Congenital Dislocation of the Knee in a Newborn
Congenital dislocation of the knee (CDK) is a relatively rare condition with an estimated prevalence of 1 per 100 000 live births, which is approximately 1% of the incidence of developmental dysplasia of the hip1. It may occur in isolation, but often occurs in the presence of muscle imbalance such as that seen with arthrogryposis, Larsen syndrome, and myelomeningocele. CDK has also been reported to occur with other musculoskeletal abnormalities including developmental hip dysplasia, clubfoot, congenital vertical talus, and congenital dislocation of the elbow2.
Introduction
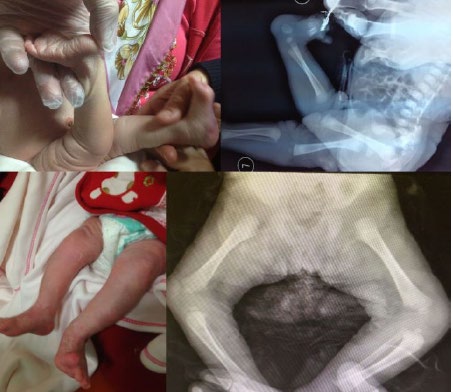
A 2700-g-female newborn was delivered by spontaneous vertex delivery to a-18 year-old mother at 394/7 gestational weeks. There was no history of oligohydramnios. The newborn had deformity as hyperextension at her knees bilaterally on initial examination (Figure 1a). No other physical anomaly was observed, and there was no family history of knee, hip, or foot deformity. Hyperextension of the knees ranged from -10° to -70° and both of them could be flexed to 90° passively. The radiograph showed the tibia as dislocated anteriorly (Figure 1b). Serial casting was started for treatment within 24 hours. The degree of hyperextension decreased gradually starting from the first week with casting, and the knee flexed fully within two mounts. Displasy of the left hip were detected during the eight months follow up. And treated with abduction brace. Figures 1c & 1d show the last examination and radiograph of the patient at 7 months of age [1].
Clinical Note
Discussion
Congenital dislocation of the knee (CDK) is a relatively rare condition with an estimated prevalence of 1 per 100 000 live births, which is approximately 1% of the incidence of developmental dysplasia of the hip. It may occur in isolation, but often occurs in the presence of muscle imbalance such as that seen with arthrogryposis, Larsen syndrome, and myelomeningocele. CDK has also been reported to occur with other musculoskeletal abnormalities including developmental hip dysplasia, clubfoot, congenital vertical talus, and congenital dislocation of the elbow [2].
Conclusion
The range of movement at the joint and any limitation of flexion are important to note. Although spontaneous reduction of CDK has been previously described in few cases, serial casting or splinting and occasionally surgery are still the main therapy strategies [3, 4]. Conservative treatment strategies may be suitable especially in newborn with isolated CDK such as in our patient.
References
-
Jacobsen K, Vopalecky F (1985) Congenital dislocation of the knee. Acta Orthop Scand 56: 1-7.
-
Shah NR, Limpaphayom N, Dobbs MB (2009) A Minimally Invasive Treatment Protocol for the Congenital Dislocation of the Knee. J Pediatr Orthop 29: 720-725.
-
Abdelaziz TH, Samir S (2011) Congenital dislocation of the knee: a protocol for management based on degree of knee flexion. J Child Orthop 5: 143-149.
-
Haga N, Nakamura S, Sakaguchi R, Yanagisako Y, Taniguchi K, et al. (1997) Congenital dislocation of the knee reduced spontaneously or with minimal treatment. J Pediatr Orthop 17: 59-62.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial