Coach’s Eye a Tool to Evaluate Kinematic Variation during Weight Acceptance Phase among Community Stair Climbing Population
Subtle signs of musculoskeletal diseases are likely to be discovered earlier in task involving walking up the stairs. Stair walking monitoring in daily living environments is what is needed to screen people for clinical treatment. Tools are being developed for modeling digital humans within virtual environments to facilitate designing products, evaluating capabilities, predicting injuries in real-world scenarios. Coach’s eye is one of the most effective tool to provide meaningful feedback to the patients, so they can make rapid improvements and also helps quickly improve overall patient performance by providing instant video feedback. Purpose: (i) To measure kinematic knee ROM using coach’s eye feedback tool, (ii) To identify the normal tread depth and riser height in relation to normal kinematics. Methodology: A group of 30 subjects including male and female having knee pain with the mean age 41.75 (±5.784) were analyzed. The groups underwent kinematic analysis while climbing up the stairs by step over step pattern in their own storey buildings. Videos were obtained in the sagittal plane by the video recorder utilizing the coach’s eye feedback tool. The level of pain was measured using visual analogue scale. Reflective markers were attached on right & left upper iliac crest, lateral femoral condyle & lateral malleolus for effortless measurement of knee joint angle.
Introduction
Stair climbing is a common activity of daily living, the ability to do it efficiently is important to an individual’s Coach’s Eye a Tool to Evaluate Kinematic Variation during Weight Acceptance Phase among Community Stair Climbing Population quality of life. Any difficulty during stair climbing is attributable to increase in muscular demands, which are reflected in larger forces, angles, powers, moments and ranges of motion (ROM) and Ann Physiother Occup Ther
Which occur consistently at the knee joint [1]. Without the use of video capture, it is likely that assessments using visual evaluation techniques are less than optimal and may lead to incorrect assessment or misdiagnosis. Video capture can improve the ability to slow human movement, as well as allowing for frame-by- frame analysis, which may permit more effective interventions [2, 3].
In order to precisely observe human motion, laboratory-based gait analysis systems require video capture: (1) at an adequate frame rate and (2) from multiple cameras (minimum of 2). Motion analysis systems use sophisticated software and hardware to capture 2D video and convert the images from each camera into a 3D reconstruction of body segments. Although 3D motion analysis systems possess superior accuracy, use of these systems can be time consuming and expensive, often with elaborate technical requirements depending on the needs of the lab. Thus, clinicians in ambulatory environments may not have access to such technology [4, 5].
However, Coach’s eye feedback tool can be used by individual physical therapists as a breakthrough assistive tool in outpatient orthopedic settings. Other features of applications include zoom, slow motion, frame-by-frame, and side-by-side comparison [6, 7]. In addition, it includes the ability to draw lines and angles and even make calculations automatically based on those drawings.
Therefore, we need to be able to discern whether differences from ‘‘normal’’ stepping are attributable to changes in the ambulation pattern during stair ascent.

Materials and Methods
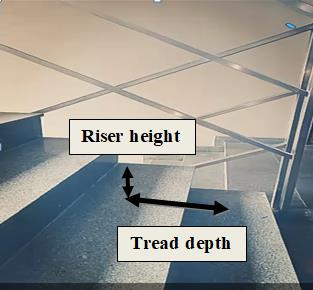
30 participants (mean age: 41.75±5.784 years) signed an informed consent form approved by the institutional review board. Presence of any known disorders such as hormonal imbalance, Musculoskeletal disorders, Neurological impairment and Cardio-vascular abnormalities are excluded. Before starting the procedure Riser Height & Tread Depth were measured with the help of measuring tape. Functional scale was asked to fill by each individual participating in the study.
The reflective markers are attached on the lower extremities therefore the subjects were reminded to wear tight pants. It was attached on the skin using double colorful tape in which it can be patched & removed easily.

Subjects were asked to perform stair climb test by step over step pattern. Coach’s Eye feedback tool for recording in the sagittal plane as subject starts climbing up the
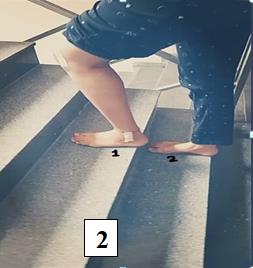
Figure 4: Knee joint position during stair climbing (Step over step pattern). Tester: If safety is concerned the tester should guard behind\below the participants going up the stairs. If there is no concern for safety, then the tester should remain on the start\finish position on the ground landing. The difference was considered statistically significant at a p value of <0.05.
Table 1 indicates mean & SD will be used to assess the outcome measures Range of motion, tread depth, riser height and VAS score in multi-storey dwellers with knee pain.
Result
All the data were expressed as a mean ± standard stairs. Knee range of motion values were obtained of each individual.

deviation (SD). A student’s version Statistical package for Social Science (SPSS) version 20.0 software for Windows was used for the statistical analysis. The level of significance was set at p<0.05 for all statistical tests.
| DOMAIN | SUM (S) | MEAN (c) | SD (s) | SE (SE ) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | 1247 | 41.566 | ±5.462 | 0.997 | ||||||||||
| YEARS OF RESIDING | 270.8 | 9.026 | ±3.198 | 0.583 | ||||||||||
| RISER HEIGHT | 550 | 18.333 | ±1.530 | 0.279 | ||||||||||
| TREAD DEPTH | 725.7 | 24.19 | ±0.748 | 0.136 | ||||||||||
| KNEE ROM | 3137 | 104.566 | ±4.825 | 0.881 | ||||||||||
| VAS SCORE | 116 | 3.866 | ±1.279 | 0.233 |
Table 1: mean and standard deviation for the baseline characteristics in affected knee joint during stair ascent.
(ROM- range of motion, VAS- visual Analogue Scale, SD- standard deviation, SE- standard error of mean).
Table 2 indicates Correlation (r) and r2 values to assess the relationship between changes in ROM over the changes in VAS Riser Height & Tread Depth. During stair ascent, the range of motion varied considerably in relation to different riser height and tread depth dimension.
Following are illustrations of knee range of motion showed in figures: 5 and 6 with distinct stair dimension.


| Pearson’s correlation-coefficient | ∑(X - M )2 x | ∑(Y -M )2 y | ∑(X - M ) (Y - M ) x y | R | r2 | ||||||||||||
| ROM over Riser Height | 67.927 | 675.367 | 188.83 | 0.8816 | 0.77 | ||||||||||||
| ROM over Tread Depth | 16.247 | 675.367 | 9.77 | 0.0933 | 0.008 |
Table 2: Correlation (r) and r2 values analysis for the relationship between changes in ROM over changes in VAS, Riser Height & T
Figure 7- Correlation of Range of Motion over Riser- Height indicates the value of Pearson’s correlation coefficient (r= 0.8816). This is a strong positive correlation. The value of R2, the coefficient of determination, is 0.7772.
Figure 8- Correlation of Range of Motion over Tread- Depth indicates the value of Pearson’s correlation coefficient (r= 0. 0.0933). Although technically a positive correlation, the relationship between the variables is weak. The value of R2, the coefficient of determination, is 0.0087.
Discussion
Study was aimed to investigate the change in the kinematic angle of knee joint during weight acceptance phase. Much higher loads on knee joint occurs during stair climbing, does so a better understanding of biomechanics is important [8, 9, 10]. Previous studies have revealed the impact of loading during weight acceptance phase at knee joint can lead to increase ground reaction forces in anterior to posterior, posterior to anterior and middle to anterior [11]. However, the limitations of the human eye to observe movement above a certain velocity raises a valid concern as to whether clinicians can accurately detect and diagnose conditions using purely visual assessment. With the availability of video technology, it seems a logical evolution to incorporate this technology into daily practice when indicated, much like any other diagnostic technology found in healthcare [12].
Angular analysis undertaken has suggested that stair dimension is one of the important factor has been mirrored in this study. In addition, less experienced clinicians are less accurate using solely visual assessment of gait and therefore video augmentation is recommend. The use of video in this case also appeared to further enhance the physical therapist interventions. Augmented feedback from video replay in order to improve human performance [9, 13].
Interestingly, early work found video feedback actually decreased performance because it overwhelmed the learner with too much information. Further investigations found video is beneficial if it is accompanied by verbal cuing from the instructor, more specifically, the use of prescriptive feedback. That is, feedback that focuses the learner’s attention on important aspects of the movement as opposed to descriptive feedback, which is feedback that focuses purely on the outcome of the movement or simply replaying with video without verbal cuing [14, 15]. In addition, it allowed for rapid feedback to alter the orthosis and added additional verbal and visual cuing for the patient.
Conclusion
Technology has advanced to allow in-clinic assessment by incorporating the use of readily available video capture using smart-phones. Furthermore, the naked eye has limitations for assessing human motion, including observation of walking. This technology and its applications can improve diagnosis and treatment with minimal addition of cost or time.
Future Recommendations
Future studies should address whether video capture for gait analysis using smart-phone technology improves a clinician’s ability to diagnose and treat orthopedic conditions.
References
-
Verghese J, Wang C, Xue X, Holtzer R (2008) Self- reported difficulty in climbing up or down stairs in nondisabled elderly. Arch Phys Med Rehabil 89(1): 100-104.
-
Standifird TW (2015) Lower Extremity Biomechanics during Stair Ascent in Healthy and Total Knee Replacement Older Adults. pp: 1-231.
-
Verbeek J, Mischke C, Robinson R, Ijaz S, Kuijer P, et al. ( 2017) Occupational exposure to knee loading and the risk of osteoarthritis of the knee: a systematic review and a dose-response meta-analysis. Saf Health Work 8(2): 130-142.
-
Reid SM, Lynn SK, Musselman RP, Costigan PA (2007) Knee biomechanics of alternate stair ambulation patterns. Med Sci Sports Exerc 39(11): 2005-2011.
-
Reid SM, Novak AC, Brouwer B, Costigan PA (2011) Relationship between stair ambulation with and without a handrail and centre of pressure velocities during stair ascent and descent. Gait Posture 34(4): 529-532.
-
Kaufman KR, Hughes C, Morrey BF, Morrey M, An KN, et al. (2001) Gait characteristics of patients with knee osteoarthritis. J Biomech 34(7): 907-915.
-
Lamont EV, Zehr EP (2006) Task-specific modulation of cutaneous reflexes expressed at functionally relevant gait cycle phases during level and incline walking and stair climbing. Exp Brain Res 173(1): 185-192.
-
Nadeau S, McFadyen BJ, Malouin F (2003) Frontal and sagittal plane analyses of the stair climbing task in healthy adults aged over 40 years: what are the challenges compared to level walking?. Clin Biomech Bristol, Avon 18(10): 950-959.
-
Zachazewski JE, Riley PO, Krebs DE (1993) Biomechanical analysis of body mass transfer during stair ascent and descent of healthy subjects. J Rehabil Res Dev 30(4): 412-422.
-
Coley B, Najafi B, Paraschiv-Ionescu A, Aminian K (2005) Stair climbing detection during daily physical activity using a miniature gyroscope. Gait Posture 22(4): 287-294.
-
Yu B (2003) Effect of external marker sets on between-day reproducibility of knee kinematics and kinetics in stair climbing and level walking. Res Sports Med 11(4): 209-218.
-
Guo M, Axe MJ, Manal K (2007) The influence of foot progression angle on the knee adduction moment during walking and stair climbing in pain free individuals with knee osteoarthritis. Gait Posture 26(3): 436-441.
-
Ajit NE, Nandish B, Fernandes RJ, Roga G, Kasthuri A, et al. (2014) Prevalence of knee osteoarthritis in rural areas of Bangalore urban district. IJRCI 1(1): 1-8.
-
Verbeek J, Mischke C, Robinson R, Ijaz S, Kuijer P, et al. (2017) Occupational exposure to knee loading and the risk of osteoarthritis of the knee: a systematic review and a dose-response meta-analysis. Saf Health Work 8(2): 130-142.
-
Ajit NE, Nandish B, Fernandes RJ, Roga G, Kasthuri A, et al. (2014) Prevalence of knee osteoarthritis in rural areas of Bangalore urban district. IJRCI 1(1) 1-8.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial