Number of Psychiatric Diagnoses and Falls in People with Huntington’s Disease (HD) in the National Inpatient Sample (NIS)
Background: Recent publications by the American Occupational Therapy Association (AOTA) and the American Physical Therapy Association (APTA) aim at guiding families and therapies in strategies that make movement in the home and the community safer for patients with HD. Huntington’s disease (HD) is an autosomal dominant neurodegenerative disorder resulting in deficits in motor, cognitive and psychiatric function. Hospitalizations due to HD and its complications are common during some stage of the illness. Falls, multiple medical conditions, poor ability to breathe or swallow and acute psychiatric distress have been noted as some of causes leading to hospitalization. Objectives: Determination of correlations between falls, severity levels, admitting diagnosis and number of ICD-10 codes for psychiatric comorbidities was reviewed in the Healthcare cost and Utilization Project (HCUP) data for the 2016 National Inpatient Sample (NIS) for inpatients with HD. Methods: Patient cases in the 4th quarter of the NIS were searched for inpatients with HD as their admitting, 2nd, 3rd and 4th diagnosis until N=230. Secondary data analysis compared variables in the NIS. Results: Level of severity was consistently higher for hospitalization within patient severity levels 2 and 3 in the sample at 72%. Severity of HD diagnosis when admitting diagnosis was HD, was statistically significant differences with the majority of inpatients injuries or fall HD severity was reported as level 2. Falls were most significantly correlated when compared to the number of psychiatric diagnosis on record (p <.001). Discussion: The most significant mild predictor of falls (33.4%) was the presence of multiple additional inpatient psychiatric diagnoses including dementia, anxiety, depression, bipolar disorder and schizophrenia. Chi-Squared analysis results indicated the greatest difference between expected falls and actual falls occurred in the presence of multiple psychiatric diagnosis’s (p<.001). Researchers in occupational and physical therapy investigating falls in the HD population could benefit from proposing psychiatric frames of reference for treatments for falls in addition to organized strategies of exercise and improvement of motor control.
Introduction
Attempting to determine fall risk for patients with HD and designing effective programing has been challenging for physicians and clinicians. Some authors report that though HD is a neurological disease, it commonly presents itself with psychiatric symptoms in approximately 80% of patients [1, 2, 3, 4]. The question of treatment thus focuses on the cause of the dysfunction. Are falls a result of impaired modulation of motor responses as the basal ganglia dysfunction causes obvious impairment in grading movement or due to an alternative psychiatric reason? Are falls the result of psychiatric presentations where patients are on medications that present fall risks or are a subset of HD patients refraining from eating/drinking due to psychosis and/or other psychiatric symptoms that would lead to falls and hospitalization?.
The recent role of balance confidence and falls has inferred that impaired cognitive ability and lack of confidence in balance, report higher fall levels in other diseases that present with motor impairment. Impaired gross motor control, including impaired postural stability indicated by an increase in postural sway and impaired vestibular and sensory testing, has been reported for HD patients both before and after showing predominant symptoms [5].
Declines in function severe enough for patients with HD to decide to leave their place of employment are often caused by the combination of emerging cognitive and motor symptoms [6].
A recent study utilized Transcranial sonography (TCS) to review the neurologic and psychiatric presentations of HD [7]. Though the sample size (N=39) was relatively small, and neuroleptic medications may have had an effect on outcomes making generalization of the findings difficult, 70.6% of the patients exhibited psychiatric symptoms before the onset of motor involvement. In addition, the majority of the samples TCS results indicated pathology in the brainstems raphe nuclei responsible for important production of neurotransmitters associated with mood.
Recent publications by the American Occupational Therapy Association (AOTA) and the American Physical Therapy Association (APTA) aim at guiding families and therapies in strategies that make movement in the home and the community safer for patients with HD [8]. In home exercises programs, providing predictable routines and recommendations for safe sleeping and mobility has been designed in attempts to keep patients in the home safe. Little indication of fall risk due to multiple psychiatric symptoms exist, though overall protocols for dementia are encouraged.
Methods
Nationally available data was obtained from the HCUP website, purchased and certifications for use were obtained. Data from 2015 was utilized for this study, specifically from the 4th quarter, as earlier quarters had not yet transferred to the new international classification updates. The first 5 diagnosis codes were searched for HD and the already deidentified cases were transferred into SPSS-23 merged on NIS number.
Results
Descriptive Data
The International classification for disease, version 10 (ICD-10) diagnosis 1-5 was searched for NIS HCUP data cells for patients with Diagnosis G.10 (HD). Nearly eight percent (7.8%) of patients had an admitting or additional diagnosis of malnutrition or diagnoses related to reduced caloric intake or electrolyte imbalances, while 13.5% of patients had an admitting or additional diagnosis or fall or injury due to falls. The percentage of patients who had an admitting or additional cognitive or psychiatric diagnosis reached 19.1%, and 19.7% of patients had an admitting or additional diagnosis of other medical (Figures 1 & 2).
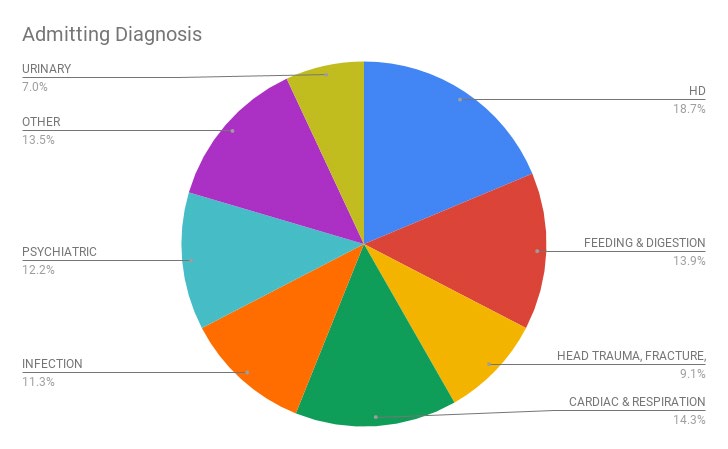
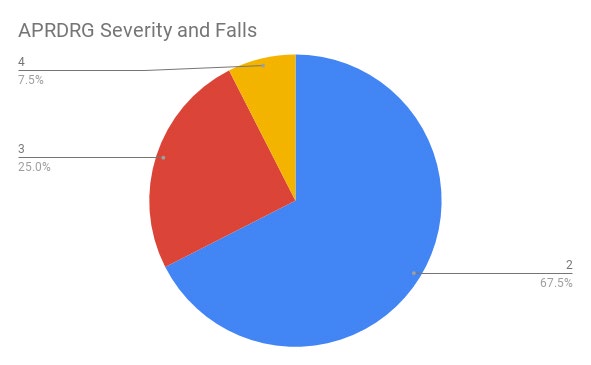
Only 3.4% of patients were admitted for palliative care, and 5.2% of patients had an admitting or additional diagnosis of swallowing or speaking difficulties. Only 2.6% of patients had an admitting or additional diagnosis of musculoskeletal disorders. The number of patients with HD were admitted for a reason other than a fall was N=192 (Tables 1 & 2) whereas the Approximated Odds Ratio was 19.8 indicating Chi-Square Test the majority of the sample was admitted for reasons other than a fall (Table 3).
| HD admissions* | ||||
|---|---|---|---|---|
| No Fall | Fall | |||
| Cog/Psych Dx | None listed | Count | 93 | 7 |
| Expected Count | 86.5 | 13.5 | ||
| Dementia | Count | 27 | 3 | |
| Expected Count | 26 | 4 | ||
| Other Psych | Count | 45 | 5 | |
| Expected Count | 43.3 | 6.7 | ||
| Multiple Psych | Count | 33 | 16 | |
| Expected Count | 42.4 | 6.6 |
Table 1: ** Cognitive or Psychiatric ICD-10 and fall, Expected Versus Actual Counts. Binary/Logistic Regression Level of severity
*X2=20.003, df=4, p≤.001 Table 1: Cognitive or Psychiatric ICD-10 and fall, Expected Versus Actual Counts. Binary/Logistic Regression Level of severity, psychiatric illness and cognition, and LOS determine predictors of falls with a binary regression examining the entire NIS HD sample (N=230).
| Observed | Predicted | ||||
|---|---|---|---|---|---|
| Fall on file_No fall on file | Percentage Correct | ||||
| No fall on file | Fall on file | ||||
| Step 0 | Fall on file_No fall on file | No fall on file | 192 | 0 | 100 |
| Fall on file | 38 | 0 | 0 | ||
| Overall Percentage | 83.5 | ||||
| a. Constant is included in the model. | |||||
| b. The cut value is .500 |
Table 2: Classification Tablea,b.
B S.E. Wald df Sig. Exp(B)
| Step | -2 Log likelihood | Cox & Snell R Square | Nagelkerke R Square |
|---|---|---|---|
| 1 | 155.442a | 0.198 | 0.334 |
Table 3: Model Summary.
Correlations
Spearman one-tailed correlations also indicated cognition and psychiatric diagnoses had a statistically significant relationship to falls (r = .337, p ≤ .001). Falls were significantly correlated with total charges (r = .121, p ≤ .036). Falls were significantly correlated with admission by Emergency Department record (r = .234, p ≤ .042). When grouping ages, there was a statistically significant correlation between age groups and severity of illness (r = .291, p ≤ .001).
The results of Table 1 indicate that cognitive and psychiatric conditions appear to be statistically associated with falls. HD patients in the NIS diagnosed with multiple psychiatric conditions fall more than expected. The Nagelkerke R Square indicates a value of .334; indicating the model is a mild predictor of falls by approximately 33.4% (Table 4).
Discussion
Occupational therapy and physical therapy in recent years have added useful protocols for HD patients and families. Improvement of motor control with exercise protocols have been researched in both animal and human HD studies [9, 10, 11]. Psychiatric disturbances and medication regimes have been widely investigated in recent years with patients with HD. Cognitive and psychiatric characterizations are being found to impact function more, or at least as much as, motor impairments [12, 13]. The current secondary data analysis of the NIS found that inpatients with HD with falls on record were more likely to have multiple psychiatric ICD- 10 codes listed in their medical record than inpatients with HD admitted for other reasons. Clinicians and physicians may consider when planning treatments, not only mobility risks of environmental modification, but variables such as psychiatric status, medication regime and these effects on fall risk. Future studies may examine dosage and medication types and other types of cognitive or psychiatric treatments in HD patients at risk for falls in addition to the physical exercise protocols that have recently been reported to be helpful interventions.
References
-
Langbehn DR, Brinkman RR, Falush D, Paulsen JS, Hayden MR (2004) A new model for prediction of the age of onset and penetrance for Huntington’s disease based on CAG length. Clinical Genetics 66(4): 267-277.
-
Epping EA, Kin JI, Craufurd D, Bashers Krug TM, Anderson KE, et al. (2016) PREDICT-HD investigators and coordinators of the Huntington Study Group. Longitudinal psychiatric symptoms in prodomal Huntingtons disease: A decade of data. American Journal of Pyschiatry 173(2): 182-192.
-
Rao AK, Gilman A, Louis ED (2014) Archives of Physical Medicine Rehabilitation 96(10): 1832-1837.
-
Dubas Slempt H, Tylec A, Micalowska Marmurowska H, Spychalska K (2012) Is Huntington’s disease a neurological or psychiatric disease?. Psychiatry Pol 46(5): 915-922.
-
Salomoncszk D, Panzera R, Pirogovosky E, Goldsten J, Corey Bloom J, et al. (2010) Impaired postural stability as a marker of premanifest Huntington’s disease. Movement disorders 25(14): 2428-2433.
-
Watkins K, Purks J, Kumar A, Sokas RK, Heller H, et al. (2018) Sept 4 Huntington’s disease and employment: The Relative contributions of motor and cognitive decline to the decision to leave work. Journal of Huntingtons disease 7(4): 367-377.
-
Crogias C, Strassburger K, Eyding J, Gold R, Norra C, et al. (2011) Depression in patients with Huntingtons disease correlates with alterations in the brain stem raphe depicted by transcranial sonography. J Psychiatry Neuroscience 36(3): 187-194.
-
(2016) American Occupational Therapy Association. Making the home safe.
-
Busse ME, Wiles CM, Rosser AE (2009) Mobility and falls in people with Huntington’s disease. 80(1).
-
Dawes H, Collett J, Debono K, Quinn L, Jones K, et al. (2015) Exercise testing and training in people with Huntington’s disease. Clinical Rehabilitation 29(2): 196- 206.
-
Grimbergen YAM, Knol MJ, Bloem BR, Kremer BPH, Roos RAC, et al. (2008) Falls and gait disturbances in Huntington’s disease. Movement Disorders 23(7): 970- 976.
-
Soliveri P, Monza D, Piacentini S, Paridi D, Nespolo C, et al. (2002) Cognitive and psychiatric characterization of patients with Huntington’s disease and their at-risk relatives. Neurological Sciences 23: 105-106.
-
Teri L, Gibbons LE, McCurry SM, Logsdon RG, Buchner DM, et al. (2003) Exercise plus behavioral management in patients with Alzheimer disease: A randomized control trial. Journal of the American Medical Association 290(15): 2015-2022.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial