To Compare the Effectiveness of Active Stretching and Eccentric Training on Hamstrings Spasticity in Spastic Cerebral Palsy Children
Objective: To compare the effectiveness of Active-Stretching and Eccentric Training on Hamstrings spasticity in spastic cerebral palsy children. Design: Experimental Study Participants: 30 patients with cerebral palsy in the age group of 4-18 years (Modified Ashworth Scale till Grade 2) participated in this study. Intervention: All the patients were randomly selected from the OPD of Physiotherapy clinic after signing of consent form they were given 1 week rehabilitation protocol of Active Stretching(Group A) and Eccentric Strengthening(Group B). Modified Tardieu Scale, Popliteal Angle and GMFM Score were used to assess the spasticity. Main outcome measures: Modified Tardieu Scale, Popliteal Angle and GMFM Score. Result: On Day 1 and Day 7 Modified Tardieu Scale (MTS) was administered for Hamstrings, GMFM score -D (STANDING) was taken and Popliteal Angle was measured. To compare the values of MTS, GMFM and Popliteal angle at the end of 1 week in each group, repeated measure ANOVA was used. Further multivariate test was used to see the measure of strength of association and level of significance in each group. Conclusion: This study concludes that Eccentric Training has better improvement of Modified Tardieu Scale (MTS), GMFM Score and Popliteal Angle, over Active Stretching in reducing the Hamstrings muscle spasticity over a 1 week training program. Hence this study accepts the hypothesis that “Eccentric training is more effective than Active Stretching on Hamstrings spasticity in spastic cerebral palsy.
Zareen Shaikh S*, Palekar TJ and Basu S
D Y Patil College of Physiotherapy, 63/3, Shatataraka, Akash Ganga Complex,
Rabodi, Thane (W)-400601, Maharashtra, India, Tel: 8087048635; Email:
summaiyazareen.shaikh@dypatil.edu cerebral palsy children.
Design: Experimental Study
participated in this study.
Modified Tardieu Scale, Popliteal Angle and GMFM Score were used to assess the spasticity.
Main outcome measures: Modified Tardieu Scale, Popliteal Angle and GMFM Score.
strength of association and level of significance in each group.
on Hamstrings spasticity in spastic cerebral palsy.
To Compare the Effectiveness of Active Stretching and Eccentric Training on Hamstrings Spasticity in Spastic Cerebral Palsy Children Ann Physiother Occup Ther
Abbreviations: CPs: Cerebral Palsies; ROM: Range of Motion; TSR: Tonic Stretch Reflex; CP: Cerebral Palsy; AS: Ashworth Scale; HS: Held Scale; MTS: Modified Tardieu Scale; TS: Tardieu Scale; GMFM: Gross Motor Function Measure.
Introduction
The “Cerebral palsies” (CPs) have been described as “a group of non-progressive, but often changing, motor impairment syndromes secondary to lesions or anomalies of the brain arising in the early stages of development”[1].
Although the diagnosis of CP suggests an entity, it is a heterogeneous condition in terms of the type of movement disorder and the severity of impaired muscle functions [2]. CP can be classified according to the type of movement disorder into three groups: spastic paresis, dyskinesia paresis and ataxic paresis, but mixed movement disorders are also common.
One of the most prominent activity limitations concerns mobility, described as movement by changing body position or location, or by transferring from one place to another [3].
The most widely accepted definition of spasticity was formulated by Lance in 1980. In this definition, he defined spasticity as the clinical symptom of a velocity-dependent increase in muscle tone at passive stretch. Elaborating on this definition to include a clinical assessment of spasticity implies grading the intensity of the muscle tone and comparing it at different passive velocity stretches. Although ignored in Lance's definition, the patient’s testing posture and the initial length from which the muscle is stretched are both of significant influence on spasticity. Spasticity is clinically characterised by a velocity-dependent increase in muscle tone, demonstrated at a certain angle in the range of motion (ROM) in response to passive muscle stretch. In order to demonstrate the velocity-dependency, the instrument should assess spasticity by applying both a slow and a fast stretch Unfortunately, most scales are of limited value as a measure of spasticity because they only use one, usually undefined, velocity of stretch. This makes them unsuitable to discriminate between spasticity and other symptoms of abnormal involuntary muscle over activity which also lead to increased muscle tone, but which are typically non-velocity-dependent, such as hypertonia due to tonic stretch reflex (TSR) activity, or even hypertonia due to a change in biomechanical properties. When the angular velocity of the stretch increases, the intensity becomes stronger and appears sooner in the ROM [3]. This is studied by stretching the muscle with two different velocities, e.g. slow and fast [4]. It is especially important to test spasticity with a fast passive stretch. This makes it possible to detect the dominant phenomenon of spasticity: the 'catch', a sudden appearance of increased resistance in response to a fast passive stretch at a certain angle before the end ROM, which stops the movement immediately [5].
Spasticity is routinely assessed in children with cerebral palsy (CP) by means of clinical scales, of which the Ashworth Scale (AS) and the Modified Ashworth Scale (MAS) are most frequently used. However, these scales rate spasticity using an undefined velocity of stretch [5]. Moreover, both have been criticised to be invalid measures op spasticity [6]. The only clinical scales that measure spasticity with a fast angular velocity are the less frequently used Held Scale (HS) (better known as the Tardieu Scale [TS]) and the Modified Tardieu Scale (MTS)this scale should be well standardised, unambiguous and not time-consuming. It has been shown that even mildly affected children with cerebral palsy have significantly reduced isometric strength in all major lower extremity muscle groups compared to normally developing children7.Eccentric activity is another critical aspect of muscle control and function that has yet to be adequately investigated in cerebral palsy [7, 8].
Although the mechanisms underlying eccentric force generation are not completely understood, it is thought that when the muscle is undergoing an eccentric activation, the stretching and eventual breaking of the actin-myosin complex generates force which is greater than that produced during the bond forming process of concentric contractions [9]. Eccentric activation also differs from concentric activation in that the magnitude of the force that can be produced eccentrically is not as sensitive to velocity changes as that which can be produced concentrically [10].
Methods
Participants
A total of 30 subjects who fulfilled the inclusion criteria, were participated in this study. Subjects were recruited from Dr. DY Patil Orthopedic department, Physiotherapy OPD & Bharthi. All subjects met the following inclusion criteria
- Cerebral palsy children with spasticity in hamstrings muscle.
- Age-4 to 18 years of both genders.
- Hamstrings spasticity less than or equal to Grade 2 (Modified Ashworth Scale).
- 4) MMSE SCORE -21 and above. Subjects were excluded with following exclusion criteria:
- Dystonic or hypotonic or athetoid cerebral palsy children.
- Acute swelling in the region of hamstrings muscle.
- Recently operated case of hamstring lengthening.
- Children with seizure disorder.
All subjects were required to sign and written informed consent document approved by the ethical committee at Dr DY Patil Vidyapeeth, Padmashree Dr. DY Patil College of Physiotherapy, Pimpri, Pune.
Study Design
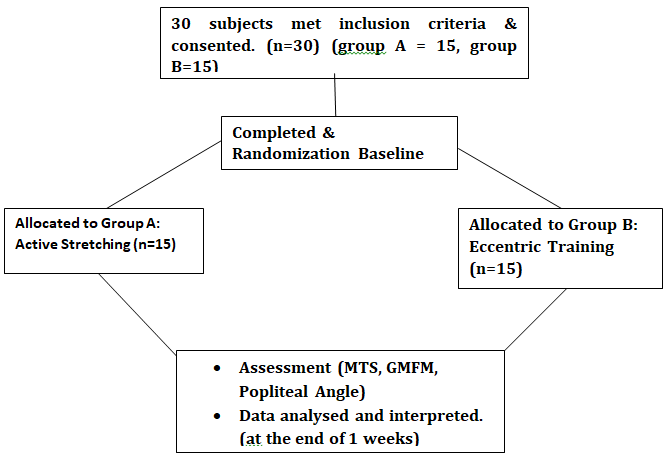
This study was an experimental study, taking place during a week period. 30 subjects were randomly allocated to two groups by the investigator who was involved in data collection, treatment implication, and data analysis. 45 cerebral palsy subjects were targeted of which 30 were included. Subjects in group A received Active Stretching. While, subject in group B received Eccentric Training. Both the groups received this protocol for a period of one week. Baseline assessments were done after randomization, at the start of the protocol. For each subject, Figure.1 all assessment sessions was performed at the same time of day.
Assessment
MTS (Modified Tardieu Scale), GMFM (Gross Motor Function Measure), Popliteal Angle assessed at baseline & at the end of 1 week.
Rehabilitation Program
The rehabilitation program consisted of 7 sessions, each for 30 second hold with a 10 second rest period for 5 times for a 1 week. All treatment sessions occurred at the same time of day on the same 7 days of the week throughout the study. Intervention was conducted individually and not in a group format. Active Stretching was given to group A patients.
Eccentric Training given to group B patients. There is evidence in the literature to support each of the components contained in the intervention.
Outcome Measures
Modified Tardieu Scale The Modified Tardieu Scale Measures Spasticity Using 2 parameters: The spasticity angle X and the spasticity grade Y. The spasticity angle X is the difference between the angles of arrest at slow speed and of catch-and- release or clonus at fast speed, whereas the spasticity grade Y is an ordinal variable that grades the intensity and thus measures the gain of the muscle reaction to fast stretch9. GMFM: Gross Motor Function Measure-ER (Expanded and Revised)-SECTION “D” The scale was administered with the child in standing and was asked to do 13 items presented on the scale and was graded accordingly. The scoring ranked from minimum 0 to a maximum of 3 points. Popliteal angle: This angle was measured at the knee joint with the hip flexed to 90 degrees and the knee range of motion was measured at the knee using a goniometer.
Statistical Analysis
Data was analysed using the SPSS Professional Statistics version 18.0 Software for Windows. Repeated measures ANOVA was used to compare the improvement in the two groups over 1 week protocol for each group in the three Outcome Measures i.e.
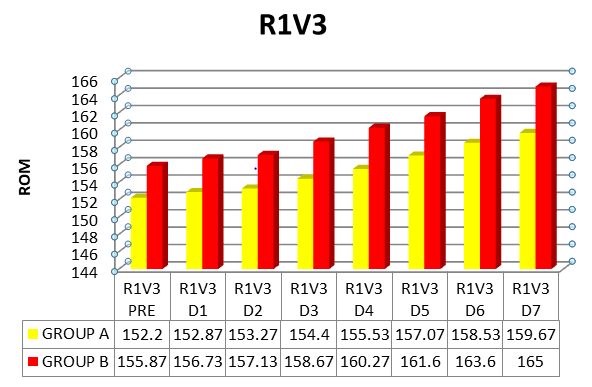
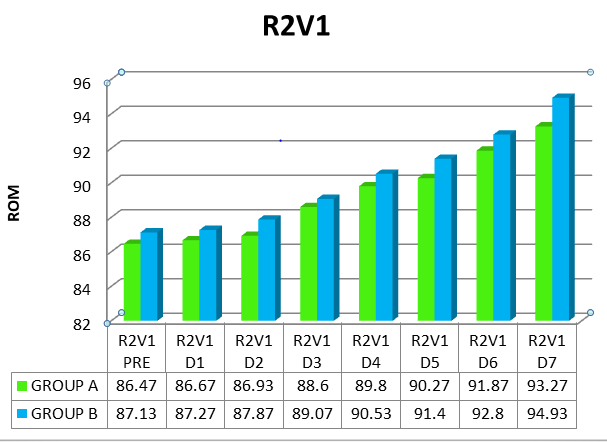
- Modified Tardieu Scale-R1V3 , R2V1
- GMFM Score.
- Popliteal Angle.
Repeated Measure Analysis (General Linear Model) was done using Multivariate Test. The Multivariate Test b was chosen and the significance value and Partial Eta Squared of the TIME bound variable and TIME * GROUP interaction was compared for the two variables R1V3 and R2V1. Pairwise Comparison Measure was also observed between the two groups and the mean difference, significance and 95% Confidence Interval for Difference. A profile plot was plotted for R1V3 and R2V1.
Results
In this study, 30 spastic cerebral palsy children were taken based on the inclusion and exclusion criteria. In Group A-15 patients were given Active Stretching to Hamstrings and 15 patients were given Eccentric Training for 7 days. On Day 1 and Day 7 Modified Tardieu Scale (MTS) was administered for Hamstrings, GMFM score-D (STANDING) was taken and Popliteal Angle was measured. To compare the values of MTS, GMFM and Popliteal angle at the end of 1 week in each group, repeated measure ANOVA was used. Further multivariate test was used to see the measure of strength of association and level of significance in each group (Table 1 and Figures 2-5).
| Mean ROM, Degrees | |||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean Diff | Significance | % Pea | |||||||||||||||||||||||||||||||||||||||
| Outcomes | Group | P | R | E | D1 | D2 | D3 | D4 | D5 | D6 | D7 | ||||||||||||||||||||||||||||||
| MTS | Time | Time*Group | |||||||||||||||||||||||||||||||||||||||
| A | 1 | 5 | 2 | 1 | 5 | 3 | 1 | 5 | 3 | 1 | 5 | 4 | 1 | 5 | 6 | 1 | 5 | 7 | 1 | 5 | 9 | 1 | 59. | 7 | 83 | ||||||||||||||||
| R1 | -4.417 | 0.001* | |||||||||||||||||||||||||||||||||||||||
| B | 1 | 5 | 6 | 1 | 5 | 7 | 1 | 5 | 7 | 1 | 5 | 9 | 1 | 6 | 0 | 1 | 6 | 2 | 1 | 6 | 4 | 165 | 0.926 | 9 | |||||||||||||||||
| A | 8 | 6. | 5 | 8 | 6. | 7 | 8 | 6. | 9 | 8 | 8. | 6 | 8 | 9. | 8 | 9 | 0. | 3 | 9 | 1. | 9 | 9 | 3.2 | 7 | 94 | ||||||||||||||||
| R2 | -0.892 | 0.001* | |||||||||||||||||||||||||||||||||||||||
| B | 8 | 7. | 1 | 8 | 7. | 3 | 8 | 7. | 9 | 8 | 9. | 1 | 9 | 0. | 5 | 9 | 1. | 4 | 9 | 2. | 8 | 9 | 4.9 | 3 | 0.725 | 16 | |||||||||||||||
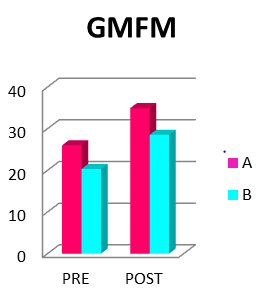
| GMFM | A | 26 | 3 | 4.9 | 3 | 86 | |||||||||||||||||||||||||||||||||||
| 6.034 | 0.001* | ||||||||||||||||||||||||||||||||||||||||
| (Score) | B | 2 | 0. | 3 | 2 | 8.5 | 3 | 0.57 | 1 | ||||||||||||||||||||||||||||||||
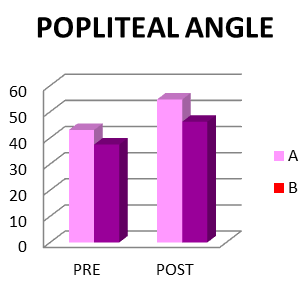
| A | 4 | 3. | 1 | 5 | 4.7 | 3 | 88 | ||||||||||||||||||||||||||||||||||
| Popliteal Angle | 7.067 | 0.001* | |||||||||||||||||||||||||||||||||||||||
| B | 3 | 7. | 5 | 46.2 | 0.047 | 13 | |||||||||||||||||||||||||||||||||||
Table 1: Data under each exercise condition for two groups were subjected to Repeated Measures ANOVA. Significant improvements (i
Discussion
The present study describes the effects of 1 week training of Active Stretching and Eccentric Training on the spasticity of Hamstrings. The overall effect was assessed using three outcome measures i.e. Modified Tardieu Scale, GMFM score and Popliteal Angle.
We found out that 1 week of regular Active Stretching increases the Range of Motion at the knee and decreases spasticity of Hamstrings. It has been seen that Active Stretching has shown significant improvement within the group.Active stretching is much better over passive stretching because the rate of bond-breaking between actin-myosin is much more effective and has a long term effect. Also, in spasticity, actively stretching a muscle against the muscle’s contraction also helps in re- education of the movement pattern. The position of the lower extremity depends on the position of the pelvis and how the lower extremity is lifted. Therefore, in supine position, while doing Active Stretching one has to lift the lower extremity against gravity, overcome the resistance to lengthen the hamstrings and hold the position for a 30 second time period did a study the effects of a Single Session of Prolonged Muscle Stretch on Spastic Muscle of Stroke Patients. The results of the study conclude that 30 minutes of prolonged static stretching is effective in reducing motor excitability of Plantar Flexors in spastic hemiplegic patients (p= 0.001).
Eccentric Training was given for a 1 week period training and that it increased the Range Of Motion at the knee and decreasing spasticity of Hamstrings. It has been seen that Eccentric Training has shown better improvement within the group and better than Active Stretching.Eccentrically lengthening a muscle has many advantages. Gravity plays a major advantageous role in Eccentric muscle contraction. Eccentric lengthening of a muscle follows movement to be done towards gravity. A spastic muscle is in a continuous state concentric muscle contraction due to an Upper Motor Neuron disorder, which over a period of time leads to muscle tightness, contracture and finally irreparable deformities affecting daily activities and functional limitations hindering the physical and social outlook of the patient and society. Lengthening of such a spastic muscle with the help of gravity, actively will help in achieving both i.e. full active Range Of Motion and re-educating the movement pattern to the damaged motor cortex. Hence, Eccentric training over Active Stretching works better in spasticity. The rationale behind it might be due to the effect of gravity which clearly minimizes the effect of stretch pain and weight of the lower extremity while lengthening of Hamstrings in both the techniques. As compared to the Eccentric training, one will be made to lie in prone, and the lower leg will be lowered down much more easily done. So also, the resistance to spasticity or the continuous state of contraction of a spastic muscle is easily overcome while doing Eccentric training. This clearly implies that the position attained itself is beneficial for overcoming the lacunae observed due to Active Stretching.
However, while this latter supposition may essentially be correct, in our opinion a rigorous interpretation of the data on which it is based does not fully account the greater magnitude of improvements observed in Eccentric Training compared to Active Stretching because both of the techniques, do show a significant improvement and progress over time. To illustrate this foresaid point, in comparison with the present findings, a recent report revealed a far more modest and significant (p=0.05), improvement in lower extremity muscle strength after giving Eccentric Training. In this study, the available evidence supports the contentions that eccentric activation is an important aspect of muscle performance and that eccentric training may be a more effective and efficient method of increasing torque production than concentric training. This is purportedly due to increased restraint from stretch reflexes at incrementally higher speeds from a spastic antagonist muscle that is lengthening during a maximal concentric exertion in the agonist. This in effect serves to limit torque production in the agonist muscle. During eccentric activation, however, a spastic stretch response in the antagonist does not occur because that muscle is now shortening; therefore, any disruptions in eccentric performance cannot be attributed to spasticity. In a similar study children with CP demonstrated decreased eccentric and concentric peak torques for all muscle groups tested. The relative deficit in eccentric torque was less than the concentric torque and the decrement in concentric torque across speeds was greater in CP for all muscle groups except the ankle dorsiflexors. The E/C ratios for the knee extensors and flexors were also greater in CP.
Even though spasticity can be managed with abundant techniques, effectively measuring or quantifying spasticity or the resistance felt in a muscle or while doing a movement due to an Upper Motor Neuron lesion is still a matter of debate. It can also be said that researchers all over the world are improvising on the same and that the outcome measure to quantify spasticity is not yet fully standardized. But there are many scales and outcome measures which have been developed and improvised over the years. One of the initial scales for assessing spasticity is Ashworth Scale which was improvised to Modified Ashworth scale, and is still used in the present clinical scenarios. The only clinical scales that measure spasticity with a fast angular velocity are the less frequently used Held Scale (HS)(better known as the Tardieu Scale [TS] and the Modified Tardieu Scale (MTS)9 (p=0.001).
The Range Of Motion changes noted in this study are remarkable for several reasons. First, significant improvements in Range Of Motion are not normally expected as an outcome of short term stretching and Eccentric Training protocols. The reason for this is that stretching protocols are not standardized. Second, and perhaps more importantly, studies done on the effect on spasticity have indicated that include a clinical assessment of spasticity implies grading the intensity of the muscle tone and comparing it at different passive velocity stretches. Although ignored in Lance's definition, the patient’s testing posture and the initial length from which the muscle is stretched are both of significant influence on spasticity [8]. Furthermore, there is limited evidence in rehabilitation literature, to our knowledge, that spasticity is modifiable by exercise or can be altered to a meaningful degree at any time in cerebral palsy as a consequence of actively stretching the muscle and / or eccentrically training it. Thus, a clear- cut finding that children afflicted with cerebral palsy can achieve significant improvements in both Range Of Motion ,spasticity i.e. response or R1,resistance1 to fast velocity and functional activities in standing with the use of Active Stretching and Eccentric Training.
Indeed, on the basis of these results, taken as a whole, it may be reasonable to hypothesize that it might even be possible to alter the long term risks like developing gait abnormalities example crouch gait and others by vigorously promoting the regular and efficient use of these training modalities.
Although, there were substantial differences in length of treatment and focus of training programs that may account for some of the disparity in the training effects, it could also be hypothesized that some mechanisms other than a simple reversal of deconditioning might account for at least part of the ROM changes observed in the present study.
Although several alternative explanations may be offered to account for the exaggerated motor gains of the spastic extremity may be due to initial cortical sensorimotor stimuli to promote local terminal sprouting and/ or beginning of functional synaptic reorganization. Assuming this conceptual framework to be substantially correct, it should be possible to demonstrate by means of modern imaging or brain- mapping techniques whether and to what extent neo-cortical changes are induced as both the techniques are done actively. Although the suggested “Neuro Plasticity” model may be debatable in its details or appropriateness, there should be no serious disagreement that the ability of cortical motor areas to recruit spinal motor units in a well-co-ordinated and timely manner underlies effective synergistic muscle contraction and control of the antagonistic muscle and ultimately purposeful movement. However, it also remains possible that exercise mediated adaptations at the level of muscle itself, such as reversal of disuse atrophy could potentially account for part of the more robust relative gains in motor output.
It is quite possible that the substantial gains in Range Of Motion and improvement in spasticity and functional activities in standing observed (GMFM Score) in this study merely reflect overcoming the physical deconditioning associated with a sedentary lifestyle. Assuming the foresaid to be a sensible explanation, the present results, viewed in isolation, would represent an important clinical finding because they indicate that the deleterious effects of long standing physical deconditioning can be reversed or modified considerably by regular Active Stretching and Eccentric Training even in patients with a chronic disability for a better quality of life.
Thus, the basic question whether the improvements identified in this study are due to central or peripheral neuro-muscular adaptations remains unanswered.
We found out that 1 week of regular Active Stretching and Eccentric Training increases the Range Of Motion at the knee and decreases spasticity of Hamstrings. Additionally, there is improvement in functional (GMFM) outcome measure and Popliteal Angle too. In preliminary analysis, the measured improvement in R1 and R2 i.e. Modified Tardieu Scale (MTS) in Range Of Motion correlate in our test population of cerebral palsy with enhanced mobility and functional activity on conventional clinical measures of physical performance.
In summary, we report that 1 week of Active Stretching and Eccentric Training produces significant gains in Range Of Motion and spasticity to a considerable extent. We are persuaded that Eccentric Training so also Active Stretching can be a useful adjunct to traditional therapeutic interventions. The timing, frequency, intensity, duration of training requires future improvements in more rigorous randomized controlled trials.
Limitations
Small sample size.
Scope of Further Study
- Measuring the eccentric torque of the spastic muscle.
- Study can be studied in other muscles-Hip Adductors, Plantar flexors.
- The study can be evaluated using gait parameters as a functional outcome measure.
Conclusion
This study concludes that Eccentric Training has better improvement of Modified Tardieu Scale (MTS), GMFM Score and Popliteal Angle, over Active Stretching in reducing the Hamstrings muscle spasticity over a 1 week training program. Hence this study accepts the hypothesis that “Eccentric training is more effective than Active Stretching on Hamstrings spasticity in spastic cerebral palsy children.
References
-
Rosenbaum P, Stewart D (2004) The World Health Organization International Classification of Functioning, Disability, and Health: A Model to Guide Clinical Thinking, Practice and Research in the Field of Cerebral Palsy. Seminars in Pediatric Neurology 11(1): 5-10.
-
Scholtes VA, Becher JG, Beelen AB, Lankhorst GJ (2006) Clinical assessment of spasticity in children with cerebral palsy: a critical review of available instruments. Dev Med Child Neurol 48(1): 64-73.
-
Mackey AH, Walt SE, Lobb G, Stott NS (2004) Intraobserver reliability of the modified Tardieu scale in the upper limb of children with hemiplegia. Dev Med Child Neurol 46(4): 267-272.
-
Singh P, Joshua A (2011) study was to investigate Iintra-rater reliability of the Modified Tardieu Scale (MTS) in elbow flexors and ankle plantar flexors in adult subjects with stroke subjects. Ann Indian Acad Neurol 14(1): 23-26.
-
Dallmeijer AJ, Knol DL, Speth LA, Maathuis CG, Jongerius PH, et al. (2007) Effect of Multilevel Botulinum Toxin A and Comprehensive Rehabilitation on Gait in Cerebral Palsy. Pediatric Neurol 36(1): 30- 39.
-
Gracies JM, Burke K, Clegg NJ, Browne R, Rushing C, et al. (2010) Reliability of the Tardieu Scale for assessing spasticity in children with cerebral palsy. Arch Phys Med Rehabil 91(3): 421-428.
-
Damiano DL, Martellotta TL, Quinlivan JM, Abel MF (2001) Deficits in eccentric versus concentric torque in children with spastic cerebral palsy. Med Sci Sports Exerc 33(1): 117-122.
-
Dodd KJ, Taylor NF, Damiano DL (2002) A systematic review of the effectiveness of strength‐training programs for people with cerebral palsy. Arch Phys Med Rehabil 83(8): 1157-1164.
-
Tsai KH, Yeh CY, Chang HY, Chen JJ (2000) Effects of a Single Session of Prolonged Muscle Stretch on Spastic Muscle of Stroke Patients. Proc Natl Sci Counc Repub China B 25(2): 76-81.
-
Thompson N, Stebbins J, Seniorou M, Newham D (2011) Muscle strength and walking ability in diplegic cerebral palsy: implications for assessment and management. Gait Posture 33(3): 321-325.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial