Motor and Nonmotor outcomes in a Yoga and Task Based Exercise Program: A Pilot Study
Background and Purpose: Parkinson’s disease (PD) is a progressive neurodegenerative disease characterized by motor, nonmotor, and functional deficits. Physical interventions shows promise in reducing motor deficits, however displays variable results in reducing nonmotor symptoms. It is well established that task based training improves balance and function in neurologic conditions, and yoga, a complementary exercise shows positive outcomes in mood and sleep. Instituting Yoga in conjunction with task based functional activity may provide a balanced intervention program to ameliorate key deficits. Therefore, the purpose of this pilot study is to ascertain whether Yoga coupled with task based exercise will induce positive change in function, postural alignment and control, improve quality of life, and reduce fatigue in persons with PD. Methods: Ten participants with PD (6 men and 4 women) with a mean age of 66.4 years enrolled in a two time per week, 8-week group intervention. The pilot study is a one group pre-post design. Outcome measures were the Cognitive Timed up and Go (TUG), Ten Meter Walk Test, craniovertebral angle for forward head, Fullerton Advanced Balance Scale (FAB) and Berg Balance Scale (BBS). The study examined the nonmotor domain by implementing the Parkinson’s disease Quality of Life (PDQL) and the Parkinson’s Fatigue Scale (PFS). Results: The PFS showed significant pre (median score 60) to post-intervention differences (median score 49), Z =-2.03, P=.042. The BBS revealed significant improvement from pre (median score 52) to post intervention (median score 53), Z=-2.108, P=.035. Additional findings were reductions in the mean craniovertebral angle (6 degrees), 4.3 second reduction in the Cognitive TUG and a mean gain of 9 points in the PDQL. Discussion and Conclusions: A positive outcome was the reduction in fatigue, which was present throughout the Hoehn and Yahr stages. Furthermore, advances were noted in cervical alignment, postural control (BBS) and the Cognitive TUG. Yoga coupled with task based activity shows benefit in reducing fatigue and improving postural control in individuals with PD. Future studies should combine Yoga and functional activities to ascertain additional benefits.
Introduction
Parkinson’s disease (PD) is a progressive neurodegenerative disorder that presents with the clinical signs of bradykinesia, resting tremors, stiffness and rigidity. The evolution ultimately impairs postural control, reduces gait speed, and diminishes axial alignment, all leading to an increased risk of falls. Additionally, debilitating nonmotor symptoms coincide with movement dysfunction, resulting in fatigue, diminished executive function, and depression. Together, the motor and nonmotor presentation reduces the ability to participate in everyday activities, thus impacting quality of life (QOL). Over the past decade, exercise has been strongly advocated because of its potential to increase function in PD [1]. Overall findings have been positive for several facets of motor function, however, there is emerging evidence that exercise may also enhance nonmotor symptoms [2, 3]. As such, the emergence of complementary exercise programs is a promising therapeutic avenue, presenting favorable reductions in non-motor symptoms in individuals with PD [4]. For example, Tai Chi, has been found to increase postural control, improve depression, resulting in fewer falls in persons with PD [5]. An additional program, Yoga has shown to be an effective intervention for reducing motor impairments, and has the potential for decreasing nonmotor symptoms in PD [6]. Classified as a complementary intervention for a host of chronic health conditions, Yoga incorporates a variety of physical poses with a focus on postural alignment, controlled movement, and sustained mental focus [7]. Studies have cited increases in sensory awareness and overall relaxation [8, 9]. Benefits of a therapeutic program of yoga in individuals with PD reveal functional changes such as an increase in sit to stand as well as nonmotor reductions in depression and blood pressure [10, 11]. Inherent in Yoga are postural transitions which mirror task based exercise. Task based exercises comprise of everyday activities such as stand to prone, prone to supine, sit to stand and floor to stand. By emphasizing task based exercise while performing Yoga, individuals with PD will engage in functional transitions, which will potentially impact their quality of life. Unfortunately, few rehabilitation studies in PD incorporate yoga and task based exercise, especially those assessing the nonmotor factors of fatigue and QOL. Consequently, it is clear that a study investigating motor and the nonmotor entities of fatigue and QOL needs to be put forth. Therefore, the purpose of this pilot study is to ascertain the effectiveness of an 8-week Yoga group class integrated with task based exercise to improve the nonmotor aspects of fatigue and quality of life along with postural control and postural alignment in individuals with PD. Secondary outcome measures are functional strength and gait speed.
Methods
Participants
Participants were recruited as a sample of convenience from the Greater Fresno Parkinson’s support group. Approval of the study was provided by the California State University, Fresno institutional review board and the Department of Physical Therapy. Participants reviewed the consent form, signed and were provided a copy prior to the initial assessment. Inclusion criteria for this study were: 1) ages 40 -75; 2) Hoehn and Yahr (H &Y) scale stages 1- 4; 3) community dwelling; 4) ambulatory with or without an assistive device, 5) stable medical regiment for over one month; and 5) ability to follow an activity program. The H & Y scale is the widely used categorical scale, charting motor and functional involvement in PD. The 5 stages are as follows: Stage1) unilateral involvement with minimal disability; Stage 2) bilateral involvement without impairment of balance; Stage 3) mild to moderate disability with some postural instability, but physically independent; Stage 4) severely disabled, but able to walk or stand using a device and Stage 5) bed or wheelchair bound [12]. Exclusion criteria were: 1) hospitalized within the last three months; 2) a second neurologic diagnosis; 3) drug induced psychosis; 4) poorly or uncontrolled hypertension or 5) cardiopulmonary pathology.
Procedure
The design is a single group pilot study that was held in a community based Yoga studio. Study duration lasted 8 weeks, with a frequency of 2 times per week for 50 minutes. A licensed physical therapist certified in Iyengar yoga led the group session. Pre and post assessment were provided one week prior and after intervention by four assessors who were blinded to the participants H & Y status and to the interventions. Assessor training was provided by the primary investigator on all outcome measures. Data was collected at the Department of Physical Therapy Research Laboratory on the campus of California State University, Fresno State.
Outcome Measures
The following assessments were provided in this set order for pre and post testing: 1) two questionnaires, the Parkinson’s Fatigue Scale (PFS) and the Parkinson’s disease Quality of Life Questionnaire (PDQL); 2) two balance scales, Berg Balance Scale (BBS) and Fullerton Advanced Balance Scale (FAB); 3) measurement of the head forward posture using the craniovertebral (CV) angle; 4) Cognitive timed up and go (TUG) is a timed functional task involving rising from a chair, walking 3 meters to a set mark, turning around the mark and returning seated to the chair while simultaneously engaged in a math problem; 5) 10 meter walk test (10MWT) examines an individual’s walking time to marked cone at 10 meters, measuring the mid 6 meters and; 6) motor section of the United Parkinson’s disease Rating Scale (UPDRS). The PFS is a self-reporting fatigue scale consisting of 16 items with a 5 response Likert scale 0 (strongly disagree) to 4 (strongly agree). Inter-rater reliability is set at r = .82 - .83, depicting good reliability and displaying concurrent validity with the Rhoten Fatigue Scale (ICC = .68) [13]. The PDQL is a self- administered PD quality of life (QOL) measure consisting of 37 items, rated on a 5 point scale, which shows excellent internal consistency (Cronbach’s α = .94) [14, 15]. The BBS is a 14 item balance scale with a 5 point ordinal scale with excellent inter-rater reliability in PD (ICC=.95) [16]. An additional balance scale is the FAB, which contains 10 items, including a 5 point ordinal scale and able to predict falls in PD with an accuracy of 0.68 [17]. The outcome measures demonstrates excellent internal consistency for older adults (Cronbach’s α=0.80) with excellent interrater reliability (r = 0.94 -0.97) [18]. For gait measures, the 10 MWT shows excellent test-retest reliability for individuals with PD (ICC=.96) [19]. The Cognitive TUG demonstrates excellent test-retest reliability in community dwelling older adults (r=0.98) along with high sensitivity (76.5%) and specificity (73.75) for predicting falls in PD [20]. Forward head posture was examined with Dartfish 8 software. Participants were videotaped in the sagittal plane, in a relaxed standing posture from a set distance of 5 feet. Dartfish measures the CV angles by setting a horizontal line at the 7th cervical vertebrae and a second intersecting line from the 7th cervical vertebrae to the tragus [21]. A CV angle < 50 degrees portrays a forward head posture.(Ruivo, Pezarat- Correia, & Carita, 2014) Photography measuring the CV angle demonstrates a high inter-rater reliability (ICC= .87- .99) [22].
Intervention
Each of the Yoga sessions was led by a physical therapist who held a certification as a Yoga instructor. Participants initiated each of the sessions with chair poses that emphasized cervical and thoracic alignment, then advanced to thoracic rotation activities. Sessions then moved to poses in supine, prone, quadruped and standing positions. Each of the distinct positions first required to maintain postural alignment, then advance spinal flexibility (flexion, extension and rotation). Poses accentuated overhead shoulder abduction or flexion to add postural complexity or gain flexibility. Additionally, participants engaged in task based activities performing sit to stand, chair to floor, rolling to and from prone to supine and engaging in floor to stand. Two to three assistants attended each session to support participants in obtaining poses and assisting as necessary in functional movements. Advances were proposed by the lead instructor, providing strategies to increase functional independence (less assistance from chair or physical assistance) and instilling increasingly difficult sitting and standing balance activities (reducing use of the chair, increase time maintaining poses or less physical assistance).
Data Analysis
Data was analyzed with IBM SPSS Statistics 25. The study implemented the paired t-test to analyze the 10 MWT and Cognitive TUG. The Wilcoxon Signed Ranked Test was performed on each of the questionnaires and with the following outcome measures: BBS, FAB, PDQL and the UPDRS. Forward head posture compared pre and post CV angles using the paired t-test. Significance levels were set at P <.05.
Results
The study recruited 12 participants from September to October 2015, however two participants did not complete the study, one dropped out during the intervention period because of medical reasons and another participant was unable to attend the final assessment session, leaving 10 participants. The average age of the 10 participants was 65.4 ± 5.7 years of age with 6 males and 4 females H & Y
ranged from 1 to 3, See Table 1 for full characteristics. During the duration of the study, no physical harm (falls, fatigue, injury) occurred during the sessions or assessment.
| Participant | Age Yrs. | Sex | Yrs. Dx PD | Assistive Device | Co-morbidities | History of Falls | PD Meds | On PD Meds yoga | H&Y Stage | Falls during study |
| 1 | 57 | F | 1 | C | 1,2,3,4,5 | No | Yes | Yes | 1 | 0 |
| 2 | 68 | M | 2 | C | 5 | Yes | Yes | No | 2 | 0 |
| 3 | 67 | M | 1 | 3 | No | Yes | Yes | 1 | 0 | |
| 4 | 61 | M | 17 | 5 | No | Yes | Yes | 1 | 0 | |
| 5 | 62 | M | 7 | 1,3,5 | Yes | Yes | Yes | 2 | 1 | |
| 6 | 73 | F | 16 | WW | 5 | No | Yes | Yes | 2 | 0 |
| 7 | 68 | M | 4 | C | 5 | Yes | Yes | Yes | 3 | 11 |
| 9 | 70 | F | 3 | 0 | No | Yes | No | 1 | 0 | |
| 10 | 67 | F | 1 | 0 | No | No | No | 1 | 0 | |
| 11 | 71 | M | 4 | 2 | No | Yes | Yes | 3 | 0 |
Table 1: Participant Characteristics of the 8 Week Yoga and Task Based Intervention Study.
Table 1: Participant Characteristics of the 8 Week Yoga and Task Based Intervention Study. Abbreviations: Yrs: Years; Dx: Diagnosed; PD: Parkinson’s disease; C: Cane; WW: Wheeled Walker; H & Y: Hoehn & Yahr. Co-morbidities 1: Hypertension; 2: Diabetes Mellitus; 3: Asthma; 4: Chronic Pain; 5: Orthopedic. Parkinson’s Fatigue Scale questionnaire documented a significant decrease in fatigue scores from pre- intervention (median score = 60) to post-intervention (median score = 49), Z =-2.033, P=.042. To further analyze the data, PFS scores were stratified into H & Y stages, with each stage revealing a decrease in fatigue scores. See Figure 1 for results.
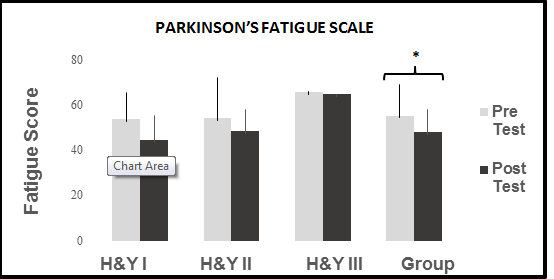
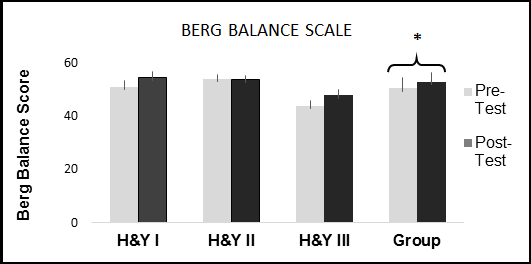
Figure 1: Parkinson’s Fatigue Scale. A comparison of pre and post-test group and H & Y stage I, II and III results.* P=.042. H & Y: Hoehn and Yah. In the postural realm, the Wilcoxon signed ranked test found a significant increase in BBS scores from pre- intervention (median score =52.0) to post-intervention (median score =53.0), Z=-2.108, P=.035. To further analyze, the data was stratified by H & Y stages, displaying an increase from pre to post-intervention in stages I and III. See Figure 2 for results. In terms of postural alignment, 8 participants (2 participants’ videos could not be analyzed) were analyzed for the CV angle. The mean pre intervention CV angle was 36 ± 15.14 (mean ± SD) degrees with post-intervention angles revealing 42 ± 9.06, (mean ± SD) degrees for a change of 6 degrees. Finally, the pre-intervention balance score for the FAB was 29.6 ± 6.09, (mean ± SD) to a post-intervention score of 32.3 ± 4.71(mean ± SD); a positive overall increase, however the results were not significant.
Although the gait outcomes did not demonstrate statistical significance, there were clinical relevant findings. For the Cognitive TUG, the pre-intervention time was 16.2 ± 8.9 (mean ± SD) seconds to a post intervention time of 11.9 ± 4.0 (mean ± SD), a difference of 4.3 seconds. In the 10 MWT, the pre intervention velocity was 0.95 m/s ± 0.41 (mean ± SD) compared to post velocity of 1.19 ± 0.18 (mean ± SD), an increase in velocity of 0.25 m/s. The PDQL pre and post intervention results did not reveal significant results, however there were positive changes in the PDQL. Pre-test scores show 126.5 ±18.4 (mean ± SD) with post-test results of 135.9 ±12.5 (mean ± SD). Eighty percent of participants stated increases in quality of life. The UPDRS motor section did not reveal meaningful changes in scores from pre 16.9 ±10.6 (mean ± SD) to post intervention 16.4 ± 8.7 (mean ± SD). Discussion This pilot study revealed that a group eight week yoga and task based intervention significantly reduces fatigue and increases postural control in individuals with PD. Additionally, there were positive gains in the gait realm, with velocity and the Cognitive TUG documenting increases in performance. Furthermore, advances were observed in the QOL questionnaire, and cervicocranial angle. Thus, a program of task based yoga holds potential for reducing the burden of fatigue while ameliorating facets of motor function. Fatigue has been identified as one of the more incapacitating symptoms in PD, leading to limitations in function and reductions in quality of life [23]. Moreover, fatigue is intrinsic to PD, emerging in the initial stages and progressing as the disease advances.(Metta et al., 2011) At the initial phase of the study, this cohort rated the fatigue questions (PFS) as a mean of 3.5, (challenging fatigue > 3.2), and post intervention, reported a score of 3.0. This finding was noteworthy, as only a few exercise studies have reported significant fatigue reductions in PD [2, 24, 25]. Yoga appears to have similar effects on fatigue reduction in other diseases, as documented in research studying persons with cancer and multiple sclerosis [26, 27]. Postural control along with alignment were the outcomes of interest. For postural control, the results of the BBS were significant, however, the pre-post mean difference score was 2.1 points, with 3.3 documented as the minimum detectable change in older adults [28]. Given that the BBS has a low ceiling and the change scores did not meet the minimum detectable change, the significant findings should be taken cautiously [17]. Scoring for the FAB may be more telling as the measure depicts a limited ceiling effect with a mean difference score was 2.6 points, however there is not an established rating for the meaningful detectable change [29]. As for the cervicocranial angle, an average increase of 6 degrees was found in the forward head posture. Although postural alignment is a major clinical presentation, there are limited studies addressing alignment. Schenkman [30] detailed similar improvement in spinal mobility implementing a three time per week/10 week program. Additionally, Colgrove [31] in an 8 week Yoga study with individuals with PD reported participants provided positive subjective comments on postural alignment. Therefore, future studies should put forth a concerted effort to include spinal flexibility exercise to confirm that flexibility activities can improve postural alignment in individuals with PD. Although the Cognitive TUG results did not reach statistical significance, the outcome reached clinically relevant cut off scores. The pre intervention Cognitive TUG time of 16.2 seconds was reduced to a post intervention time of 11.9 seconds. Vance [20] set the PD Cognitive TUG cut off score for falls at > 14.7 seconds, thus ascertaining a reduction in falls risk for this cohort. Similarly, the 10 MWT obtained a clinical meaningful change in velocity, posting a pre-post difference of 0.25 m/s, a substantial change given 0.1 - 0.2 m/s is the clinical meaningful score for both the geriatric population and in adults with movement based pathology [32, 33]. An interesting caveat in this pilot study were the advances in gait velocity and improvements in the Cognitive TUG, primarily because the study did not institute a gait intervention. Several interventional studies in PD have shown similar outcomes, particularly if the studies included motor tasks intertwined with cognitive activities (dual task) [34]. In one such study, Brauer [35] found that dual task activities improved step length in individuals with PD. Additionally; an interventional study in individuals with PD found that dual task activities resulted in increased in gait speed [36]. In this study dual tasking was instilled in the interventions, as participants’ maintained visual and auditory vigilance to produce physical poses while sustaining a high level of attention to maintain the task. Furthermore, the program imparted systematic increases, with greater postural control demands, longer duration of holding a physical pose and precise feedback to advance postural alignment. Thus, the interaction of these demands, both cognitive and motoric could have unintentionally enhanced performance in gait activities.
Limitations
There were several limitations that should be addressed. First of all, this was a pilot study with limited number of participants and a single group design, thus the results should be taken cautiously. Additionally, recruitment was performed as a sample of convenience and the stages of PD was not evenly distributed. Furthermore, one individual required more physical cueing and assistance during the intervention sessions, therefore was provided with more individualized feedback which may have biased the results.
Conclusion
The 8-week pilot study implementing an adapted yoga program with task based functional activity revealed positive changes in fatigue with favorable responses in balance. Furthermore, there were positive changes alignment and gait velocity. Future studies should incorporate yoga with other forms of interventions to affirm if a multimodal approach of exercise can reduce additional motor components and non-motor symptoms in individuals with PD.
Acknowledgement
I would like to acknowledge the Doctor of Physical Therapy students from California State University, Fresno for their assistance in this study.
Conflict of Interest
There was no personal or institutional conflict of interest for this study.
References
-
Ahlskog JE (2016) New and appropriate goals for parkinson disease physical therapy. JAMA Neurol 73(3): 269-270.
-
Cusso ME, Donald KJ, Khoo TK (2016) The Impact of Physical Activity on Non-Motor Symptoms in Parkinsons Disease: A Systematic Review. Front Med (Lausanne) 3: 35.
-
Subramanian I (2017) Complementary and Alternative Medicine and Exercise in Nonmotor Symptoms of Parkinsons Disease. Int Rev Neurobiol 134: 1163-1188.
-
Kwok JY, Choi KC, Chan HY (2016) Effects of mind- body exercises on the physiological and psychosocial well-being of individuals with Parkinsons disease: A systematic review and meta-analysis. Complement Ther Med 29: 121-131.
-
Cwiekala-Lewis KJ, Gallek M, Taylor-Piliae RE (2017) The effects of Tai Chi on physical function and well- being among persons with Parkinsons Disease: A systematic review. J Bodyw Mov Ther 21(2): 414-421.
-
Justice C, Cheung C, Samson-Burke A (2018) Development and Evaluation of a Yoga Intervention Program for Parkinson's Disease. Int J Yoga Therap 28(1): 113-122.
-
Ross A, Thomas S (2010) The health benefits of yoga and exercise: a review of comparison studies. J Altern and Complement Med 16(1): 3-12.
-
Govindaraj R, Karmani S, Varambally S, Gangadhar BN (2016) Yoga and physical exercise - a review and comparison. Int Rev Psychiatry 28(3): 242-253.
-
Wims ME, McIntyre SM, York A, Covill LG (2017) The Use of Yoga by Physical Therapists in the United States. Int J Yoga Therap 27(1): 69-79.
-
Boulgarides LK, Barakatt E, Coleman-Salgado B (2014) Measuring the effect of an eight-week adaptive yoga program on the physical and psychological status of individuals with Parkinson's disease. A pilot study. Int J Yoga Therap 24: 31-41.
-
Sharma NK, Robbins K, Wagner K, Colgrove YM (2015) A randomized controlled pilot study of the therapeutic effects of yoga in people with Parkinsons disease. Int J Yoga 8(1): 74-79.
-
Bhidayasiri R, Tarsy D (2012) Parkinsons Disease: Hoehn and Yahr Scale. Inc R Bhidayasiri D Tarsy (Eds.), Movement Disorders, pp: 4-5.
-
Brown RG, Dittner A, Findley L, Wessely SC (2005) The Parkinson fatigue scale. Parkinsonism & Relat Disord 11(1): 49-55.
-
Hobson P, Holden A, Meara J (1999) Measuring the impact of Parkinsons disease with the Parkinsons Disease Quality of Life questionnaire. Age and Ageing 28(4): 341-346.
-
de Boer AG, Wijker W, Speelman JD, de Haes JC (1996) Quality of life in patients with Parkinsons disease: development of a questionnaire. J Neurol Neurosurg Psychiatry 61(1): 70-74.
-
Leddy AL, Crowner BE, Earhart GM (2011) Functional Gait Assessment and Balance Evaluation System Test: Reliability, Validity, Sensitivity, and Specificity for Identifying Individuals with Parkinson Disease Who Fall. Phys Ther 91(1): 102-113.
-
Schlenstedt C, Brombacher S, Hartwigsen G, Weisser B, Moller B, et al. (2016) Comparison of the Fullerton Advanced Balance Scale, Mini-BESTest, and Berg Balance Scale to Predict Falls in Parkinson Disease. Phys Ther 96(4): 494-501.
-
Rose DJ, Lucchese N, Wiersma LD (2006) Development of a Multidimensional Balance Scale for Use With Functionally Independent Older Adults. Arch Phys Med Rehabil 87(11): 1478-1485.
-
SteffenT, Seney M (2008) Test-retest reliability and minimal detectable change on balance and ambulation tests, the 36-item short-form health survey, and the unified Parkinson disease rating scale in people with parkinsonism. Phys Ther 88(6): 733- 746.
-
Vance RC, Healy DG, Galvin R, French HP (2015) Dual tasking with the timed "up & go" test improves detection of risk of falls in people with Parkinson disease. Phys Ther 95(1): 95-102.
-
Singla D, Veqar Z, Hussain ME (2017) Photogrammetric Assessment of Upper Body Posture Using Postural Angles: A Literature Review. J Chiroprac Med 16(2): 131-138.
-
Ruivo RM, Pezarat-Correia P, Carita AL (2014) Cervical and shoulder postural assessment of adolescents between 15 and 17 years old and association with upper quadrant pain. Braz J Phys Ther 8(4): 364-271.
-
Metta V, Logishetty K, Martinez-Martin P, Gage HM, Schartau PES, et al. (2011) The Possible Clinical Predictors of Fatigue in Parkinsons disease: A Study of 135 Patients as Part of International Nonmotor Scale Validation Project. Parkinsons Dis 2011: 125271.
-
Cugusi L, Solla P, Serpe R, Carzedda T, Piras L, et al. (2015) Effects of a Nordic Walking program on motor and non-motor symptoms, functional performance and body composition in patients with Parkinsons disease. Neuro Rehabilitation 37(2): 245-254.
-
Franssen M, Winward C, Collett J, Wade D, Dawes H (2014) Interventions for fatigue in Parkinsons disease: A systematic review and meta-analysis. Mov Disord 29(13): 1675-1678.
-
Kahraman T, Ozdogar AT, Yigit P, Hosgel I, Mehdiyev Z, et al. (2018) Feasibility of a 6-Month Yoga Program to Improve the Physical and Psychosocial Status of Persons with Multiple Sclerosis and their Family Members. Explore (NY) 14(1): 36-43.
-
Sprod LK, Fernandez ID, Janelsins MC, Peppone LJ, Atkins JN, et al. (2015) Effects of Yoga on Cancer- Related Fatigue and Global Side-Effect Burden in Older Cancer Survivors. J Geriatric Oncol 6(1): 8-14.
-
Donoghue D, Stokes EK (2009) How much change is true change? The minimum detectable change in elderly people. J Rehabil Med 41(5): 343-346.
-
Hernandez D, Rose DJ (2008) Predicting which older adults will or will not fall using the Fullerton Advanced Balance scale. Arch Phys Med Rehabil 89(12): 2309-2315.
-
Schenkman M, Cutson TM, Kuchibhatla M, Chandler J, Pieper CF, et al. (1998) Exercise to improve spinal flexibility and function for people with Parkinsons disease: a randomized, controlled trial. J Am Geriatr Soc 46(10): 1207-1216.
-
Colgrove YS, Sharma NK, Kluding P, Potter D, Imming K, et al. (2012) Effect of Yoga on Motor Function in People with Parkinsons Disease: A Randomized Controlled Pilot Study. J Yoga Phys Ther 2(2): 1-12.
-
Bohannon RW, Glenney SS (2014) Minimal clinically important difference for change in comfortable gait speed of adults with pathology: a systematic review. J Eval Clin Pract 20(4): 295-300.
-
Perera S, Mody SH, Woodman RC, Studenski SA (2006) Meaningful change and responsiveness in common physical performance measures in older adults. J Am Geriatr Soc 54(5): 743-749.
-
Nocera JR, Hackney ME (2015) The Cognition- Exercise Interaction in Parkinsons Disease: A Perspective on Current Rehabilitation Approaches with Promise to Impact the Whole Disease Sequelae. J Gerontol Geriatr Med 1(1): 1-4.
-
Brauer SG, Morris ME (2009) Can people with Parkinson's disease improve dual tasking when walking? Gait Posture 31(2): 229-233.
-
Yogev-Seligmann G, Giladi N, Brozgol M, Hausdorff JM (2012) A training program to improve gait while dual tasking in patients with Parkinsons disease: a pilot study. Arch Phys Med Rehabil 93(1): 176-181.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial