409-415.
-
Childs J, Cleland J, Elliot J (2008) Neck Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health From the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther 38(9): A1-A34.
-
Riddle D, Stratford P (1998) Use of generic versus region-specific functional status measures on patients with cervial spine disorders. Phys Ther 78(9): 951- 963.
-
Hoving J, OLeary E, Niere K, Green S, Buchbinder R, et al. (2003) Validity of the neck disability index, Northwick Park neck pain questionnaire, and problem elicitation technique for measuring disability associated with whiplas-associated disorders. Pain 102(3): 273-281.
-
Cleland J, Fritz J, Whitman J, Palmer J (2006) The Reliability and Construct Validity of the Neck Disability Index and Patient Specific Functional Scale in Patients With Cervical Radiculopathy. Spine 31(5): 598-602.
-
Harle D, Wolffsohn J, Evans B (2005) The pupillary light reflex in migraine. Ophthal Physiol Opt 25(3): 240-245.
-
Dutsch M, Hilz M, Raunhut U, Solomon J, Neundorfer B, et al. (2002) Sympathetic and parasympathetic pupillary dysfunction in familial dysautonomia. Journal of Neurological Sciences 195(1): 77-83.
-
Pfeifer M, Cook D, Brodsky J (1982) Quantitative Evaluation of Sympathetic and Parasympathetic Control of Iris Function. Diabetes Care 5(5): 518-528.
-
Boxer Walcher B, Krueger R (1999) Agreement and Repeatability of Infrared Pupillometry and the Comparison Method. Ophthalmology 106(2): 319- 323.
-
Boxer Walcher B, Krueger R (2000) Agreement and repeatability of pupillometry using videokeratography and infrared devices. J Cataract Refract Surg 26(1): 35-40.
-
Levy D, Rowley D, Abraham R (1992) Portable infrared pupilloemtry using Pupilscan: relation to somatic and autonomic nerve function in diabetes mellitus. Clin Auton Res 2(5): 335-341.
-
Meeker M, Du R, Bachetti C, Larson M, Holland M, et al. (2005) Pupil Examination: Validity and Clinical Utility of an Automated Pupillometer. Journal of Neuroscience Nursing 37(1): 34-40.
-
Piha S, Halonen JP (1994) Infrared pupillometry in the assessment of autonomic function. Diabetes Res Clin Pract 26(1): 61-66.
-
Pop M, Payette Y, Santoriello E (2002) Comparison of the pupil card and pupillometer in measuring pupil size. J Cataract Refract Surg 28(2): 283-288.
-
Twa M, Bailey M, Hayes J, Bullimore M, McOptom B, et al. (2004) Estimation of pupil size by digital photography. J Cataract Refract Surg 30(2): 381-389.
-
Taylor W, Chen J, Meltzer H (2003) Quantitative pupillometry, a new technology: normative data and preliminary observations in patients with acute head injury. Technical note. J Neurosurg 98(1): 205-213.
-
Bakes A, Bradshaw M, Szabadi E (1990) Attentuation of the pupillary light reflex in anxious patients. Br. J. clin. Pharmac 30(3): 377-381.
-
Boev A, Fountas K, Karampelas I (2005) Quantitative pupillometry: normative data in healthy pediatric volunteers. Journal of Neurosurg 103(6): 496-500
-
Mylius V, Braune H, Schepelmann K (2003) Dysfunction of the pupillary light reflex following migraine headache. Clin. Auton. Res 13(1): 16-21.
-
Neil H, Smith S (1989) A simple clinical test of pupillary autonomic function, Correlation with cardiac autonomic function tests in diabetes. Neuro- ophtalmology 9(4): 237-242.
-
Giakoumaki S, Hourdaki E, Grinakis V, Theou K, Bitsios P, et al. (2005) Effects of peripheral sympatehtic blockade with dapiprazole on the fear- inhibited light reflex. Journal of Psychopharmacology 19(2): 139-148.
-
Miciele G, Tassorelli C, Martignoni E, Marcheselli S, Rossi F, et al. (1995) Further characterization of autonomic involvement in multiple system atrophy: a pupillometric study. Funct Neurol 10(6): 273-280.
-
Portney L, Watkins M (2000) Foundations of Clinical Research, Application to Practice. 2nd (Edn.), New Jersey: Prentice-Hall Inc.
-
Merritt S, Keegan A, Mercer P (1994) Artifact Management in pupillometry. Nurs Res 43(1): 56-59.
-
Ellermeier W, Westphal W (1995) Gender differences in pain ratings and pupil reactions to painful pressure stimuli. Pain 61(3): 435-439.
-
Oka S, Chapman R, Kim B, Nahajima I, Shimizu O, et al. (2007) Pupil dilation response to noxious stimulation: Effect of varying nitrous oxide concentration. Clin Neurophysiol 118(9): 2016-2024.
-
Wilson S, Amling J, Floyd S, McNair N (1988) Determining Interrater Reliability of Nurses' Assessments of Pupillary Size and Reaction. J Neurosci Nurs 20(3): 189-192.
-
Hreidarsson A (1982) Pupil Size in Insulin-dependent Diabetes: Relationship to Duration, Metabolic Control, and Long-Term Manifestations. Diabetes 31(5): 442- 448.
-
Tyron W (1975) Pupillometry: A survey of Sources of Variation. Psychophysiology 12(1): 90-93.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial