Effect of Pilates Vs. Yoga on Balance, Cognition and Core Strength in Elderly
Background: In older people, falls have become a major health issue. People aged 65and above are more prone for most frequent accidents which can lead to injury related hospitalisation. Elderly people have many serious health issues and they have several disorders affecting their body at the same time. Pilates is kind of exercise that uses a combination of muscle that increases power, stretches muscle and also concentrate on breathing to develop strength of the trunk muscles and restore muscle balance for physical fitness. Yoga is the active engagement between the mind and body. Yoga focuses specifically on what is exactly happening is the body and where the body is actually moving in space which increases both awareness and proprioception. Objective: To study the effect of Pilates on balance, cognition and core strength. To study the effect of Yoga on balance, cognition and core strength. To compare the effect of Pilates Vs. Yoga on balance, cognition and core strength in elderly. Method: There were two groups Pilates and Yoga. 30 subjects were sequentially divided in both groups. The treatment was given for 3 days a week for 4 weeks. The outcome measures were taken at the beginning and at the end of 4th week. Result: The Pilates group is having statistically significant improvement in balance .The Yoga group is having statistically significant improvement in cognition. The core strength is clinically significant in Pilates group. Conclusion: This study concluded that Pilates and Yoga both are equally effective in improving cognition, balance and core strength at the end of 4 weeks protocol, yoga group showed marked increase in cognition whereas pilates group showed marked increase in balance and core strength.
Introduction
Today people live longer worldwide and now can expect to live beyond their sixties. There is a dramatic increase in the frequency of population ageing in the world [1]. There are two inseparable concepts called demographic transition and population ageing. The process of demographic transition have a resultant product called population ageing [2].
The ageing results are having mark impact by the gathering of vivid variety of cell level and molecular level changes over the period of time. Progressive decline in physical and mental capability, progressive risk of disease and progressively death are all carried out because of the process of ageing. Characteristics of older age is development of plenty of difficult level of health issue which are supposed to appear only in later stage of life and also those does not come into separate categories. Those are known as old age syndromes commonly [1].
Changes in Skeletal Muscle
Reduction in performance of skeletal muscle is the significant factor of responsible factor of physical inability and progressive age. The reduced level of work done by skeletal muscle is in the form of sarcopenia [3]. Regulating factors of elderly skeletal muscle performance are nervous, muscular and skeletal systems [4]. Grossly, physiological and/ or anatomical degeneration will lead to decrease performance of skeletal muscle which are carried over by the way of living, biological and psychological elements [5].
Nervous system along with skeletal system controls more than 500 skeletal muscles [6]. The smallest functional unit of skeletal muscle fibre which goes under constant pumping which leads to movement of body like fast and powerful or small and time motions. Loss of sarcomere, difference in muscle fibre type and muscle atrophy, decreased level of activation of junction of nerve and muscle could affect the kinematics of muscle like velocity, force, strength of movement that ultimately leads to functional disability and hospitalization. Importance of maintaining muscle health throughout life truly depends on the metabolic functions and role of myokines [7].
Neuralogical Control of Muscles and Motion
Nervous system controls the largest movement and forces of human body skeletal muscle. The neural control of skeletal muscle goes as follows:
Produces co – ordination, targeted movements [8].
Neurological Factors Responsible for Muscular Decline in Elderly
Motor neurons and muscle fibres are recruited more and more as the voluntary contraction force of muscle increases. Major factors of timing and strength of voluntary contractions comes from descending tract from motor cortex [9]. According to the previous studies, functionally healthy older adults usually will not lead difficulty in voluntary muscle activation and visa versa for the weaker older people [10, 11].
According to the prediction, amongst the total mass of people 22% are having old age than 60 years and 5 % will be counted of having old age till 2050 [12] in India due to improved quality of life and life expectancy the population ageing is showing an upward going and rising sharp graph [13]. As the age progresses, the population will have increased incidence of physical performance limitations. Those limitations leads to the risk of falls. So in today’s world prevention of limitations and treatment of physical performance improvement are very much important for public health benefits [4].
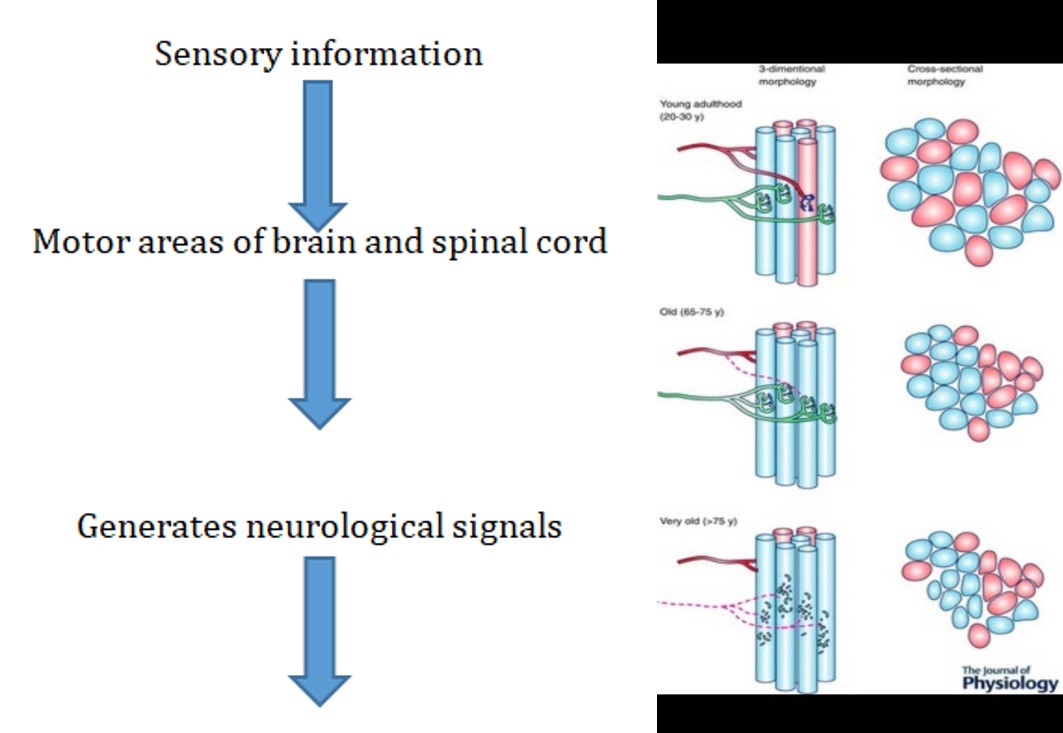
Ageing Muscle Morphology and Neurophysiological Manifestation
According to the figure showed below,
• Young adulthood shows the interconnected threads of
muscle which are part for varied motor units.
- Starting from adult life to elderly shows cycle of denervation – re innervation.
- Elderly is showing increased number of axonal ageing which eventually leads to grouped fibre atrophy [14].
Sensory and motor inputs contribute to declines in balance with age. Progressive decline in spinal motor neurons causes reduced in muscle fibre number and size i.e. sarcopenia, these results in reduced mechanical muscle performance, decreased muscle strength, power and force that eventually reduces functional capacity during everyday tasks due to the effects of ageing. Along with balance, strength, cerebellar integrity, Vestibulo – cochlear function, hearing and vision & proprioception all contributes for the falls in elderly [15].
Changes of ageing includes repeating cycles of denervation and re innervation which leads to grouping of fibre and extension of living MUs, neuronal loss, instable neuromuscular junction. Along with strength and power ageing also leads to impaired co – ordination that collectively cause falls and physical imperfection in performance [14].
All our systems, organs and tissues are all affected by the fundamental process of ageing. Total body decline is inevitable with ageing but it depends on person to person that at which rate and magnitude it makes changes in each system [16].
In older people, falls have become a major health issue. People aged 65and above are more prone for most frequent accidents which can lead to injury related hospitalisation. Disability, loss of independence and increased mortality are all associated with fall injuries [17]. A restricted activities related to daily life are the eventual results of falls in elderly are defined as a feeling of fear of fall. Fear of falling is multi factorial and multidimensional, which is widely accepted. Decreased functional capacity, impaired cognitive capacity and depression those all are responsible for feeling of fear of falling in both gender having old age [18].
Prevention of fall and assessment of balance training is helpful in counteracting the age related decline in function and aids in prolonging independence in elderly individuals [19]. Depending on the risk factors identifying and treating the reasons prevents the consequences of falls [20].
The complex interaction of neuromuscular, proprioceptive, vestibular and visual system is required for the ability to maintain balance in humans. And with ageing performance of many of these system declines gradually which results in impaired equilibrium and eventually progresses to risk of falling in elderly. Maintenance of balance and functional mobility in elderly is very important [20].
Many years ago an exercise was developed relayed on the eastern philosophical principle and motion technologies such as Yoga and western method of body conditioning such as P.H.ling’s medical gymnastics by JOSEPH PILATES (1880 – 1967). This method was developed for the core muscle which had more than 500 techniques of improving muscle flexibility and muscle strengthening exercise which is divided into two different categories: Mat pilates and pilates using Apparatus [21].
Pilates is kind of exercise that uses a combination of muscle that increases power, stretches muscle and also concentrate on breathing to develop strength of the trunk muscles and restore muscle balance for physical fitness. In Pilates one will have to activate several groups of muscles at the same time. This works on the co – activation and co - ordination of the muscles. Recent studies suggested that now a days Pilates exercise is used by many people of different age group, people having different body type and poeple having different level of physical ability because of flexibility of changes [22].
We can assume that Pilates is a different kind of physical movement that engages mind to focus on what the boding is doing. Which helps in increasing the cognitive functions? Researchers have found that when one has to think about how their body is moving, their brain cells grow at a faster rate and their nervous system creates better connections throughout the body.
Effect of Pilates on Cognitive Function:
- It helps in improving circulation and oxygenation in the brain
- Brain derived neutrophin supports neuronal survival in developing brain
- It provides mood enhancement
- Generates new neurons
- Increases neurotransmitters [23]
Yoga is considered as one of the complementary and alternative therapies which is more theorized as therapeutics than traditional exercise as it involves mind and body component. Yoga is active coordination of body and mind. Yoga focuses particularly on what is exactly happening in the body and how the body is actually being moved in the space which increases proprioception and consciousness. As yoga have gentle movements is can be addressed to prevent the risk of falls in persons having reduced balance, difficulty in mobility, decreased muscle strength and flexibility and it also focuses that how one can increase the awareness and proprioceptive function which can decrease the fear of fall and improve balance in elderly.
Need for Study
Aging is associated with the common problem of cognitive impairment with occurrence rate of approximately 21.5 – 71.3 per 1000 person/ year in old age population. Mild cognitive functions can range from 3% to as high as 42% in population and 6% to 85% in clinical setting. Maintenance of balance and functional mobility in elderly is the result of very important strengthening of core muscles. Activation and co – ordination of several muscle groups at the same time is the classical feature of Pilates exercise. This exercise suits to people having different age, different body type and different level of physical ability due to flexibility in changes in movement. Active engagement of mind and body simultaneously is the classical characteristic of yoga therapy. Mind is stimulated to engage the focus on what is happening in the body and how the body moves in the space. That increases both proprioception and consciousness. There are few studies which have given the combined treatment of Pilates and yoga on balance and there are also few studies which individually saw the effect of Pilates on balance or cognition or core strengthening, but not a single studies have compared the effect of Pilates and yoga on balance, cognition and core strengthening in elderly. So this study is needed to compare the effect of Pilates and yoga on balance, cognition and core strengthening in elderly.
Aims: To study the effect of Pilates Vs. yoga on balance, cognition and core strength in elderly. Objectives: To study the effect of Pilates on balance, cognition and core strength. To study the effect of yoga on balance, cognition and core strength.to compare the effect of Pilates Vs. yoga on balance, cognition and core strength in elderly. Methodology: participants recruited were elderly individuals coming regularly at konkane chowk public garden pimple saudagar are. Selected were of age 65-75 year. Demographic data was collected from all the individuals. Which includes name, age, gender and occupation, address and contact details. Participants were asked about their past medical history that is about hypertension and recent surgical history in past year. This was documented for all the patients. A questionnaire form was filled by all patients through interview method for measuring fear of fall efficacy scale – international (FES-I).
A total number of 30 individual selected for the study according to inclusion and exclusion criteria was elderly people with the age of 65 – 75 years. Not participating in any sports or any physiotherapy sessions. Willingness to do physical exercise thrice a week with regular attendance. Fall efficacy scale score more than 16. Montreal assessment scale score less than 23 are included.
Exclusion Criteria
Any neurological disease and cardiovascular disease. Any psychiatric conditions, Malignancy, Medications known to effect muscle strength. Recent fractures. Any recent soft tissue injury.
Now they were divided into two groups, Pilates group and yoga group through sequential allocation. Participants were informed about the benefits and possible risk which mainly includes muscular soreness. Thus written consent was taken from all the subjects. Ethical approval was taken from institutional ethical; committee.
Baseline parameters for balance, cognition and core strength were assessed for all individuals by using berg balance scale, Montreal cognition scale and pressure biofeedback. Public garden at konkane chowk pimple saudagar area was use as a study setting where exercise was given to both the groups.
Participants of both the groups were called for exercise sessions for 4 weeks, 3 times a week for 45 min each session. Pilates and yoga both were practised using Mat. After completing the 4 week protocol the outcome measures were assessed again.
![Figure 2: Motor unit alteration in ageing muscle by morphological view [11].](/fulltextimages/6257/fig_2.png)
Outcome Measures
Balance was measures using the berg balance scale. Cognition was measured using the Montreal cognition scale and the core strength was measured using the pressure biofeedback.
Statistical Analysis
The outcome measures were assessed and the values obtained were documented and tabulated for statistical analysis. Pre post assessment within group was done by paired t – test or wilcoxon test respective to the normality of the data. Pre post assessment between groups was done by using t – test or Man Whitney Rank sum test respective to the normality of data.
The outcome measure were assessed for both group A (Pilates) and group B (Yoga) all subjects were taken that is n = 11 each.
Data Analysis and Interpretation
| Pilates | Yoga | |
|---|---|---|
| N | 15 | 15 |
| Gender | Male = 10 | Male = 7 |
| Gender | Female = 5 | Female= 8 |
| Mean age | 69 | 68.67 |
| SD | 3.703 | 3.478 |
| P value and t value | P= 0.801 | |
Table 3: Characteristics of Subjects of Both the Groups.
Table 1 shows mean age of participants of both the groups. Graph 1b shows male and female ratio in Pilates and yoga groups. After applying t – test on mean age between groups (p = 0.801) were not found significant. Hence both the groups were comparable as the participants were of same age group.
| Pilates | Yoga | |
|---|---|---|
| Pre mean + SD | 19.93+2.086 | 19.07+4.044 |
| Post mean + SD | 21.47+1.995 | 22.93+4.317 |
| P value | 0 | 0 |
Table 5: Montreal Cognition Assessment Scale score of both groups (within).
Table 2 shows that there is marked increase in score of Montreal Cognition Assessment Scale in yoga group. While in Pilates group there is slight increase observed in Montreal Cognition Assessment Scale score.
| Pilates | Yoga | |
|---|---|---|
| Pre mean + SD | 43.87±1.995 | 44.2±3.167 |
| Post mean + SD | 49.93±2.086 | 47.27±3.127 |
| P value | 0 | 0 |
Table 7: Berg balance scale score of both groups (within).
Table 3 shows that there is marked increase in berg balance scale score in Pilates group while there is slight increase observed in yoga group in berg balance scale score.
| Pressure biofeedback | Pilates | Yoga | |
|---|---|---|---|
| Pre mean + SD | 72.2±2.507 | 72.2±4.632 | |
| Post mean + SD | 67.2±1.265 | 68.4±1.882 | |
| P value | 0 | 0.001 |
Table 1: Pressure biofeedback score of both groups (within).
Table 4 shows that there is marked improvement in both Pilates and yoga group in pressure biofeedback score.
| Montreal cognition scale | Pilates | Yoga | |
|---|---|---|---|
| Mean + SD | 1.533±0.7432 | 3.867±1.125 | |
| Gender | Male = 10 | Male = 7 | 0 |
| Gender | Female = 5 | Female = 8 | 0 |
Table 2: Comparison of difference in Pilates and Yoga group for Montreal Cognition Assessment Scale score (between).
Table 5 shows that in comparison between the groups for the Montreal Cognition Assessment Scale score there is marked increase in cognition score in yoga group. While in Pilates group there is slight increase observed in cognition.
| Berg balance scale | Pilates | Yoga |
|---|---|---|
| Mean + SD | 6.067±2.12 | 3.067±0.9612 |
| P value | 0 | |
Table 4: Comparison of difference in Pilates and yoga group for berg balance scale score (Between).
Table 6 shows that in comparison between the groups for the berg balance scale score there is marked increase in balance score in Pilates group. While in yoga group slight increase was observed in cognition.
| Pressure biofeedback | Pilates | Yoga |
|---|---|---|
| Mean + SD | -2.829 | -0.13 |
| P value | 0.097 | |
Table 6: Comparison of difference between Pilates and yoga for pressure biofeedback (Between).
Table 7 shows that in comparison between the groups for the pressure biofeedback score there is marked improvement in the Pilates group. While in yoga group slight improvement was observed in core strength. Here the minus data indicates the improvement.
Results
Data obtained was analysed using paired t-test and Wilcoxon test for within group and t – test and Man Whitney test for between group comparison for pre post values of both groups and following results were found. Table 1 shows the demographic characteristics of subject of both the groups. Table 2 shows that Montreal Cognition Assessment Scale score was significant statistically within group for both Pilates and yoga with p values of 0.000 and 0.000 respectively. Table 3 shows that berg balance scale score was significant statistically within group for both Pilates and yoga with p values of 0.000 and 0.000 respectively. Table 4 shows that pressure biofeedback score was significant statistically within group for both Pilates and yoga with p values of 0.000 and 0.001 respectively. Table 5 shows that comparison between Pilates and yoga for Montreal Cognition Assessment scale score was highly significant statistically with p value of 0.000. This result also co – relates with the clinically significant effect of yoga over Pilates. Improvement is seen in both the groups but clinically yoga group shows more improvement. Table 6 shows that comparison between Pilates and yoga for berg balance scale score was highly significant statistically with p value of 0.000. This result also co – relates with the clinically significant effect of Pilates over yoga. Improvement in balance is seen in both the groups but Pilates group shows more improvement. Table 7 shows that comparison between Pilates and yoga for pressure biofeedback score was not statistically significant with p value of 0.000. But this result contradicts the clinically significant effect of Pilates over yoga. Clinically improvement is seen in both the groups but Pilates group shows more improvement. The result of the study found that cognition was highly statistically and clinically significant for yoga group with p value of 0.000. Balance measured through berg balance scale was highly statistically and clinically significant for Pilates group. This study also shows that core strength measure with pressure biofeedback was not significant statistically with the p value of 0.097 but it is definitely clinically significant for the Pilates group.
Discussion
Our study is comparing the effect of pilates and yoga programs on cognition, balance and core muscle strength in elderly with age of 65 – 75 years. The subjective assessment of participants was done and outcome measures were analysed like cognition, balance and core strength through Montreal cognition scale, berg balance scale and pressure biofeedback respectively. Group A received Pilates intervention and Group B received yoga intervention.
According to study of Gonul Babayigit, et al. improvement in dynamic balance, muscle flexibility, reaction time and muscular strength could be done by Pilates exercise for reducing the number of falls in older age women and they concluded that improvement in dynamic balance, muscle flexibility, reaction time and muscle strength can be done by pilates as well as it can reduce the tendency of fall in older women. Here we can find out the reason that why the Pilates will have marked improvement in the balance and core strength components, that is because as in a multi-storeyed building the base is the important element similarly the core muscles are the base of our body. As Pilates directly work on the core muscle according to its principles, we could connect the strings that once the base i.e. the core muscles are strengthened the body will have its equilibrium and balance in space and eventually balance shows improvements.
In one recently study done by Hishikawa N, et al., in on the effect of yoga and exercise together promotes cognitive, affective and physical functions in old age people he concluded that Cognitive, affective, ADL, and physical functions in a local older age people. Populations were improved by yoga plus exercise which indicates the benefits in preventing dementia among elderly individuals. In our study also the yoga group is showing marked improvement than Pilates group so this study findings supports our study.
The ultimate reason behind the improvement in cognition in yoga is because whenever the yoga postures are being held or assumed the muscles are engaged and focused and it goes in a state of attention and the similar happens during the meditation. In the meditative process there is increased level of oxyhemoglobin in the pre frontal cortex due to the increased blood flow to that area of brain. This eventually improves the cognition but this process takes a longer duration studies to be followed. In this current study it was found that participants in the yoga group showed improvement significantly in the cognition and while Pilates group showed improvement significantly in balance and core strength.
Conclusion
This study concluded that Pilates and yoga both are equally effective in improving cognition, balance and core strength at the end of 4 weeks protocol, but there was marked increase in cognition in yoga group whereas the Pilates group showed marked increase in balance and core strength.
References
-
WHO (2018) Ageing and health. World Health Organization.
-
Ahmad WIW, Astina IK, Budijanto B (2015) Demographic Transition and population ageing. Mediterranean Journal of social science 6(3).
-
Janssen I (2002) Low relative skeletal muscle mass (Sarcopenia) in older persons in associated with functional impairment and physical disability. Journal of Geriatric Society 50: 889- 896.
-
Fiatarone MA, Marks EC, Ryan ND, Meredith CN, Lipsitz LA, et al. (1990) High intensity strength training in nonagenarians. Effects on skeletal muscle. JAMA 263(22): 3029-3034.
-
Fiatarone MA, O’Neill, solares GR, Nelson ME, Ryan ND, et al. (1994) Exercise training and nutritional supplementation for physical frailty in very elderly people. N engl J med 330: 1769-1775.
-
Jones HR, Burns T (2013) The netter collection of medical illustrations: Nervous system, spinal cord and peripheral motor and sensory system. 2nd (Edn.), Philadelphia: Elsevier
-
Ried KF, Fielding R (2012) Skeletal muscle power: a critical determinant of physical functioning in older adults. Exere sport sci Rev 40(1): 4-12.
-
Kandel ER, Schwarts JH, Jessell TM, Siegelbaum SA, Hudspeth AJ (2013) Principles of neural science. 5th (Edn.), United States of America: The McGraw-hill companies.
-
Ashe J (1997) Force and the motor cortex. Behav Brain Res 87: 255-269.
-
Power Ga, Minozzo FC, Spendiff S, Filion ME, Karokhova Y, et al. (2016) Reduction in single, muscle fiber rate of force development with aging is not attenuated in world class older masters athlets. AMJ physiol cell physiol 310(4): C318-C327.
-
Tieland M, Trouwborst I, Clark BC (2017) Skeletal muscle performance and aging. Journal of cachexia, sarcopenia and muscle 9(1): 3-19.
-
United Nations (2012) Population ageing & developmental. In: Do Eas (Eds.), New York.
-
Mathur S (2015) Demographic transition and population ageing in India: Implication on the elderly of the future. Global journal of medicine and public health 6.
-
Hepple RT, Rice CL (2016) Innervation and neuromuscular control in aging skeletal muscle. J Physiol 594(8): 1965-1978.
-
Aagaard P, Suetta C, Caserotti P (2010) Role of the nervous system in sarcopenia and muscle atrophy with aging: strength training as a counter measure. Scand J Med Sci Sports 20(1): 49-64.
-
Mohmadi M, Bize R, Johnson AJ, Ronald C (2017) Journal of preventive medicine 45: 401-415.
-
Guccione AA, Avers D, Wong R, Brown M (2011) Physiology of age related and lifestyle related decline, geriatric physical therapy. 2nd (Edn.), Elsevier health science.
-
Lavendan A, Viladrosa M, Jürschik P, Botigué T, Nuín C, et al. (2018) Fear of falling in community – dwelling older adults: a cause of falls, a consequence, or both?. PLoS One 13(3).
-
Ambroise TL, Khan KM, Lord SR, Donaldson MG, Eng JJ, et al. (2006) Fall related efficacy independently in older women with low bone mass. J Gerontol A Biol Sci Med Sci 61(8): 832-838.
-
Kahle N, Tevald MA (2014) Core muscle strengthening’s improvement of balance performance in community dwelling elderly: a pilot study. J Aging Phys Act 22(1): 65-73.
-
Quiroz BC, Cagliari MF, Amorim CF, Sacco IC (2010) Muscle activation during four Pilates core stability exercises in quadruped position. Arch Phys Med Rehabil 91(1): 86-92.
-
Irez GB, Ozdemir RA, Evin R, Irez SG, Korkusuz F, et al. (2011) Integrating Pilates exercise into an exercise program for 65+ years old women to reduce falls. J Sports Sci Med 10(1): 105-111.
-
Hariprasad VR, Koparde V, Sivakumar PT, Varambally S, Thirthalli J, et al. (2013) Randomised clinical trial of yoga based intervention in residents from elderly homes: effects on cognitive function. Indian J Psychiatry 55(3): 357-363.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial